
Abstract
Zafren, Ken, Raimund Lechner, Peter Paal, Hermann Brugger, Giles Peek, and Tomasz Darocha. Induced hypothermia as cold as 3°C in humans: Forgotten cases rediscovered. High Alt Med Biol. 23:105–113.—The lowest temperature from which humans can be successfully rewarmed from accidental hypothermia is unknown. The lowest published core temperature with survival from accidental hypothermia is 11.8°C. We recently reported a rediscovered case series of patients in whom profound hypothermia was induced for surgery. The patient in this case series with the lowest core temperature, 4.2°C, survived neurologically intact. We subsequently rediscovered several additional case series of induced hypothermia to core temperatures below 11.8°C. In one case series, at least one patient was cooled to 3°C. We do not know if any patient survived cooling to 3°C. As in the previous case series, the authors of the additional reports presented physiological data at various core temperatures, showing wide variations in individual responses to hypothermia. These data add to our understanding of the physiology of profound hypothermia. Although induced hypothermia for surgery differs from accidental hypothermia, survival from very low temperatures in induced hypothermia provides evidence that humans with accidental hypothermia can be resuscitated successfully from temperatures much lower than 11.8°C. We continue to advise against using core temperature alone to decide if a hypothermic patient in cardiac arrest has a chance of survival.
Introduction
The lowest published core temperature from which a person with accidental hypothermia has been resuscitated with neurologically intact survival is 11.8°C in a 2-year-old boy who sustained an unwitnessed asystolic cardiac arrest (Darocha et al., 2020). The lowest published core temperature from which an adult has been resuscitated is 13.7°C (Gilbert et al., 2000). The patient was a 29-year-old woman who fell into an ice-covered stream while ski touring. She made a full recovery and was neurocognitively intact after rewarming, although she took many years to recover from severe peripheral sensorimotor polyneuropathy.
The lowest core temperature with neurologically intact survival from induced hypothermia has been previously widely quoted as 9°C (Niazi and Lewis, 1958). The patient was a 51-year-old woman with terminal ovarian cancer who was cooled by surface cooling using “rubberized blankets” with coolant at −1°C to −7°C, in an effort to treat the tumor. The attempt to treat the tumor with cooling was based on previously published data suggesting that hypothermia might be an effective method of debulking. No surgical procedure was performed. She made a full recovery from cooling but died 38 days later from complications of the malignancy. There was no evidence that hypothermia had affected the tumor.
We recently reported (Zafren et al., 2020) a rediscovered case series, published in 1961, of patients in whom profound hypothermia was induced for surgery (Stephen et al., 1961). The patient with the lowest core temperature, 4.2°C, survived neurologically intact. This is much colder than 9°C, the previously quoted lowest core temperature with survival from induced hypothermia (Niazi and Lewis, 1958). Four additional patients in this series survived neurologically intact after being cooled to core temperatures below 11.8°C (Stephen et al., 1961).
We have discovered seven more case series, published between 1959 and 1965, with induced hypothermia to core temperatures, either measured or estimated, below 11.8°C (Table 1). We also discovered a detailed case report of the patient in our previous article who survived neurologically intact after being cooled to a core temperature of 4.2°C (Woodhall et al., 1960). We found three additional cases from the late 1950s of patients who were cooled to esophageal temperatures of 4°C (Sealy, 1984), about 6°C (Sealy et al., 1959), and 9.3°C (Young et al., 1959). One patient was presented in a case report (Young et al., 1959) and also included in a case series (Sealy et al., 1959). The other two cases were reported only graphically (Sealy et al., 1959; Sealy, 1984).
Case Series and Case Reports with Induced Hypothermia to Core Temperatures, Either Measured or Likely, Below 11.8°C
Nasopharyngeal temperatures from 13°C to 15°C very likely correspond to esophageal temperatures below 10°C.
One patient was cooled to a brain temperature of 16.5°C, likely corresponding to Tes ≤9.5°C.
Tes, esophageal temperature; Tnp, nasopharyngeal temperature.
As in the previous case series (Stephen et al., 1961), the authors of the additional reports presented cardiovascular and other physiological data at various core temperatures. These data included heart rates at various temperatures, threshold temperatures for ventricular fibrillation (VF), effects on the central nervous system (CNS), and temperature measurements at various anatomic sites.
We also discovered review articles, based on experiences with induced profound hypothermia for surgery (Clowes, 1960; Hickey et al., 1962; Nealon and Gosin, 1965). These articles provided useful background on the techniques used in the cases and case series as well as additional physiological observations.
Case Report: Patient Cooled to 4.2°C
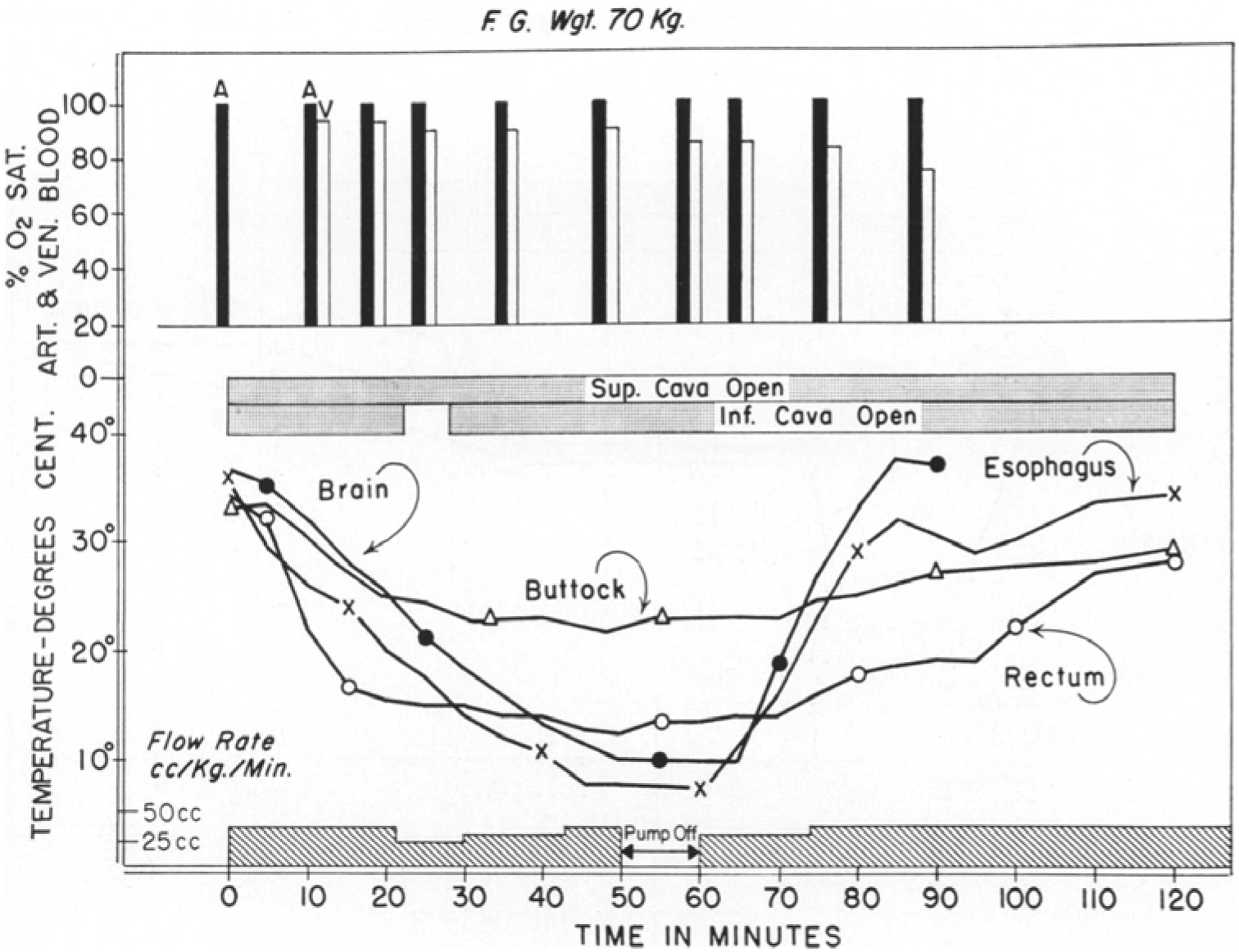
A 39-year-old man, patient 48 in the case series (Stephen et al., 1961) we described in our previous paper (Zafren et al., 2020), presented with bifrontal headaches for 3 months with cognitive deterioration, ataxia, and anorexia (Woodhall et al., 1960). An asymptomatic pulmonary mass was identified by arteriography. The patient underwent cooling for subtotal removal of an apparent single brain metastasis with the secondary goal of studying the effect of profound hypothermia on the inoperable lung carcinoma. Temperatures were measured in the blood inflow, cerebral cortex, esophagus, pharynx, rectum, and peripheral muscle (Fig. 1). The patient was cooled using cardiopulmonary bypass (CPB) and a heat exchanger. He made an “uneventful recovery” after being rewarmed from a core temperature of 4.2°C, measured in the mid-esophagus.

Course of blood inflow, cerebral cortex (brain), esophageal, pharyngeal, rectal, and peripheral muscle temperatures in induced hypothermia. Nadir of esophageal temperature was 4.2°C (Woodhall et al., 1960).
Case Known Only from a Figure: Patient Cooled to About 5°C
We discovered a figure in a review article (Sealy, 1984), showing time series data of a 44-year-old patient who underwent cooling to an esophageal temperature of about 5°C for surgical repair of a cerebral aneurysm (Fig. 2) (Sealy, 1984). As far as we know, this case was never included in a published case series or case report. The figure shows that the patient survived for at least 2 hours after being rewarmed. Further information was not available.

Course of esophageal, brain, rectal, and muscle temperatures in induced hypothermia. Nadir of esophageal temperature was about 5°C (Sealy, 1984).
Case Series
In the first additional case series (Sealy et al., 1960), we found what is most likely the lowest recorded core temperature from induced hypothermia in a human. In a series of 36 patients of whom 33 patients were operated for intracardiac defects and 3 patients for neurological diseases, at least 1 patient was cooled to 3°C (Sealy et al., 1960). Nadir temperatures ranged from 3°C to 22°C, measured in the mid-esophagus. Unfortunately, the authors gave no details about individual patients, including outcomes. The specific indications for surgery, age, sex, and other characteristics of the patient or patients cooled to 3°C were also not described. The overall mortality was 30%. The authors stated that no deaths or complications could be attributed to perfusion or hypothermia. An exhaustive search for a case report of the patient or patients cooled to 3°C failed to yield any further information.
In our previous paper, we reviewed a case series of 50 patients with survival after hypothermia to as low as 4.2°C (Stephen et al., 1961). Hypothermia was induced for cardiac surgery in 47 patients and for brain surgery in 3 patients. It is possible that 33 of the patients who had heart surgery and the 3 patients who had brain surgery had been previously reported in the case series in which at least 1 patient was cooled to 3°C (Sealy, 1960), but we cannot be sure because the older case series gave no information about individual patients (Sealy et al., 1960).
In the second case series, six adult patients who underwent surgery after intracranial aneurysmal hemorrhage were cooled using cooling blankets followed by circulatory bypass to esophageal core temperatures ranging from 5°C to 7°C (Patterson and Ray, 1965). Four patients, with core temperatures from 5°C to 6.5°C, survived neurologically intact. Two died from complications of the brain surgery rather than from hypothermia. A seventh patient was also operated, but the lowest esophageal temperature was not reported (Table 2).
Case Series of Seven Patients Cooled to Esophageal Temperatures ≤7°C, Showing Esophageal Temperatures, Brain Temperatures, and Outcomes
Patterson and Ray (1965).
Tbrain, brain temperature; Tes, esophageal temperature.
In the third additional case series of 21 patients who underwent induced “deep hypothermia” for intracardiac surgery, 16 recovered (Gordon et al., 1960). Core temperatures were measured in the esophagus. The lowest core temperature was 8°C. Each patient was cooled to a target core temperature that depended on the anticipated length of surgery, with lower core temperatures for longer surgeries. The authors documented a few details about individual patients, other than the diagnoses.
Four of the five patients who died regained consciousness after surgery and appeared to be neurologically intact. Three of the five patients who died had cyanotic tetralogy of Fallot. Two of these three regained consciousness. One of the remaining patients died 12 hours after surgery as the result of a technical error; the closure of the aorta obstructed the orifice of the right coronary artery. The other died from aspiration 3 days postoperatively.
In the fourth additional case series, seven patients were cooled by extracorporeal circulation to esophageal temperatures of 9°C–20°C for cardiac surgery (Sealy et al., 1959). Six of the patients were children (11-months to 6-years-old). There were four survivors, all children, including a 4-year-old patient cooled to 9°C. The other patients were cooled to 14°C–20°C. The three deaths, including one adult patient (32-year-old), were caused by complications of the surgery rather than by hypothermia. The 7 patients seem to have been a subgroup of a larger series of 95 patients that the authors mention in the paper, who underwent intracardiac operations using extracorporeal circulation with a heat exchanger.
The authors present the diagnoses and outcomes by diagnosis, but not the lowest esophageal temperatures. Of the 95 patients, 79 (83%) survived. The authors also present a figure showing data from a 70 kg patient who was cooled to an esophageal temperature of about 6°C for an operation on an extracardiac lesion (Fig. 3). Based on the figure, this patient survived for at least 30 minutes after rewarming. The authors gave no further information about this patient, who was not included in the larger series of 95 patients. We also found a case report and time-series figure of a 5-year-old girl who was cooled to an esophageal temperature of 9.3°C for repair of a severe tetralogy of Fallot (Young et al., 1959).
Course of esophageal, brain, rectal, and muscle temperatures in induced hypothermia. Nadir of esophageal temperature was about 6°C (Sealy et al., 1959).
She recovered without complications. Her case was also presented in more detail in a review article (Sealy, 1984). She may have been the same patient as the 4-year-old cooled to 9°C in the case series of seven patients. The details of the cases were the same, although the ages were reported to be different (Sealy et al., 1959).
The fifth additional case series involved 10 patients cooled with CPB to esophageal temperatures of 9.6°C–16.8°C for repair of ruptured intracranial aneurysms (Drake et al., 1964). Six of the patients were cooled to esophageal temperatures of 12.5°C or lower. All patients survived the operation. There were three postoperative deaths that the authors characterized as resulting from extracorporeal circulation, two from hemorrhage (at 5 and 18 hours) and one critically ill patient from “poor perfusion” after 6 days. Two patients with high-grade aneurysms remained neurologically unchanged and died months later.
Only three patients had “excellent results.” Two patients were “disabled,” one moderately and one severely. The authors ascribed the high morbidity and mortality to the large size and high-risk locations of the aneurysms and to early operation in eight patients, before arterial spasm and brain swelling had resolved.
In the sixth additional case series (Drew and Anderson, 1959), the authors reported three cases of induced hypothermia in cardiac surgery with nasopharyngeal temperatures as low as 13°C (Drew and Anderson, 1959). In one case, the nasopharyngeal temperature was lower than 20°C in a 12-month-old male. The child died, because the severe intracardiac defect could not be repaired. The other two patients made full neurologic recoveries. The first was a 4-year-old male cooled to a nasopharyngeal temperature of 15°C. The second, a 2.5-year-old male, was cooled to a nasopharyngeal temperature of 13°C.
The seventh additional case series, a later case series by one of the authors of the sixth case series, reported that 90 more patients with cardiac abnormalities had been cooled with cardiac bypass to nasopharyngeal temperatures as low as 10°C in two patients (Drew, 1961). The other 88 patients were cooled to nasopharyngeal temperatures of 13°C–15°C. The author provided no further details of individual patients.
All the patients in the last two case series cooled to nasopharyngeal temperatures (very close to brain temperatures) at or below 15°C likely had esophageal temperatures that were below 10°C. We have presented data (discussed later in the Sites of Temperature Measurement and Temperature Gradients section) that shows the gradients between esophageal and brain temperatures.
Physiologic Observations
Respiratory effects
In most of the case series, there were no data regarding the respiratory effects of hypothermia because ventilation was controlled. In one case series with assisted ventilation, respirations in one patient stopped during cooling at an esophageal temperature of 20°C and resumed during rewarming at an esophageal temperature of 17°C (Patterson and Ray, 1965). In another case series, spontaneous respiration resumed in one patient during rewarming at a nasopharyngeal temperature of 22°C. (Drew and Anderson, 1959).
Cardiovascular effects
The heart rate usually slowed progressively with cooling until the rhythm deteriorated spontaneously to asystole or VF, followed by asystole. During rewarming, the heart reverted to sinus rhythm or to VF and then sinus rhythm, either spontaneously or with electrical cardioversion. (Drew and Anderson, 1959; Sealy et al., 1960; Drew, 1961; Stephen et al., 1961; Patterson and Ray, 1965; Sealy, 1984). Other rhythms, including sinus bradycardia and various degrees of heart blocks, also occurred during cooling and rewarming (Niazi and Lewis, 1958; Drew, 1961). In one case report, there was a slow idioventricular rhythm during cooling and rewarming, rather than VF (Niazi and Lewis, 1958).
CNS effects
Because the patients were anesthetized, only electroencephalograms (EEGs) and neurologic outcomes could be used to evaluate the effects of hypothermia on the CNS. In one series of 21 patients cooled to between 8°C and 21°C, the EEG was normal before and after surgery in all patients (Gordon et al., 1960). When the EEG was monitored during induced hypothermia, it became isoelectric, depending on the series, at 16°C–20°C (Gordon et al., 1960), below 20°C (Niazi and Lewis, 1958), between 14°C and 20°C (Stephen et al., 1961), and about 20°C (Drew, 1961). In one study, the EEG remained isoelectric until 20°C during rewarming (Drew, 1961). In the case report of the patient cooled to 4.2°C, the EEG became isoelectric during cooling at a core temperature of 22°C (Woodhall et al., 1960).
The patient, previously reported, who was cooled to 4.2°C, made an “uneventful recovery” (Stephen et al., 1961). In the series of 50 patients we originally reported, 30 patients woke up and did not die within 17 days of the operation (Stephen et al., 1961). None had evidence of cerebral injury. In the series of seven patients operated for intracranial aneurysms, five made full recoveries; two died from complications of the brain surgery (Patterson and Ray, 1965). In the series of 21 patients cooled to 8°C–21°C for intracardiac surgery, all patients except one regained consciousness postoperatively and were “lucid” with normal reflexes (Drew, 1961).
The patient who was cooled to 9°C became conscious 10 hours after being rewarmed to normal body temperature. Her mental condition and intelligence were reportedly unchanged (Niazi and Lewis, 1958). In three patients who underwent profound hypothermia for cardiac surgery, one died from a severe intracardiac defect that could not be repaired. The other two patients, a 4-year-old male and a 2.5-year-old male, made full neurologic recoveries (Niazi and Lewis, 1958). In the later series of 90 patients with profound induced hypothermia, the author found “no evidence of cerebral damage which certainly could be attributed to the long period of circulatory and respiratory arrest…” (Drew, 1961).
Sites of temperature measurement and temperature gradients
As in accidental hypothermia, core cooling by extracorporeal circulation can cause large temperature gradients between different parts of the body. Esophageal temperature, measured in the lower third of the esophagus, is the best reflection of core temperature, but brain temperature is the main factor limiting safe low-flow or no-flow time during surgery with decreased perfusion or cardioplegia.
Brain temperature in induced hypothermia is characteristically warmer than esophageal temperature (Sealy et al., 1959; Woodhall et al., 1960; Stephen et al., 1961; Sealy, 1984). In the patient cooled to 4.2°C, when a thermistor was inserted 2 cm below the cortex during cooling it registered 18°C. The brain eventually cooled to 11°C (Fig. 1) (Woodhall et al., 1960). In the 44-year-old patient cooled to an esophageal temperature of about 5°C, the lowest brain temperature was about 13°C (Fig. 2) (Sealy, 1984). In the 70 kg patient cooled to an esophageal temperature of about 6°C, the lowest brain temperature was about 9°C (Fig. 3) (Sealy et al., 1959).
In one case series, the lowest brain temperatures (14°C–17°C) were 7°C–11.5°C warmer than the lowest esophageal temperature (5°C–7°C) (Table 2) (Patterson and Ray, 1965). In the 46-year-old patient from the case series (Stephen et al., 1961) we reported in our previous paper (Zafren et al., 2020), the lowest esophageal temperature was 9°C and the lowest brain temperature was about 10°C (Fig. 4).
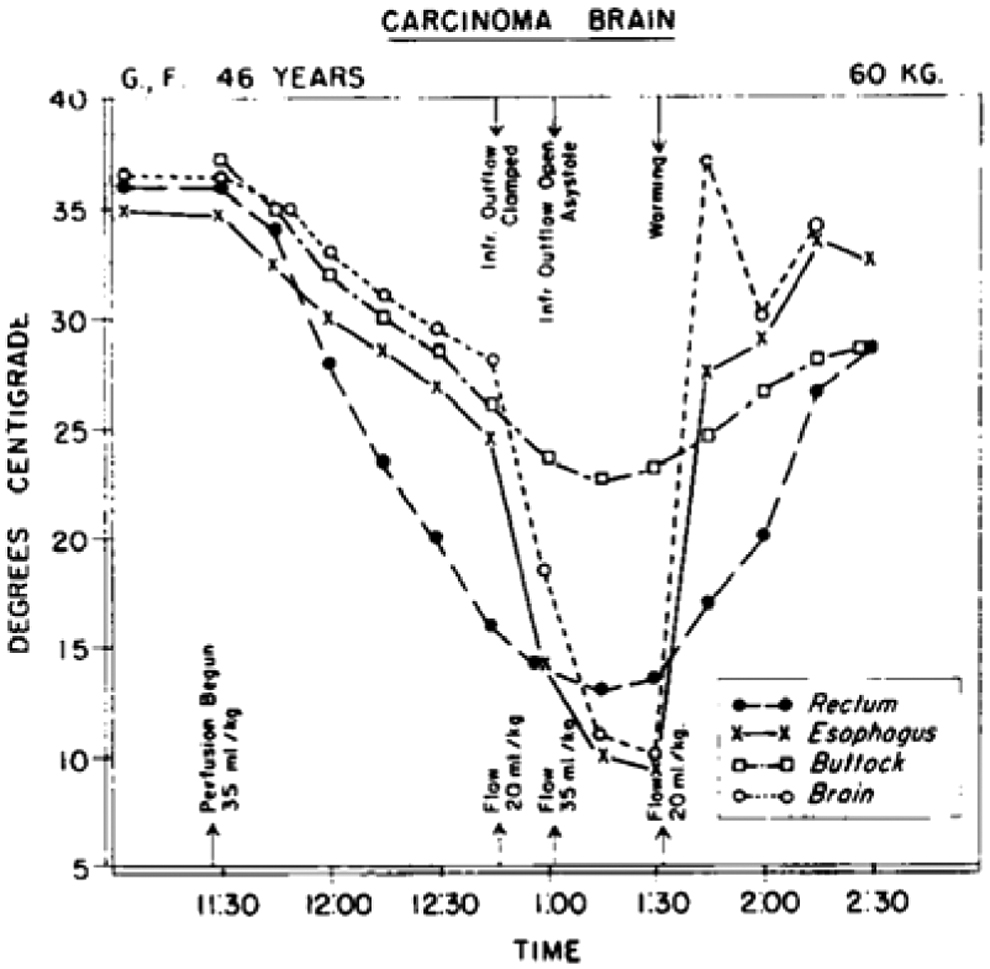
Course of esophageal, brain, rectal, and muscle temperatures in induced hypothermia. Nadir of esophageal temperature was 9°C (Stephen et al., 1961).
In most reported cases, brain temperature lags behind esophageal temperature during extracorporeal cooling and rewarming. In the 39-year-old man cooled to an esophageal temperature of 4.2°C, the nadir of brain temperature (11°C) was about 8 minutes later than the nadir of esophageal temperature (Fig. 1) (Woodhall et al., 1960). In the 44-year-old man cooled to about 5°C, the nadir of brain temperature (about 13°C) was about 5 minutes later than the nadir of esophageal temperature (Fig. 2) (Sealy, 1984).
In both cases, the brain temperature increased more slowly than the esophageal temperature during rewarming. In the 70 kg patient cooled to an esophageal temperature of 6°C, the brain temperature lagged behind the esophageal temperature by a few minutes during cooling but increased at about the same rate as esophageal temperature during rewarming (Fig. 3) (Sealy, 1984). In the 46-year-old man from the case series we reported in our previous paper, the brain temperature rose and fell at a rate similar to that of esophageal temperature (Fig. 4). The esophageal and brain temperatures reached their nadirs (9.0°C and about 10°C) at nearly the same time after cooling (Stephen et al., 1961).
There were outliers in the study of 10 patients cooled for treatment of ruptured intracranial aneurysms. The temperature of the cerebral cortex was measured in two of the patients. In one patient, the nadir of the cortex temperature was 10°C at an esophageal temperature of 11°C. In the other patient, both nadir cortical temperature and esophageal temperature were 12.5°C (Drake et al., 1964). The relatively high brain temperatures in these two cases, compared with most of the reported cases, were likely artifacts of the extracorporeal technique (femerofemoral cannulation), with lower blood flows than those currently used.
Rectal temperature generally lags behind esophageal temperature during cooling and does not go as low as esophageal temperature. During rewarming, rectal temperature usually increases more slowly than esophageal temperature (Figs. 2–4) (Sealy et al., 1959; Stephen et al., 1961; Sealy, 1984).
To better understand the dynamics of brain cooling and rewarming, it would be useful to know the in-flow blood temperature during CPB. This was reported, graphically (Fig. 1), in only one study (Woodhall et al., 1960). One other article mentioned that the gradient between perfusing blood and core (esophageal) temperature was not more than 12°C (Drake et al., 1964). Another factor in the dynamics of brain cooling and rewarming was the use of low-flow, low-pressure CPB perfusion. The majority of studies reported the use of low-flow perfusion, often interspersed with periods of total circulatory arrest, ranging from 2 minutes to 1 hour.
Complications
Mortality was high in some of the case series we studied but was most often related to the underlying conditions. In the case series of 36 patients cooled to 3°C–22°C (Sealy et al., 1960), the authors reported that the high mortality (30%) resulted from their inability to correct complicated cardiac anomalies. They specifically stated that no deaths or complications could be attributed to extracorporeal circulation or to profound hypothermia.
In the case series we previously presented (Stephen et al., 1961), six patients were cooled to 11.8°C or below for cardiac surgery; two of the six died on the table from cardiac failure. One patient cooled to 9.0°C for brain surgery never awoke and died 4 months postoperatively. Another patient cooled to 6°C for brain surgery died on the table of hemorrhage from cerebrovascular abnormalities. In the case series of seven patients cooled to core temperatures 5°C–7°C for brain surgery, five patients made full recoveries, while two died from complications of the brain surgery (Patterson and Ray, 1965).
In the case series of seven patients cooled to esophageal temperatures of 9°C–20°C for open heart surgery, six of the patients had core temperatures 14°C–20°C (Sealy et al., 1959). Three patients, including the patient cooled to 9°C, died. The causes of death were surgical complications, rather than hypothermia. In a case series of three patients undergoing cardiac surgery with nasopharyngeal temperatures of 13°C–15°C, one patient died because of a “severe intracardiac defect” that could not be completely repaired. The other two patients made full recoveries (Drew and Anderson, 1959).
In the case series of 90 patients cooled to a nasopharyngeal temperature of 15°C for cardiac surgery, two adult patients had slight confusion postoperatively that resolved in a few days and three patients (ages 8-, 10-, and 12-year-old) developed brainstem damage starting 36 hours to 4 days postoperatively (Drew, 1961). Delayed brain damage may have been caused by hypothermia, but it was unlikely to have been related to circulatory and respiratory arrest. The author used a different technique than other cardiac surgeons before or since.
Using the patients' own lungs rather than an extracorporeal oxygenator, he drained blood from the systemic veins and reinfused it into the pulmonary artery, then drained the pulmonary venous atrium (usually the left), and reinfused the blood into the systemic arterial circulation. This may have caused less inflammation than oxygenators available at the time and therefore less cerebral edema.
Past and Present Levels of Induced Profound Hypothermia
In modern cardiac surgery, it is unusual to cool patients to nasopharyngeal temperatures below 20°C when using deep hypothermic circulatory arrest (DHCA). In the 1990s, it was common to use nasopharyngeal temperatures of 14°C. Lower temperatures are no longer used, because patients may develop choreoathetoid movement disorders after being cooled to nasopharyngeal temperatures below 14°C. Choreoathetosis in infants was usually mild and transient but was severe and chronic in patients after infancy (Wong et al., 1992).
Modern practice also includes techniques to minimize the amount of DHCA time using regional perfusion of the brain and body. The pioneers of cardiac surgery and neurosurgery did not know what level of cooling was necessary to protect the brain in the absence of circulation. They purposely erred on the cold side to avoid cerebral ischemia. In addition, they had no method, other than cooling, to stop the heart for intracardiac surgery. Pharmacologically induced cardioplegia had not yet been developed.
Discussion
The discovery of a case series (Stephen et al., 1961), presented in our previous paper (Zafren et al., 2020), describing uneventful recovery from induced hypothermia with a core temperature of 4.2°C, raised questions about the limits of survival from hypothermia. The discovery of several additional case series and an unreported case, with at least six additional survivors of cooling to 7°C or below, adds further hope of resuscitating profoundly hypothermic patients with accidental hypothermia below the current record of 11.8°C.
The additional papers add to the physiologic observations of the case series we previously described (Stephen et al., 1961). As in the previous case series, the additional papers demonstrated the extreme variability of human responses to physiologic stimuli, such as cooling and rewarming.
Limitations
Most of the articles we reviewed are about 60 years old. Temperatures were charted by analog methods that are not as accurate as digital methods. In some cases, temperatures were reported to the nearest 0.1°C. In other cases, temperatures were reported only to the nearest 1°C or we had to estimate temperatures from graphic representations of data. We cannot be sure that all the esophageal temperatures were measured with the probe in the lower third of the esophagus. Nasopharyngeal temperatures, reported in two case series, may not correspond well to esophageal temperatures. We also do not know the temperatures of the inhaled gases.
As observed in our previous paper, there is a difference of greater than 7°C between the lowest core temperature with survival in accidental and induced hypothermia. Induced hypothermia is not the same as accidental hypothermia. One difference is that cooling in accidental hypothermia proceeds from the body surface inward (centripetal), while induced hypothermia for surgery is usually produced by core cooling that spreads to the periphery (centrifugal). We do not know how this difference affects the likelihood of survival. It is not known whether survival in accidental hypothermia is possible at temperatures as low as in induced hypothermia.
In accidental hypothermia, cooling is much slower and lasts much longer than with direct cooling of blood for surgery. In induced hypothermia, cooling times are typically less than an hour. We do not know the time course of core temperatures in cases of accidental hypothermia. Longer durations of cooling may have more pronounced physiological effects than shorter courses, with possible depletion of energy stores or prolonged physiologic derangements, such as metabolic acidosis. Rewarming times using extracorporeal circulation (CPB or extracorporeal membrane oxygenation) may be similar in accidental and induced hypothermia.
Because the methods and durations of cooling are different between accidental and induced hypothermia, esophageal temperature measurements may not be equivalent. Various methods were used to induce hypothermia. The distribution of temperatures measured at different locations, such as the esophagus and the brain, may have varied among cooling methods. Esophageal temperatures may have been affected by opening the chest in hypothermia induced for surgical procedures.
Additional potential problems in using data from induced hypothermia as a proxy for accidental hypothermia involve the use of anesthetics and other drugs in induced hypothermia and the fact that hemodynamic parameters are typically controlled during the induction of hypothermia. The effects of anesthesia on the cardiovascular system and on the CNS during profound hypothermia are unknown. Other drugs used during induced cooling include heparin and, in some cases, antidysrhythmic medications. The physiological measurements we reviewed may have been influenced by the use of anesthetics and other drugs or by the cooling and perfusion techniques that were used to induce hypothermia. Only EEGs could be used to evaluate the effects on the CNS.
Yet another limitation is the lack of formal assessment of neurologic outcomes. Without the results of neurocognitive testing, we have assumed that the patients who made satisfactory or uneventful recoveries or who were reported as “well” were neurologically intact.
Conclusions
As in our previous report, there was a wide variation in individual physiological responses to hypothermia. These data add to our understanding of the physiology of profound hypothermia. It is still not known whether survival from accidental hypothermia is possible with a core temperature below 11.8°C, but the additional cases, with survival after cooling to as low as 5°C, suggest that the lower limit for successful resuscitation is much lower. We continue to advise against using core temperature alone to decide whether a hypothermic patient in cardiac arrest has a chance of survival.
Footnotes
Acknowledgments
The authors are grateful to the University of Alaska Anchorage Medical Library, a member of the Network of the National Library of Medicine, for tracking down full text of many older references.
Authors' Contributions
K.Z. wrote the first draft. All authors revised the article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.