
Abstract
Background:
Middle ear (ME) pressure regulation has been suggested as a physiological mechanism that maintains pressure equilibrium between the ME and the ambient environment. This mechanism would be based on a complex sensorineural reflex loop composed of mechanoreceptors, an integrative center, and efferent neural pathways. Our aim was to demonstrate that hypoxic conditions, which would inhibit mechanoreceptors in general, similarly participate in the inhibition of the opening of the Eustachian tube (ET), and thus, to suggest that such receptors are involved in the overall regulation of ME pressure.
Materials and Methods:
Among 14 healthy volunteers, tubomanometry was performed in normoxia followed by hypoxia, and 3 parameters were evaluated for each ear under each condition, allowing the evaluation of the reactivity of the system: ET opening latency index (R), the Index of Velum Contraction (IVC), and the latency of pressure instauration (C2–C1).
Results:
Hypoxia induced a significant increase in the opening latency index of ET opening, without deleterious effects on the quality (IVC) and latency (C2–C1) of soft palate contraction.
Conclusions:
Our study supports the theory of a sensorineural reflex loop and provides evidence for the existence of mechanoreceptors, whose function is modified by changes in oxygen partial pressure, able to collect information on pressure variations between the ME and the external environment.
Introduction
Middle ear (ME) pressure regulation has been suggested as a physiological mechanism that maintains pressure equilibrium between the ME and the ambient environment, allowing for normal hearing. This function plays a key role in the pathophysiology of chronic ME diseases. A large number of hypothetical mechanisms for this regulation have been published in the literature. For some authors, ME pressure is governed by two passive mechanisms: the normal continuous mastoid gas absorption, which is counteracted by intermittent Eustachian tube (ET) openings (Doyle, 2017). For others, under physiological conditions, the opening of the ET behaves similar to a reflex mechanism (Gaihede et al., 2013; Martin et al., 2017). In this theory, permanent gas exchange occurs between the mastoid cavity, the ME mucosa, and the venous blood circulation, for gradual and slow pressure changes. The active opening of the ET allows for steep and fast pressure changes, under a reflex mechanism (Gaihede et al., 2010). The afferent neural pathways of this mechanism would contain afferents from mechanoreceptors found in the ME, the tympanic membrane, and the nasopharynx that collect pressure gradients between the ME and the ambient environment (Salburgo et al., 2016). The tympanic plexus, which contains afferents from the entire ME and the tympanic membrane and merging with the glossopharyngeal nerve, has been suggested to be involved in these afferent neural pathways.
Neurophysiological studies have clearly shown the existence of interactions between mechanosensitivity and chemosensitivity in different control systems (Somers et al., 1991; Cooper et al., 2004; Scruggs et al., 2016; Janssen et al., 2018). This was shown at the level of the arterial baroreceptors where endothelin-1 mediates an attenuation of carotid baroreceptor activity during intermittent hypoxia (Peng et al., 2012). Similarly, in skeletal muscles, hypoxemia markedly reduced the response of muscle spindles and Golgi tendon organs to mechanical stimulation in animal (Lagier-Tessonnier et al., 1993; Dousset et al., 2001) and human studies (Delliaux and Jammes, 2006).
Thus, we questioned the role of moderate hypoxia in healthy subjects on the control of the ET opening for the equalization of ME pressure. Should a link be proven between hypoxia and ET opening, then this would support the presence of mechanoreceptors, as described in other control systems. The findings of this study would surely have important implications on the development and understanding of the theory of a reflex mechanism governing the overall regulation of ME pressure.
Materials and Methods
Ethical considerations
The procedures were in accordance with the 1996 Helsinki Declaration, with Institutional Review Board approval. Written informed consent was obtained from all subjects.
Population
The study was conducted on 14 voluntary healthy subjects in a tertiary university referral center. All subjects underwent a full ENT examination before the study, including a tubomanometry (TMM). Exclusion criteria were the absence of ET opening on TMM, and any ENT, neurological, cardiac, or pulmonary diseases.
Tubomanometry
TMM is a clinical tool that allows the measuring of gas transport from the nasopharynx to the ME after ET opening (Esteve et al., 2001). The tubal opening latency index (R-value) reflects the latency between pressure application in the nasopharynx and the measurement of a pressure change in the ear canal in relationship to ET opening. This latency describes ET function: early opening (R ≤ 1), late opening (R > 1), or no opening (R not measurable). On the nasopharyngeal pressure curve of the TMM (Fig. 1), the C points represent the onset of sharp pressure increase in the nasopharynx (C1), the reach of the maximum pressure increase (C2), the end of the high pressure plateau where pressure begins to drop (C3), and the end of the peak where the pressure returns to baseline (C4). To evaluate the quality of soft palate isometric contraction, the Index of Velum Contraction (IVC) is measured in cm2/second by dividing the area of the zone found under the nasopharyngeal curve in cm2 by the duration of C3–C1 in seconds. The latency of pressure instauration (C2–C1), which is required to induce isometric contraction of the soft palate (velum), is calculated, normally <0.30 seconds. For each ear, these three parameters (R-value, IVC, and C2–C1) were recorded at three different pressure levels (30, 40, and 50 mbar).
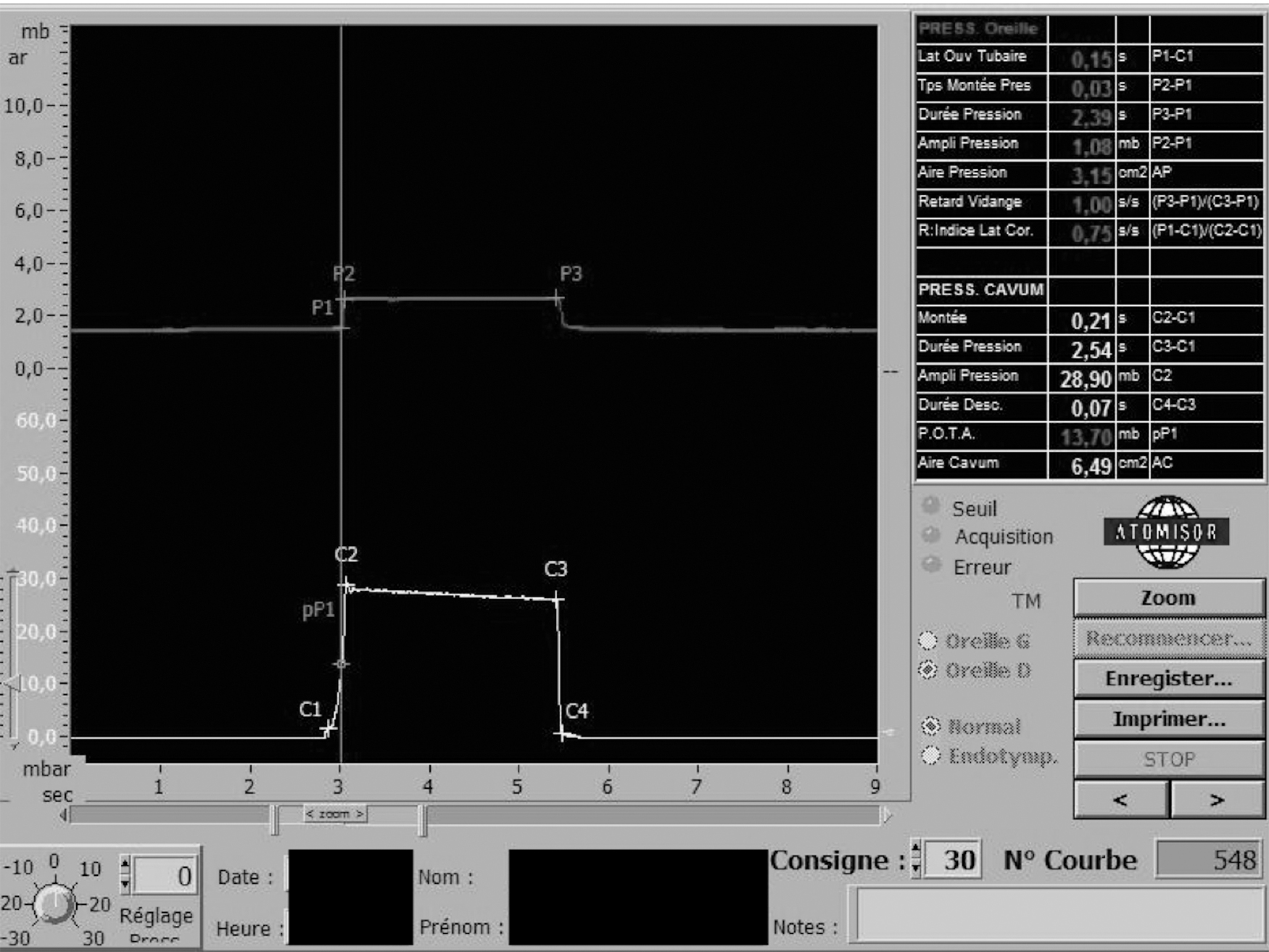
Illustration of a normal TMM chart (right ear, normal mode, intact tympanic membrane, and stimulus at 30 mbar). The top curve represents pressure variations in the EAM, and the bottom curve represents pressure variations in the nasopharynx. P1: ET opening; P2: end of the phase of pressure rise in the EAM; P3: closure of the ET; C1: start of the pressure rise in the nasopharynx; C2: target pressure achieved in the nasopharynx; C2–C3: phase of isometric soft palate contraction; C3–C4: phase of decline of pressure in the nasopharynx. EAM, external auditory meatus; ET, Eustachian tube; TMM, tubomanometry.
Normoxic and hypoxic conditions
Oxygen saturations were monitored by digital pulse oximeter (MasimoSET rainbow®). The first set of TMM recordings was performed in normoxic conditions under ambient air (FiO2 = 21%, SaO2 ≥98%). For the second set under hypoxic conditions, the patients were made to breathe in a Douglas bag carrying low levels of oxygen (FiO2 = 16%, i.e., a partial pressure of 0.16 bar). This resulted in an oxygen saturation below 95%, which was ensured by pulse oximetry monitoring over the entire period of the hypoxic TMM experiments.
Statistical analysis
A linear mixed-effects model was used to describe how the R-value is related to the following factors: condition (hypoxia/normoxia), pressure (30/40/50 mbar), and side (left/right). Estimation was carried out using the maximum likelihood method. The initial model contained all interactions between condition, pressure, and side. For the initial model, the optimal Box-Cox transformation was applied to obtain normality and variance homogeneity of errors. All model comparisons were based on F tests. Estimated means for the two conditions and the different pressure levels are presented together with confidence intervals computed using the bootstrap method. The data were analyzed using the R version 2.5.1, and the add-on package nlme version 3.1–80. All differences were considered statistically significant at p < 0.05.
Results
The study was conducted on 14 subjects, including 9 females and 5 males, with a mean age of 33 years (range 20–58 years). A total of 26 ears were investigated (exclusion of two ears by physiological no ET opening). Hypoxic conditions were obtained for each subject.
Opening latency index (R-value)
The R-value in normoxia is stable whatever pressure stimulation is used (Table 1 and Fig. 2). We report an increase in the mean R-value in hypoxia under all three pressure variations, which was statistically significant at 30 mbar (1.93 vs. 0.84, p < 0.0001) and 40 mbar (1.25 vs. 0.8, p < 0.0001), and not statistically significant at 50 mbar (0.78 vs. 0.71, p = 0.19). This increase in the R-value indicates a delay in ET opening in hypoxia.
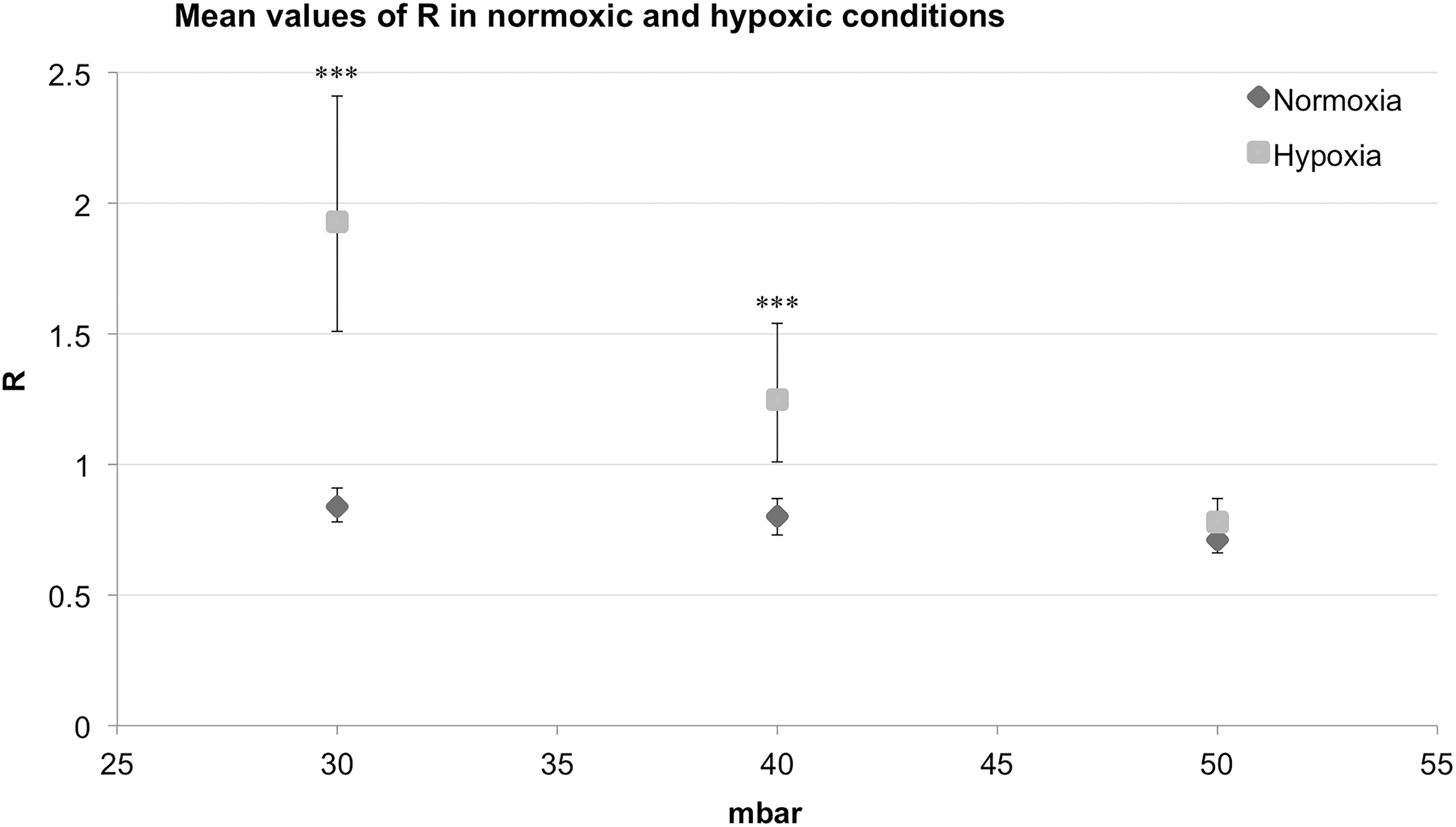
Chart representation of the mean values of the latency of ET opening (R) (along with the CIs as calculated by bootstrapping) in normoxic and hypoxic conditions, at 30, 40, and 50 mbar of pressure stimulation. Statistically significant findings are indicated with asterisks (***p < 0.001). CI, confidence interval.
Mean Values and Confidence Intervals of the Latency of Eustachian Tube Opening (R), the Index of Velum Contraction (IVC), and the Latency of Pressure Instauration (C2–C1) in Normoxic and Hypoxic Conditions at 30, 40, and 50 mbar of Pressure Stimulation
The italicized values indicate significance p-values.
CI, confidence interval; IVC, index of velum contraction; TMM, tubomanometry.
Index of velum contraction
The mean values of IVC showed a significant increase in the hypoxic condition at all three levels of pressure stimulation from 1.75 cm2/s in normoxia to 2.23 cm2/s in hypoxia (p = 0.0129), from 2.37 to 2.92 cm2/s (p = 0.0015), and from 2.95 to 3.79 cm2/s (p < 0.0001), at 30, 40, and 50 mbar, respectively (Table 1 and Fig. 3).

Chart representation of the mean values of the IVC (along with the CIs as calculated by bootstrapping) in normoxic and hypoxic conditions, at 30, 40, and 50 mbar of pressure stimulation. Statistically significant findings are indicated with an asterisk (*p < 0.05, **p < 0.01, ***p < 0.001). IVC, index of velum contraction.
Latency of pressure instauration (C2–C1)
We report no significant modification in the mean value of C2–C1 in hypoxia under all three pressure variations in comparison to normoxia (p = 0.69) (Table 1 and Fig. 4).
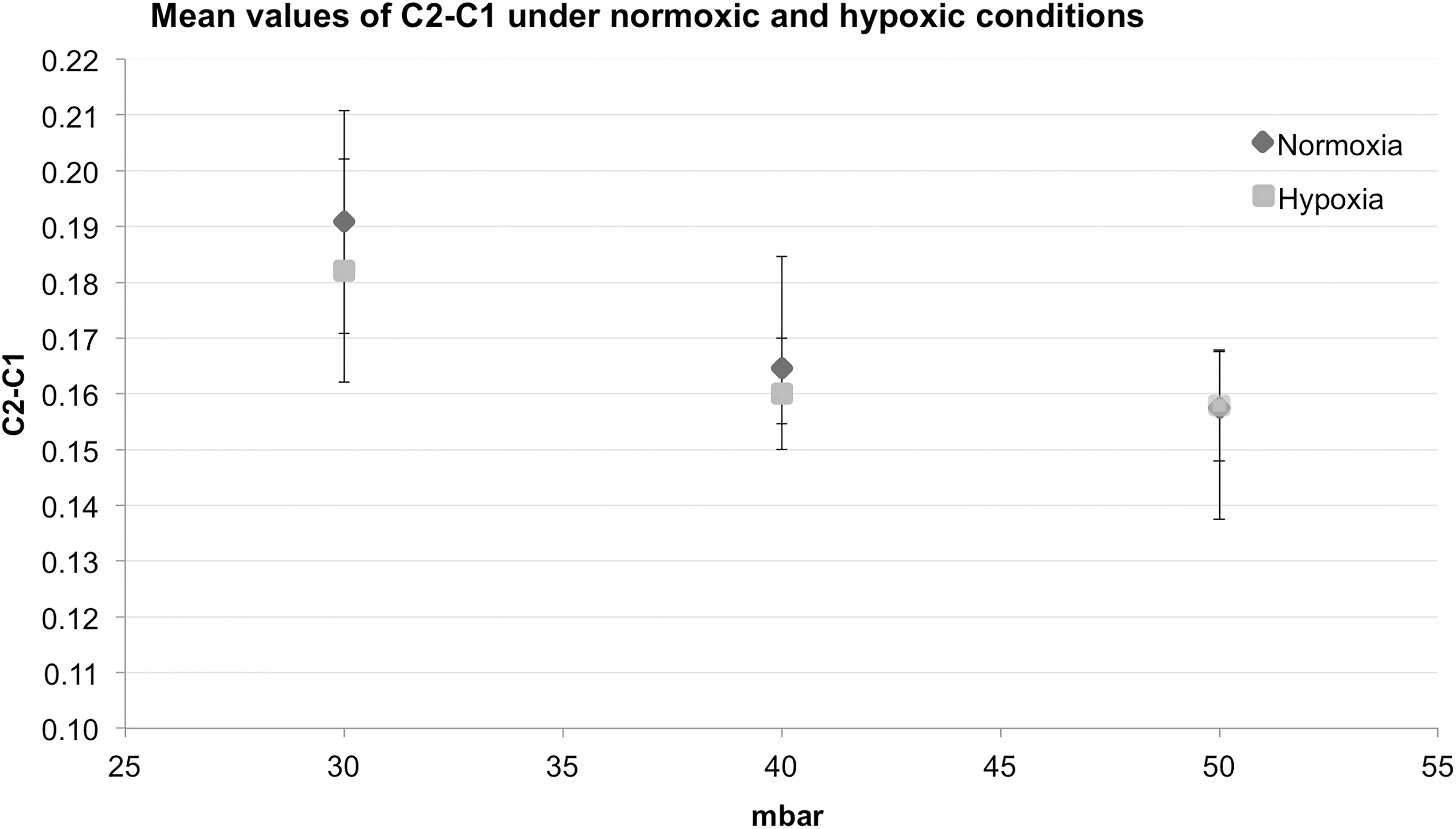
Chart representation of the mean values of the latency of pressure instauration (C2–C1) (along with the confidence intervals as calculated by bootstrapping) in normoxic and hypoxic conditions, at 30, 40, and 50 mbar of pressure stimulation.
Discussion
The major findings of this study were the modification of ET opening by hypoxia without any deleterious effect on the latency or quality of soft palate contraction. The aim of this study was to demonstrate the presence of mechanoreceptors that play a role in the opening of the ET, by demonstrating a loss of sensitivity of these receptors' reactivity in hypoxic conditions. This demonstration would provide similar evidence to that identified in other systems previously mentioned, such as the loss of carotid baroreceptor sensitivity in hypoxia (Peng et al., 2012). In fact, the peripheral effect of hypoxia seems to be identical to that identified by the application of local anesthesia on the mechanoreceptors, rendering them significantly hyposensitive to pressure changes (Nagai et al., 1989; Esteve et al., 2001).
ME pressure regulation has been suggested as a complex physiological mechanism. One of the aspects of this hypothesis is that ET opening is a reflex mechanism. In this theory, ME pressure regulation is based on a complex sensorineural reflex loop with peripheral barosensible starting points and an integrative center in the nucleus of the solitary tract of the brainstem (Eden et al., 1990). The efferent plexus would be composed of the tubal muscles and vascularization of the mastoid mucosa (Gaihede et al., 2010). The afferent plexus would be composed of mechanoreceptors in three locations: (1) in the ME, whose function is to collect endotympanic pressure (Gussen, 1970; Lim, 1970), (2) on the tympanic membrane (in the form of stretch receptors), especially on the pars flaccida, able to collect a pressure gradient between endotympanic and exotympanic pressures (Nagai and Tono, 1989), and (3) in the nasopharynx, especially the pharyngeal recess and the posterior nasopharyngeal wall, able to collect pressures of the upper aerodigestive tract, therefore reflecting atmospheric pressure (Guindi, 1981; Salburgo et al., 2016). While these structural elements may point to properties with afferent information in a neural feedback mechanism of ME pressure regulation, their detailed function is still unknown. In fact, ME Vater Pucinian-like structures are inconsistently found in autopsy materials. Furthermore, the pars flaccida seems to be involved in the monitoring of ME pressure gradient as it contains many nerve endings. However, it does not contain specialized nerve endings similar to those found on Vater Pucinian-like structures.
Under normal conditions, ET opening latency is stable no matter what pressure stimulation is used, but not under hypoxia (Fig. 2). Since the level of hypoxia in our study was only moderate, the significant rise of ET opening latency was obtained only for lower pressures (30 and 40 mbar, p < 0.0001), and the rise of this value was not significant for the highest pressure tested (50 mbar, p = 0.19). In fact, the stimulation at 50 mbar would generate a more efficient stimulus on the afferent pathways than at lower pressures, therefore triggering ET opening more rapidly, given that the level of hypoxia was moderate. We assume that, had the level of hypoxia been more severe, the R-value at 50 mbar would have been altered in a similar manner. This is also true for soft palate contraction. Moderate hypoxia had no deleterious effect on the quality (IVC) and latency (C2–C1) of soft palate contraction. In fact, a deleterious effect on muscle contractions would require a higher level of hypoxia to be demonstrated. This finding would, therefore, mean that the stimulus was constant in our experiment. That is, the increase of the R-value was directly in relationship to the level of hypoxia and was not due to any potentially deleterious modification of soft palate contractions.
The mean IVC increased in hypoxia under all three levels of pressure stimulation. We hypothesize that this increase could have been due to repetitive swallowing performed during TMM tests. This could have led to an elongation of the isometric phase of soft palate contraction under hypoxic conditions.
The main finding of our study was a significant modification of ET opening induced by hypoxia (i.e., increase of opening latency index) without any deleterious effect on the quality and latency of soft palate contraction. The function of ME pressure regulation was modified when oxygen partial pressure decreased, and these modifications could potentially promote ME barotraumas. These findings form a basis supporting the hypothesis of a sensorineural reflex loop.
Conclusion
ME pressure regulation is a complex and poorly understood phenomenon that requires physiological explorations. Our study has demonstrated that hypoxic conditions that inhibit mechanoreceptors in general, also inhibit the opening of the ET, and thus, it suggests that such receptors are involved in the overall regulation of ME pressure. The understanding of this complex system of ME pressure regulation would provide a better understanding of the pathophysiology of chronic ME diseases.
Footnotes
Acknowledgments
Our grateful thanks to Pr. Y. Jammes and Dr. D. Esteve for their gracious help.
Author Confirmation Statement
All authors have made substantial contributions to the conception and design of the study, acquisition of data, interpretation of data, and/or final approval of the version to be submitted.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this study.