
Abstract
Gou, Qiling, Rufeng Shi, Xin Zhang, Qingtao Meng, Xinran Li, Xi Rong, Zhabu Gawa, Nage Zhuoma, and Xiaoping Chen. The prevalence and risk factors of high-altitude pulmonary hypertension among native Tibetans in Sichuan Province, China. High Alt Med Biol. 21:327–335, 2020.
Background:
Studies evaluating the prevalence and risk factors of high-altitude pulmonary hypertension (HAPH) are lacking.
Objective:
To determine the prevalence of HAPH and its correlated factors among highlanders living 3200 m above sea level in Ganzi Tibetan Autonomous Prefecture, Sichuan Province, China.
Methods:
This was a single-center, cross-sectional study involving 1129 subjects (mean age 46.6 ± 14 years, 39% men). In native Tibetans, HAPH was defined as a mean pulmonary artery pressure >30 mmHg as measured by transthoracic echocardiography.
Results:
HAPH had a crude prevalence of 6.2% and was more prevalent in men than in women (8.6% vs. 4.6%, p = 0.005). Elderly adults were more likely to develop HAPH than young adults (odds ratio [OR] = 5.308, 95% confidence interval [CI] = 2.562–10.993). Highlanders with HAPH had more severe metabolic abnormalities (including elevated blood pressure, blood glucose, blood lipids, BMI, etc., p < 0.05) and significantly increased hemoglobin and hematocrit levels (p < 0.01). In multivariate logistic regression analysis, independent risk factors for HAPH were metabolic syndrome (OR = 3.128, 95% CI = 1.110–8.818), age (>60 years vs. <40 years) (OR = 2.924, 95% CI = 1.282–6.669), and decreased Sp
Conclusion:
It could be concluded that HAPH was prevalent among 6.2% of native Tibetans in Sichuan Province, China. Increasing age, metabolic syndrome, and decreased Sp
Introduction
More than 140
A previous study related to HAPH revealed that it was a rare disease in highlanders, as the prevalence was 0.59% in native Tibetans dwelling in Qinghai Province, China (Wu, 1983). Later studies conducted in the Himalayas and South American plateau showed that the prevalence of HAPH ranged from 3.2% to 20% based on the different diagnostic methods and the diagnostic criteria applied (Aldashev et al., 2002; Xu and Jing, 2009; Negi et al., 2014). These studies indicated that HAPH may be a public health problem rather than a rare disease. Further research is highly necessary to determine whether the genetic backgrounds of native Tibetans protect them from HAPH or whether the prevalence of HAPH was underestimated.
History of HAPH and history of persistent excessive pulmonary vasoconstriction in response to hypoxia and hypoxia during sleep are risk factors of HAPH (Leon-Velarde et al., 2005). In addition, there are some controversial risk factors such as hemoglobin level and metabolic syndrome (Ge and Helun, 2001). Maggiorini and Léon-Velarde (2003) found a significant correlation between hemoglobin level and PAP in Han Chinese and Andean individuals. However, there are highlanders who have excessive polycythemia but not pulmonary hypertension (Tufts et al., 1985). It has been well documented that metabolic syndrome affects vascular endothelial and smooth muscle cell function in coronary artery, kidney, and peripheral vessels (Tesauro et al., 2011). However, there is less information regarding whether metabolic syndrome can alter pulmonary artery function, especially in high-altitude areas. This study was therefore designed to investigate the prevalence and predisposing factors of HAPH among native Tibetans in western China's Sichuan Province.
Methods
Study subjects
We carried out a cross-sectional study among residents in Luhuo county of Ganzi Tibetan Autonomous Prefecture, which has an average altitude of 3200 m. This investigation used a multistage, stratified, random-cluster sampling scheme. The number of villages was listed and selected using a random number table. A total of 1418 participants older than 18 years were recruited from different villages from January 2019 to September 2019. We excluded pregnant women, and those with congenital heart disease, severe heart valve disease, chronic obstructive pulmonary disease, interstitial lung disease, other lung diseases, mental health problems, malignant tumors, and severe hepatic or kidney failure. We ultimately included 1129 subjects. This research was approved by the Ethics Committee of West China Hospital, Sichuan University (Chengdu, China). The researchers guaranteed participants that their identities and answers would be kept confidential.
Data collection
Data were collected by investigators using a standardized questionnaire including age, sex, marital status, education, job, and cardiovascular risk factors. Peripheral oxygen saturation (Sp
Weight and height were measured to the nearest 0.2 kg and 1 cm, respectively. Body mass index was calculated as weight in kilograms divided by the square of the height in meters (kg/m2). Waist circumference (WC) was measured (accurate to 0.1 cm) midway between the bottom edge of the last rib and the iliac crest using a cloth tape directly touching the participant's skin. Hip circumference (HC) was measured at the level of the greater trochanter. The waist-to-hip ratio was calculated as WC divided by HC.
Transthoracic echocardiography was performed by a professional cardiologist using a Philips-CX50 color Doppler ultrasound system equipped with a 2.5 MHz adult transducer. Data were stored on DVD and analyzed by two investigators. The diameters of the left atrium (LA), right atrium (RA), left ventricle (LV), right ventricle (RV), interventricular septal thickness (IVS), left ventricular posterior wall (LVPW), and main pulmonary artery (MPA) were collected on the left ventricular long axis plane, left ventricular short axis plane, apex four-chamber view, apex two-chamber view, and apex three-chamber view. The Simpson method was used to calculate the left ventricular ejection fraction. mPAP was estimated using pulmonary artery acceleration time (PAAT) recorded at the right ventricular outflow tract (RVOT). When PAAT was >120 ms, mPAP was calculated using the formula mPAP = 79 − (0.45 × PAAT). When AT was <120 ms, mPAP was assessed using the formula mPAP = 90 − (0.62 × PAAT) (Rudski et al., 2010).
Laboratory measurements
Blood samples were obtained in the morning after at least 8 hours of overnight fasting. Biochemistry parameters including HGB, red blood cells, platelets, total cholesterol, triglycerides (TG), high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol, creatinine (Cr), uric acid (UA), and fasting plasma glucose (FPG) were measured in the laboratory of West China Hospital (Chengdu, China).
Definitions
Metabolic risk factors were defined according to the revised National Cholesterol Education Program ATP III criteria (2004) with a modification to the WC cutoff to be more appropriate for the Asian population. Metabolic risk factors were diagnosed using the following criteria: (1) elevated blood pressure: BP ≥130/85 mmHg or use of antihypertensive drugs; (2) abdominal obesity: WC ≥90 cm in men and ≥80 cm in women; (3) high TG level ≥1.69 mmol/L (150 mg/dL); (4) reduced HDL-C level <1.03 mmol/L (40 mg/dL) in men and <1.29 mmol/L (50 mg/dL) in women; and (5) high blood glucose: FPG level ≥5.6 mmol/L (100 mg/dL) or use of hypoglycemic medications. For analysis, the study subjects were categorized into three groups according to the metabolic risk factor clustering number: absent group (0 criteria), premetabolic syndrome group (1–2 criteria), and metabolic syndrome group (≥3 criteria) (Grundy et al., 2006).
Hypertension was defined as a systolic blood pressure (SBP) of at least 140 mmHg, a diastolic blood pressure (DBP) of at least 90 mmHg, and/or the use of antihypertensive medication. Normotension was defined as SBP <129 mmHg, and DBP <84 mmHg. Prehypertension was defined as BP between 139/89 and 130/85 mmHg, and grade 1 to 2 hypertension was defined as BP between 140/90 and 179/109 mmHg. Grade 3 hypertension was defined as SBP >180 mmHg and/or DBP >110 mmHg (Williams et al., 2018). Diabetes mellitus was diagnosed using the World Health Organization criteria: FPG of at least 7 mmol/L (126 mg/dL) and/or treatment for diabetes. Current smokers were defined as smoking at least one cigarette per day during the last year. Current drinkers were defined as having a least one drink in the 12 months. Education level was divided into four levels: 1, 2, 3, and 4 represented as illiteracy, primary school, middle school, and high school and higher, respectively. Obesity was defined as BMI >28 kg/m2, overweight was defined as BMI between 24 and 28 kg/m2, and normal weight was defined as BMI <24 kg/m2.
HAPH was defined as mPAP >30 mmHg at rest, moderate hypoxemia, with or without hypertrophy of the right heart and right heart failure, and absence of excessive erythropoiesis.
Statistics
The results are presented as mean (standard deviation). Statistical differences between groups were tested using analysis of variance, or Student's t-test. Categorical data were analyzed using the χ2 test or Fisher's exact test. Logistic regression analysis was used to identify risk factors for HAPH. The odds ratio (OR) and 95% confidence interval (CI) were estimated when appropriate. All statistical comparisons were two-tailed, and a p < 0.05 was considered to indicate statistical significance. All statistical analyses were performed using SPSS version 22.0.
Results
A total of 1418 native Tibetans were screened, of whom 59 were excluded because of poor quality of Doppler signals in the RVOT. A further 113 highlanders with cardiac diseases (coronary artery disease, congenital heart disease, hypertrophic cardiomyopathy, valvular heart disease, atrial fibrillation, and heart failure), 28 subjects with excessive erythrocytosis, and 89 subjects with lung disease (chronic obstructive pulmonary disease, post-tuberculosis fibrosis, and lung cancer) were excluded; finally, our study included 1129 residents in the Sichuan Tibetan region (Fig. 1).

The flow chart of the study. COPD, chronic obstructive pulmonary disease; HAPH, high-altitude pulmonary hypertension; RVOT, right ventricular outflow tract.
Prevalence of HAPH
Figure 2A provides the distribution of mPAP in our study cohort. The overall prevalence of HAPH, defined as mPAP >30 mmHg measured by Doppler echocardiography-derived PAAT, was 6.2% in the study cohort. Among the 1129 subjects, 183 had mPAP >25 mmHg corresponding to a 16.2% pulmonary hypertension (PH) prevalence. HAPH was more prevalent in male residents than in female residents (8.6% vs. 4.6%, p < 0.05). The prevalence of HAPH progressively increased with age (Fig. 2B).
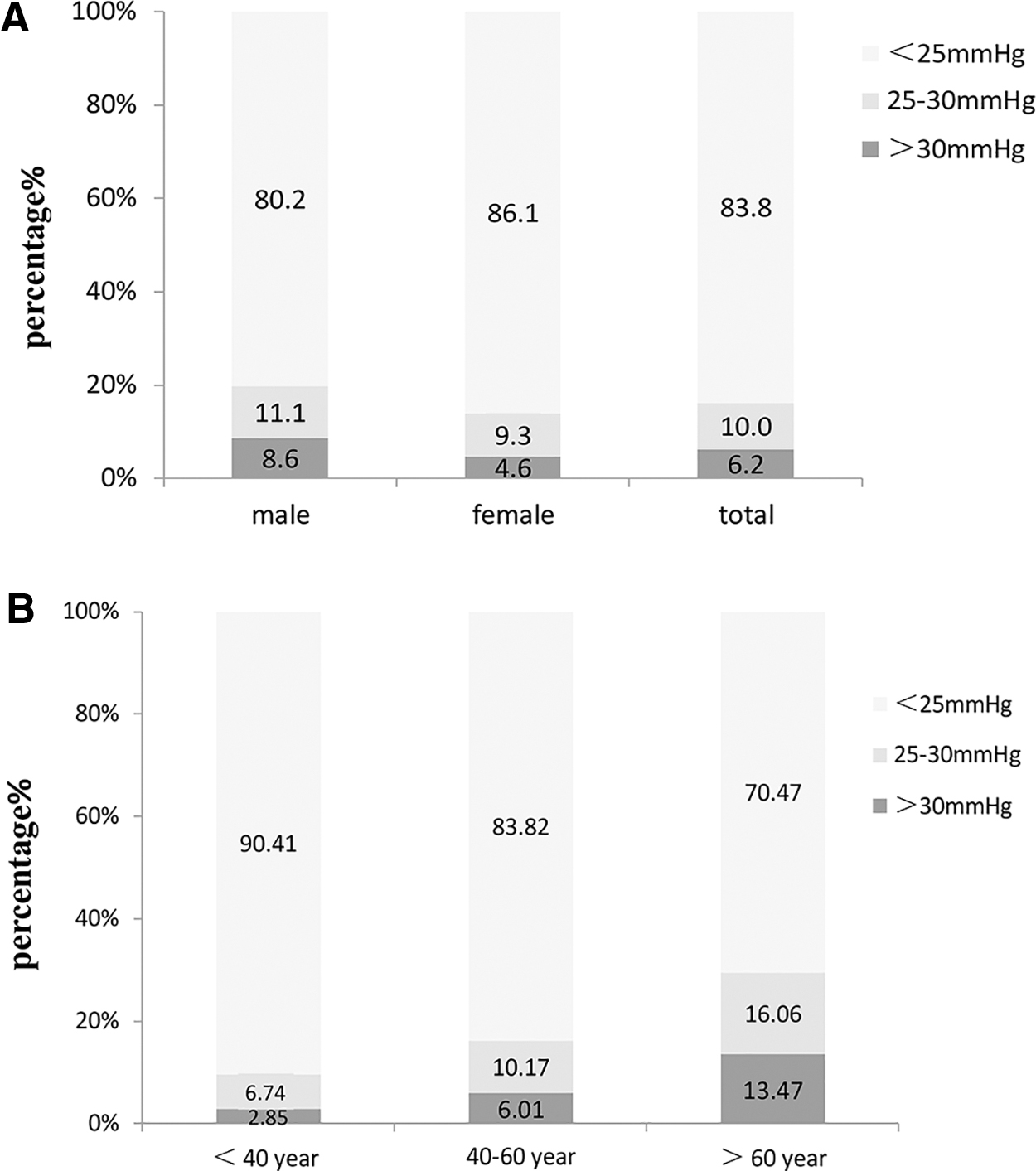
The percentage of different pulmonary artery pressure (<25, 25–30, and >30 mmHg) in three age groups (<40, 40–60, and >60 years) and in different genders.
Table 1 provides the baseline characteristics of residents with and without HAPH. Subjects with HAPH were older and more likely to be men and to have a higher HGB, HCT, and UA levels. Metabolic disorders such as hypertension, abdominal obesity, and dyslipidemia were more prominent in the HAPH group than in the control group. In addition, the levels of Sp
Demographic, Anthropometric and Biochemical Characteristics of Subjects Without and With High-Altitude Pulmonary Hypertension
Education level was assessed as illiteracy, primary school, middle school, or high school and higher for 1, 2, 3, 4. Metabolic risk factors included: (1) elevated blood pressure: BP ≥130/85 mmHg or taking antihypertensive drugs; (2) abdominal obesity: WC ≥90 cm in men and ≥80 cm in women; (3) high TG level ≥1.69 mmol/L; (4) reduced HDL-C level <1.03 mmol/L in men and <1.29 mmol/L in women; and (5) high blood glucose: FPG level ≥5.6 mmol/L or taking hypoglycemic medications.
p < 0.05.
BMI, body mass index; Cr, creatinine; DBP, diastolic blood pressure; eGFR, estimated glomerular filtration rate; FBG, fasting blood glucose; FPG, fasting plasma glucose; HAPH, high-altitude pulmonary hypertension; HC, hip circumference; HCT, hematocrit; HDL-C, high-density lipoprotein cholesterol; HGB, hemoglobin; HR, heart rate; LDL-C, low-density lipoprotein cholesterol; PLT, platelets; RBC, red blood cells; SBP, systolic blood pressure; TC, total cholesterol; TG, triglycerides; UA, uric acid; WC, waist circumference; WHR, waist-to-hip ratio.
Echocardiographic parameters in subjects with pulmonary hypertension
Table 2 shows that participants with HAPH had shorter PAAT than native Tibetans without HAPH (88 ± 9 vs. 129 ± 19, p < 0.000). The mPAP was 34 mmHg in the HAPH group and 18 mmHg in the control group. Subjects with HAPH had larger diameters of the RA and MPA. There were no significant differences between the two groups in parameters including the diameter of the LA, LV, IVS, LVPW, RV, and ejection fraction.
Echocardiographic Parameters Between High-Altitude Pulmonary Hypertension Patients and Without High-Altitude Pulmonary Hypertension Subjects
p < 0.05.
IVS, interventricular septal thickness; LA, left atrium; LV, left ventricular; LVEF, left ventricular ejection fraction; LVPW, left ventricular posterior wall; MPA, main pulmonary artery; mPAP, mean pulmonary artery pressure; PAAT, pulmonary artery acceleration time; RA, right atrium; RV, right ventricular.
Factors associated with HAPH
Bivariate logistic regression analysis showed that HAPH was positively related to age, number of metabolic risk factors, male sex, obesity, hypertension, hypoxemia, HGB, HCT, and UA levels. Furthermore, HAPH was negatively related to the Sp
Variables Related to High-Altitude Pulmonary Hypertension from Bivariate Logistic Regression Analysis
Metabolic risk factors included: (1) elevated blood pressure: BP ≥130/85 mmHg or taking antihypertensive drugs; (2) abdominal obesity: WC ≥90 cm in men and ≥80 cm in women; (3) high TG level ≥1.69 mmol/L; (4) reduced HDL-C level <1.03 mmol/L in men and <1.29 mmol/L in women.
p < 0.05.
CI, confidence interval; OR, odds ratio.
Factors with High-Altitude Pulmonary Hypertension from Stepwise Multivariate Logistic Regression
Adjusted for current smoking, snore, education, occupation, hypoxemia, BMI, WHR, eGFR, UA, HGB, RBC, diameter of RA and MPA.
p < 0.05.
Discussion
Our study demonstrated that a mean PAP of 19 mmHg was measured based on echocardiography in 1129 natives Tibetans living an average altitude of 3200 m, and the crude prevalence of HAPH was 6.2% for local residents in Luhuo County of Ganzi Tibetan Autonomous Prefecture, Sichuan Province, China, which was higher than that reported in a previous study conducted in another Tibetan ethnic area in Qinghai Province, China (Wu, 1983). This discrepancy may be caused by the variable sensitivity of different methods for screening PH. Electrocardiogram rather than echocardiography or right heart catheterization was used as a screening method to detect PH in previous research; however, studies revealed that electrocardiogram had insufficient sensitivity (20%–59%) to be a screening tool for PH (Kojonazarov et al., 2007). In this research, mPAP was assessed by the PAAT, the time from the beginning of right ventricular ejection to the peak velocity across the pulmonary valve, which had a sensitivity of 70% and specificity of 88% in adult PH detection (Kojonazarov et al., 2007).
A meta-analysis conducted by Soria et al. (2016) included 12 articles with a total of 834 high-altitude participants, and this study showed that a mean PAP obtained by echocardiography was 17.53 mmHg (95% CI = 16.74–18.39), which was slightly lower than our study (mean PAP ≈19 mmHg). In Soria et al. study, the age of the subjects ranged from 9.5 to 48 years, and 200 of 834 participants were children having a mean PAP of 15.8 mmHg. However, the age ranged from 18 to 84 years in our study, and the differences of mean PAP may be caused by the effect of age on PAP. In addition, In Soria et al. study, participants were recruited from general populations in one study, and the other 11 studies' subjects were healthy highlanders. However, all subjects in our study were recruited from general population, and the researchers' selective bias could contribute to this mild disparity.
Negi and colleagues did a cross-sectional study in a random sample of 1087 high-altitude general populations residing at an altitude of 3000–4200 m (Negi et al., 2014). Pulse Doppler signals recorded at RVOT were optimum for measurement of PAAT in 1021 subjects of 1087 subjects. The mPAP was higher than our study in case mean PAAT in their study was shorter than our study (119 ms vs. 126 ms). The difference could be caused by the positive influence of altitude on mPAP. In Negi's study, >70% subjects resided at an altitude of >3500 m; however, the average altitude in our study was 3200 m. In addition, Negi and colleagues did not exclude the subjects with erythrocythemia, which can possibly raise the PAP (León-Velarde et al., 2010).
In addition, there is growing evidence suggesting that mildly elevated mPAP ≈19–24 mmHg, which is below the traditional threshold of >25 mmHg used to define pulmonary hypertension at sea level, is associated with an increased risk of all-cause mortality (Maron et al., 2016; Kolte et al., 2018). The influence of mildly elevated mPAP on mortality on the high-altitude areas remains unclear. Our study found that 16.2% of residents had a mean PAP of >25 mmHg, whether this mild to moderate increase in PAP affects the occurrence and prognosis of HAPH needs to be further explored.
Our study was the first survey based on echocardiography to screen for HAPH in the Tibetan areas of western Sichuan, and it could be concluded that HAPH was not a rare disease although native Tibetans were most adaptable to high-altitude environments.
Long-term chronic hypoxia will lead to corresponding physiological changes for highlanders. Among them, relative polycythemia can increase the oxygen-carrying capacity of the body and improve hypoxia. However, excessive erythrocythemia will increase blood viscosity, which exerts a deleterious effect on tissue perfusion and aggravates tissue hypoxia. Chronic mountain sickness is a typical example (León-Velarde et al., 2010). In addition, hypoxic ventilatory response and hypoxic pulmonary vasoconstriction can increase ventilation, improve ventilation-to-blood flow ratio, and alleviate hypoxia. However, excessive hypoxic vasoconstriction can cause pulmonary vascular remodeling, resulting in HAPH (Maggiorini and Léon-Velarde, 2003; West, 2013).
The contribution of hemoglobin on HAPH remains unknown. Studies showed that the hematocrit and hemoglobin concentration were similar between the HAPH subjects and healthy highlanders. However, the level of Sp
The main reason for this difference may be that erythrocythemia was not excluded in Negi's study, which led to a significant increase in hemoglobin levels in the HAPH group. It can be inferred from our research that although there is an overlap of pathological mechanisms between HAPH and CMS, they are still two diseases with different pathological processes. For HAPH, the relationship between reduced Sp
There are few or no epidemiological studies related to the association between metabolic syndrome and PAP in highland hypoxic environments. Recent evidence has shown increases in metabolic syndrome on long-term high-altitude residents, where a higher BMI is related to lower oxygen saturation (Miele et al., 2016). In concordance with this, it has also been demonstrated that a strong association exists between BMI and HAPH subjects at altitudes between 4630 and 4905 m (Wu et al., 2007).
In this study, the prevalence of metabolic syndrome was more prominent in subjects with HAPH than in healthy highlanders (33.9% vs. 18.8%, p < 0.01), and after adjusting for the influence of age, sex, HGB, Sp
Advanced age was found to be an independent predictor of HAPH in our and Negi's studies (Negi et al., 2014). Snoring could be an indication of nocturnal hypoxia and there was no obvious difference in the percentage of snorers between the two groups (healthy native Tibetans vs. HAPH patients) in this study. However, hypoxemia during sleep was another significant risk factor in previous studies (Güvenç et al., 2016). Because of the lack of accurate assessment of nocturnal hypoxia in our study, the relevance between nocturnal hypoxia and HAPH needs to be further explored on the high-altitude areas. Our results demonstrated that the percentage of tobacco consumers in the HAPH group was higher than that in the control group (5.1% vs. 1.4%, p = 0.07). Previous studies also showed that smoking should play a significant role in HAPH. However, in multivariate regression analysis, there was no close association between smoking and HAPH in this research. This could be explained by the fact that smoking is forbidden for the majority of native Tibetans with religious beliefs.
Conclusion
HAPH as measured by echocardiography affected 6.2% of native Tibetans residing at an average altitude of 3200 m in western Sichuan Province, China. However, estimates may be higher in specific subgroups, especially in those older than 60 years of age. Metabolic syndrome was associated with HAPH independently of lung or heart diseases. For HAPH patients, interventions to decrease metabolic disorders may potentially protect subjects from pulmonary hypertension.
Limitations of the study
HAPH was diagnosed with noninvasive methods instead of right heart catheterization because of ethical reasons. Although measuring PAP based on tricuspid regurgitation velocity was the most recommended noninvasive method by the American Society of Echocardiography (ASE), because of its image quality, PAAT across RVOT was used as the criterion for the diagnosis of HAPH. Lung disease was excluded based on past medical records and clinical examination. Chest computed tomography should be performed to rule out other lung diseases. In our research, we excluded HFrEF and valvular diseases, but owing to lack of evaluation of left ventricular diastolic function and NT-proB-type natriuretic peptide, we could not totally exclude the HFpEF patients. Therefore, some patients with WHO group 2 PH may be mistaken for HAPH patients, which is also one of the limitations of this article.
Footnotes
Author Contributions
Dr. Chen has full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. All coauthors have reviewed and approved the article before submission. Q.G. and R.S. made equal contributions to this work. Study concept and design: Q.G., R.S., and X.C. Acquisition of data: Q.G., R.S., Z.G., and N.Z. Analysis and interpretation of data: Q.G., R.S., X.Z., Q.M., and X.C. Drafting of the article: Q.G., R.S., and X.C. Critical revision of the article for important intellectual content: X.Z., Q.M., and X.C. Statistical analysis: X.L. and X.R. Study supervision: Q.G. and X.C.
Acknowledgments
The authors thank the teams led by Zhabu Gawa at Luhuo County People's Hospital, Tibetan Autonomous Prefecture for their contributions to this study.
Author Disclosure Statement
The authors declare that they have no competing interests (financial, political, personal, religious, ideological, academic, intellectual, or any other) to declare in relation to this article.
Funding Information
This study was funded by a Science and Technology Pillar Programs in Sichuan Province (2017SZ0008). The funding body had no role in the design of the study, collection, analysis and interpretation of the data, or writing the article.