
Abstract
This study was aimed at evaluating a potential association between blood pressure variation and acute mountain sickness (AMS) during acute exposure to normobaric hypoxia. A total of 77 healthy subjects (43 males, 34 females) were exposed to a simulated altitude of 4500 m for 12 hours. Peripheral oxygen saturation, heart rate, systemic blood pressure, and Lake Louise AMS scores were recorded before and during (30 minutes, 3, 6, 9, and 12 hours) hypoxic exposure. Blood pressure dips were observed at 3-hour mark. However, systolic blood pressure fell more pronounced from baseline during the initial 30 minutes in normobaric hypoxia (−17.5 vs. −11.0 mmHg, p = 0.01) in subjects suffering from AMS (AMS+; n = 56) than in those remaining unaffected from AMS (AMS−; n = 21); values did not differ between groups over the subsequent time course. Our data may suggest a transient autonomic dysfunction resulting in a more pronounced blood pressure drop during initial hypoxic exposure in AMS+ compared with AMS− subjects.
Introduction
Information on systemic blood pressure responses during acute exposure to high altitude is still scarce. Systemic blood pressure has previously been shown to increase during early exposure to high altitude, and thus during hypobaric hypoxia, especially at night (Bilo et al., 2011). In contrast, no or only a small decrease in systemic blood pressure was demonstrated at simulated high altitude (i.e., normobaric hypoxia during laboratory conditions) associated with a rise in heart rate (HR) and cardiac output and reduced peripheral resistance (Vogel and Harris, 1967; Winkler et al., 2017).
During the first minutes of hypoxia, a decrease in blood pressure might be evoked by adenosine triphosphate (ATP) from erythrocytes, which activates endothelial nitric oxide synthase (eNOS) and results in NO-dependent vasodilation (Kulandavelu et al., 2015). During more prolonged exposure (hours/days), sympathetic activation with rising noradrenaline levels and increasing firing of sympathetic nervous fibers becomes predominant, resulting in tachycardia and peripheral vasoconstriction, which leads to elevated systemic blood pressure (Parati et al., 2013, 2015). Although autonomic cardiovascular dysfunction seems to be associated with the development of acute mountain sickness (AMS) (Lanfranchi et al., 2005), the relationship between AMS and changes in systemic blood pressure during acute high-altitude exposure remains unclear.
Whereas Liu et al. (2014) demonstrated a relationship between blood pressure variation and AMS development at real high altitude, Winkler et al. (2017) found no such relationship during exercise in acute normobaric hypoxia. These authors suggested that hypertensive patients would not be at higher risk to develop AMS when acutely exposed to high altitude. Prediction of individual blood pressure response to acute hypoxia is complicated by the complex and temporarily changing interplay between chemoreceptor and baroreceptor activity (Marshall, 1998; Cooper et al., 2005). It is well documented that adrenergic drive (vasoconstriction) at acute high altitude is counterbalanced by peripheral direct effects of hypoxia (vasodilation). Therefore, in AMS, it could be a dysfunction in sympathetic system or in local vasodilation (endothelium or smooth muscle dysfunction) (Winkler et al., 2017).
To the best of our knowledge, no study evaluated the variation of systemic blood pressure concomitantly with manifestation of AMS during the early hours of acute exposure to hypoxia under standardized laboratory conditions. We hypothesized that such an association might exist and therefore monitored systemic blood pressure and AMS symptoms in a large sample of healthy subjects exposed to 12 hours of normobaric hypoxia.
Methods
Study participants
A total of 80 healthy subjects (43 males, 34 females; 3 dropouts; 18 to 45 years of age) volunteered to participate in the study (Table 1). Health status of participants was carefully checked before inclusion by a thorough medical examination. Exclusion criteria were any type of cardiovascular, respiratory, neurological, or psychiatric disease, permanent residence >1000 m, an overnight stay at altitudes >2500 m in the previous month, and exposure above 2500 m 2 weeks before the 12-hour hypoxic exposure. Three subjects did not fulfill inclusion criteria or were not able to perform hypoxia exposure due to lack of time. All participants provided written informed consent, and the study protocol was approved by the ethics committee of the Medical University of Innsbruck. For more detailed information, see Burtscher et al. (2014).
Baseline Characteristics of Male and Female Participants
Data are presented as mean ± standard deviation (age, body mass, BMI, height, SpO2, and HR) or median (interquartile range) (SBP, DBP, and MBP).
Significantly different between sexes.
BMI, body mass index; DBP, diastolic blood pressure; HR, heart rate; MBP, mean arterial blood pressure; SBP, systolic blood pressure; SpO2, peripheral oxygen saturation.
Hypoxia exposure
After routine medical examination, subjects were exposed to normobaric hypoxia (FiO2 = 12.6% equivalent to 4500 m) for 12 hours in the hypoxia chamber of the University of Innsbruck, situated 600 m above sea level. The hypoxia chamber was prepared with the desired FiO2 (12.6%) so that participants entered straight into the simulated altitude of 4500 m. Up to six participants were comfortably seated in the chamber.
They were free to walk, to read, or to listen to music. Subjects only performed very little physical activity probably not contributing to perception of fatigue. They were not allowed to leave the hypoxia chamber except, though, for going to the toilet, which was not the case during the first hour of exposure. Carbon dioxide concentration in the chamber (Low Oxygen Systems; Berlin-Buch, Germany) was continuously monitored by automatic flow regulation and remained below 0.1% at all times. Room temperature and humidity were kept constant at 22°C–24°C and 23%–27%, respectively. Water, juice, and fruits were freely available.
Measurements and AMS diagnosis
Peripheral oxygen saturation (SpO2), HR (by pulse oximetry; Onyx II 9550, NONIN), and systemic systolic blood pressure (SBP) and diastolic blood pressure (DBP) (M4 Plus; OMRON, Japan) were recorded after resting for at least 10 minutes in a sitting position at baseline, and after 30 minutes, 3, 6, 9, and 12 hours of hypoxia according to the American Heart Association recommendations (Pickering et al., 2005). Subjects were extensively familiarized with all measurements before taking baseline values.
Blood pressure measurements were then taken once at each time point and were only repeated if the device did not work properly. At the same time points, AMS scoring was performed using the Lake Louise scoring (LLS) system. The LLS is a self-assessment questionnaire considering five main symptoms (i.e., headache, nausea, dizziness, and fatigue; in the past also difficulty sleeping), each rated with a score from 0 to 3 (0 for no discomfort, 1 for mild symptoms, 2 for moderate, and 3 for severe symptoms) (Roach et al., 1993, 2018). “Difficulty sleeping” was not considered since participants did not stay overnight in the hypoxia chamber. AMS was diagnosed when headache was present together with at least one other symptom and when the total score was ≥3.
Statistics
Data were analyzed for normal distribution using the Kolmogorov–Smirnov test, and all but blood pressure measurements were normally distributed. Therefore, blood pressure is presented as median (interquartile range). Mean arterial blood pressure (MBP) was calculated as DBP + (SBP – DBP)/3. The Wilcoxon signed-rank test was used to compare blood pressure changes (deltas) within groups and the Mann–Whitney U test to compare deltas between study participants with AMS (AMS+) and without AMS (AMS−). Data of all other parameters are presented as mean (standard deviation), and paired and unpaired t-tests were applied to compare within- and between-group changes (deltas).
Spearman (blood pressure values) and chi-squared tests were applied for comparisons of frequencies. Correlations between AMS scores and changes in blood pressure, SpO2, and HR in hypoxia were calculated by partial correlation analyses (controlled for age, body mass index, and baseline values of MBP, HR, and SpO2). p-Values of less than 0.05 were considered to indicate statistical significance, which were corrected (Bonferroni) for multiple testing where applicable. All data analyses were conducted with the use of IBM SPSS Statistics 24 (IBM Corporation, Armonk, NY).
Results
Of the 77 subjects who actually participated in this study, the incidence of developing AMS (LLS ≥3) was 73%. More women were affected by AMS than men; however, this did not reach statistical significance (women to men is 82% to 65%).
In 22 participants, AMS symptoms became unbearable and they had to leave the chamber prematurely (3–6 hours: n = 3; 6–9 hours: n = 12; 9–12 hours: n = 7). Characteristics of participants are shown in Table 1.
Time course of hemodynamic responses to normobaric hypoxia is shown in Table 2.
Time Course of Hemodynamic Responses to Normobaric Hypoxia
n is reduced at later time points because some study participants left the hypoxia chamber due to severe AMS symptoms.
p < 0.05 versus baseline.
AMS, acute mountain sickness.
Changes in blood pressure, HR, and SpO2 during normobaric hypoxia were not significantly different between sexes; therefore, further analyses were performed on the whole study population. Moreover, based on information on menstrual cycle and contraceptive use, there was also no indication that female sex hormones may have affected presented findings.
As displayed in Table 2, SBP, DBP, and MBP all took a similar time course. During the first 3 hours, a highly significant decrease was observed (all p < 0.001) with the lowest values reached after 3 hours, followed by an increase back to baseline values after 9 and 12 hours of hypoxia. Variation of MBP in AMS− and AMS+ at baseline and after 3 hours in hypoxia is shown in Figure 1.

Box plots representing values of MBP at baseline (gray dotted boxes) and after 3 hours in hypoxia in subjects suffering from AMS (AMS+) and those free of AMS (AMS−), based on highest scores observed during the stay in the hypoxia chamber. AMS, acute mountain sickness; MBP, mean arterial blood pressure.
Highest AMS scores were used for categorizing AMS+ or AMS−. Only three subjects had their highest AMS scores before 6 hours of hypoxia exposure, those who left the chamber between 3 and 6 hours. Results remain unchanged when excluding these subjects.
Significant between-group differences in SBP were observed in AMS+ versus AMS− when values at baseline and after 30 minutes of hypoxia were compared (Fig. 2). No significant between-group (AMS+ vs. AMS−) changes occurred with regard to DBP and MBP (Table 3) and SpO2 and HR values.
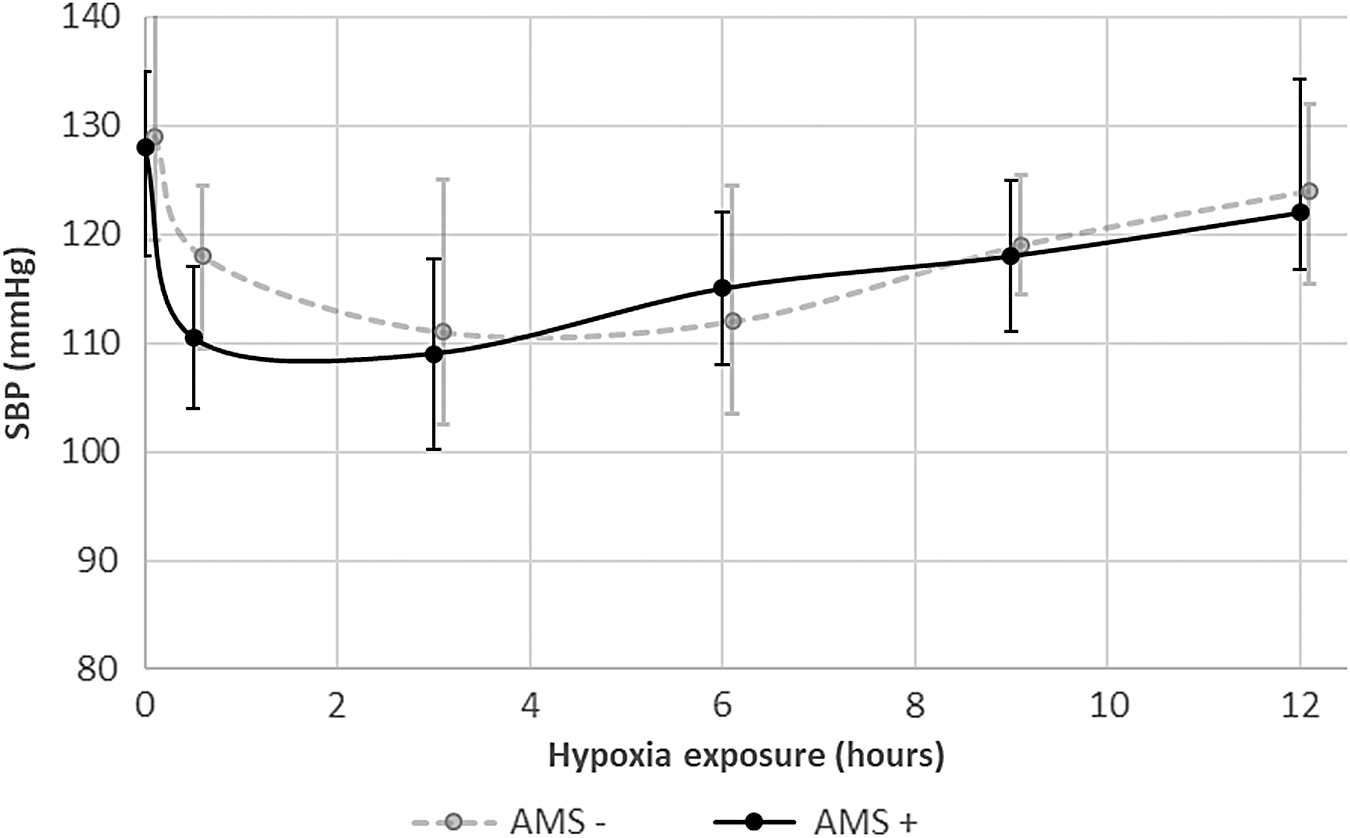
Time course of SBP in AMS+ compared with AMS− individuals during the 12-hour exposure to normobaric hypoxia. SBP, systolic blood pressure.
Time Course of Systemic Diastolic and Mean Blood Pressure in AMS+ Compared with AMS− Individuals During the 12-Hour Hypoxia Exposure
Data are presented as median (interquartile range) (DBP and MBP). There are no significant between-group differences.
Partial correlation analyses revealed that the highest individual AMS score of the overall group was correlated with SpO2 after 30 minutes of hypoxia exposure (r = −0.34, p < 0.05). In AMS− subjects, the decline of MBP during the first 30 minutes in hypoxia was correlated with the increase in HR (r = −0.42, p < 0.01), which was not the case for AMS+ (r = −0.19, p > 0.05).
Discussion
The main finding of this study is the differing time course of SBP during the first 3 hours in acute hypoxia between AMS+ and AMS−. Blood pressure dips were observed at 3-hour mark in hypoxia, but the initial drop in SBP was more pronounced in AMS+ than in AMS− individuals, suggesting a possible association between disturbed blood pressure control and subsequent AMS development. This is also supported by the potentially insufficient HR increase to compensate MBP decrease in AMS+. The significance of adequate autonomic cardiovascular regulation in the adaptation to hypoxia is also supported by a previous study where subjects treated with carvedilol (nonselective blocker of alpha and beta-adrenergic receptors) had lower BP during altitude exposure but also worse tolerance of high-altitude exposure (Bilo et al., 2011; Valentini et al., 2012).
The autonomous nervous system may respond differently in AMS+ and AMS− subjects during exposure to high altitude and thus hypoxia (Lanfranchi et al., 2005; Bernardi, 2007; Sutherland et al., 2017; Bourdillon et al., 2018). Indeed, differences in HR variability between AMS+ and AMS− individuals in response to normoxia (Sutherland et al., 2017), short-term normobaric hypoxia (Sutherland et al., 2017), and during ascent to high altitude have previously been observed (Kanai et al., 2001; Karinen et al., 2012).
Recently, Bourdillon et al. (2018) reported decreased baroreflex sensitivity in acute hypoxia contributing to impaired blood pressure control. Based on the more pronounced decline in SBP in AMS+ individuals in the present study, orthostatic intolerance to high altitude and thus hypobaric hypoxia might be expected in these subjects.
Although Mytton et al. (2008) showed a larger drop in SBP during orthostatic challenge at high altitude compared with sea level, this was not associated with AMS development. However, most blood pressure assessments in the studies mentioned above were performed with considerable delay (hours/days) after entering high altitude/hypoxia. Therefore, effects of short-term (minutes/hours) exposure to high altitude/hypoxia on systemic blood pressure responses and subsequent AMS development cannot be derived from those results (Kanai et al., 2001; Lanfranchi et al., 2005; Karinen et al., 2012; Liu et al., 2014).
Systemic blood pressure decline upon acute exposure to high altitude/hypoxia by hypoxia-related vasodilation is well known and may be counteracted by baroreceptor control (i.e., increase of HR, cardiac output, and vasoconstriction) (Mazzeo et al., 1991; Bernardi et al., 1998; Kanstrup et al., 1999; Bernardi, 2007; Mytton et al., 2008; Bourdillon et al., 2018). Thus, the most likely explanation for the more pronounced transient fall in SBP in AMS+ subjects may be insufficient vasoconstriction.
Limitations
Unfortunately, we did not include a control group and did not design the study to evaluate potential mechanisms responsible for blood pressure changes in acute hypoxia, representing the most important limitations. In addition, measurements were obtained during resting conditions in normobaric hypoxia and therefore results, including relatively mild AMS symptoms, should be verified in hypobaric hypoxia (i.e., exercising at high altitude). Moreover, BP was measured with an oscillometric device. However, the validity of these devices in hypoxic setting is unknown. However, shown differences in blood pressure responses between AMS+ and AMS− may at least be indicative of effects of the autonomic nervous system on AMS development and may stimulate future research.
In conclusion, our findings may suggest transient autonomic dysfunction in subjects who develop AMS when acutely exposed to hypoxia. If true, measures targeted to prevent this dysfunction might help prevent AMS development.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The study was funded by the Austrian National Bank (OENB) and the “Förderverein Sportmedizin,” Salzburg, Austria. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.