
Abstract

D
Ledingham was the first to report the use of HBOT to treat cold injury, but the details of the treatment protocol were not provided (Ledingham, 1963). Since then, many studies have attempted to assess the efficacy of HBOT in the treatment of freezing cold injury, with equivocal results. Rapid tissue freezing in animal models, where HBOT did not show improvement, might be the main reason for this bias, as this does not mimic the pathophysiology of freezing cold injury observed in alpinists. A digit with frostbite always comprises both tissue with freezing- and nonfreezing cold injury and possibly uninjured tissue. HBOT can provide support to nonfreezing cold injury tissue and prevent further damage.
Our research group has been administering HBOT as an adjunct therapy in patients presenting with freezing cold injury for the last 25 years, always with a positive outcome or improvement, however, an early onset of HBOT after injury is crucial (Mekjavic et al., 2005). This has culminated in the clinical paradigm “Planica protocol” for the treatment of freezing cold injury, presented in Figure 1, which includes HBOT as an adjunct therapy. Such a paradigm should be recommended as a guideline for frostbite treatment to societies such as Wilderness Medicine Society and ICAR. We credit Dr. W.J. Mills, Jr., for providing us with the confidence to pursue this effort.
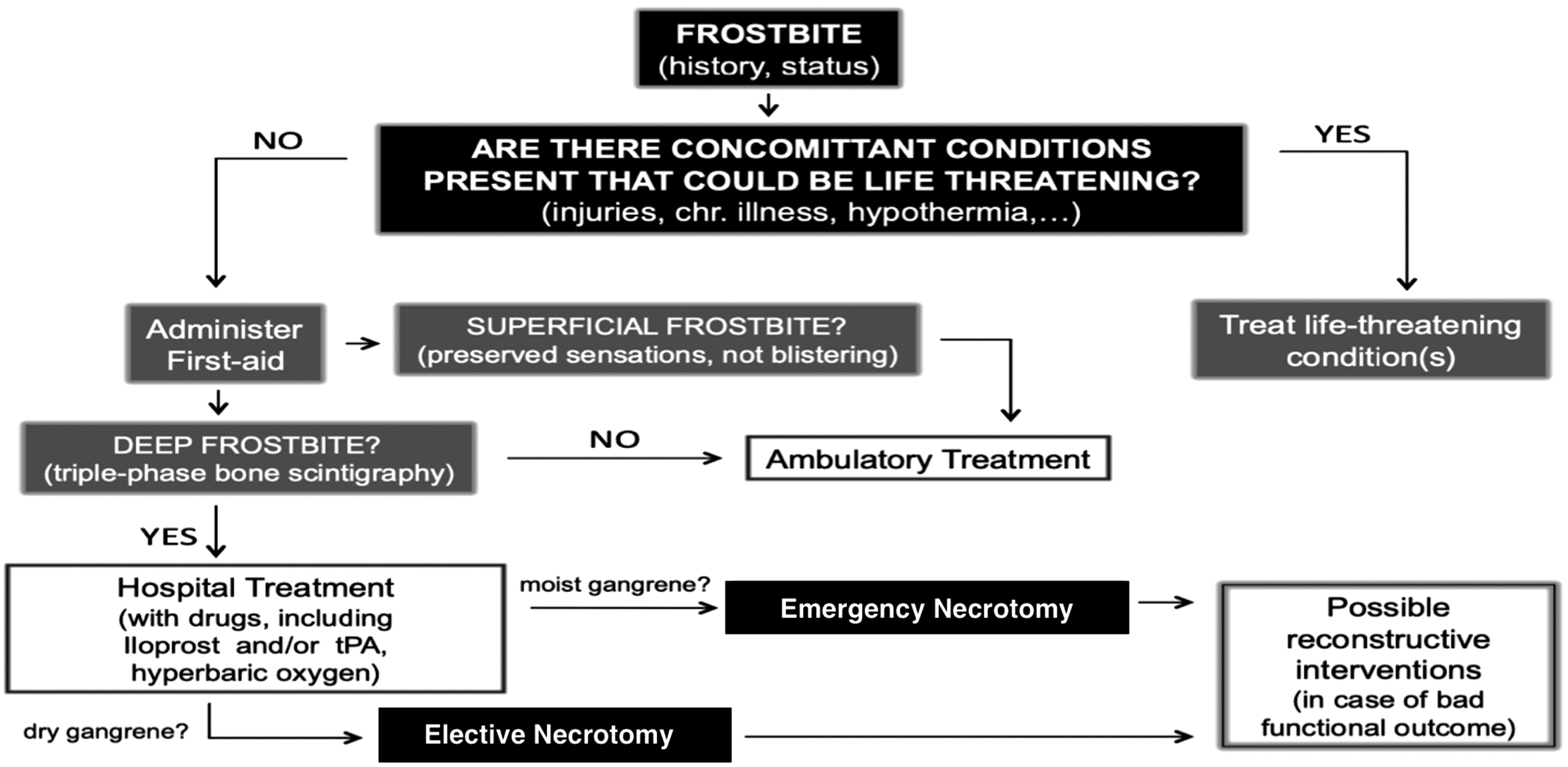
Planica protocol for frostbite management.
The article by Davis, et al. raises the issue of individual susceptibility to freezing cold injury (Davis et al., 2022). The most commonly used test for assessing it is the test of cold-induced vasodilatation (CIVD), whereby a limb or digit is immersed in cold water (8°C), and the subsequent vasodilatory response, if present, is quantified. Subjects with a good vasodilatory response that increases skin temperature significantly (responders) may be less susceptible to freezing cold injury than those with a weaker response (nonresponders). Analysis of mountaineering expeditions where members used the same equipment, followed the same daily routine, and were, therefore, exposed to the same weather conditions showed that some sustained freezing cold injury, whereas others did not (Gorjanc et al., 2019).
The possibility, that the reason for success of late HBOT in the injured Denali alpinist reported by Davis, might have been a lower susceptibility for freezing cold injury (e.g., better CIVD response), cannot be neglected. We suggest that the Denali female climber from the case report might be one of those “good-responders,” who suffered frostbite in very harsh conditions, but improved better than expected because of her probably excellent vasomotor drive, optimized by the introduced treatment. This hypothesis could possibly be tested after her full recovery.