
Abstract
Background:
Controversy remains in the association between smoking and the risk of acute mountain sickness (AMS). Therefore, a systematic review of the existing literature may help clarify this association.
Methods:
We conducted a systematic search of PubMed, Embase, and Cochrane Library from database inception up to October 19, 2021. Both unadjusted and adjusted relative risks (RRs) and 95% confidence intervals (CIs) were calculated to compare the risk of AMS in the smoking and nonsmoking groups. Meta-regression was conducted to explore the factors causing heterogeneity of the studies, and subsequent stratified analysis was performed to present the pooled RR in different subgroups. Publication bias was assessed using funnel plots.
Results:
A total of 28 eligible articles (31 studies) were included. The pooled unadjusted and adjusted RRs were 0.88 (95% CI: 0.78–1.01) and 0.87 (95% CI: 0.77–0.99), respectively, using random-effect models. Publication bias was observed owing to restrictions on the sample size. The ascending altitude and sex composition of the study population were likely sources of heterogeneity according to meta-regression. Studies on participants with an ascending altitude of over 3,500 m or composed of both males and females reported a slight but not significant protective effect of smoking on the risk of AMS, with high heterogeneity.
Conclusions:
Smoking had no significant effect on AMS risk in this meta-analysis. Current studies showed high heterogeneity and included little information on quantitative exposure to smoking (i.e., dose and frequency); thus, the results require careful explanation.
Introduction
Acute mountain sickness (AMS) is a clinical syndrome caused by maladjustment to a hypoxic environment at high altitudes in a short time, usually manifesting as headache, dizziness, fatigue, weakness, dyspnea, and gastrointestinal illness (Wagner et al., 2006; Luks et al., 2017). Besides its high prevalence and common symptoms (Meier et al., 2017), AMS may also progress to life-threatening conditions, such as high-altitude pulmonary edema (HAPE) and high-altitude cerebral edema (HACE), resulting in death (Lamichhane et al., 2022). Given the growing number of people from low-altitude areas travelling, working, and undergoing extreme sports in high-altitude areas, interventions are needed to reduce the risk of AMS.
Many studies have explored the risk factors for AMS, and significant associations have been observed with age (Gianfredi et al., 2020), sex, body mass index (Vignati et al., 2021), medical history (Duke et al., 2020), smoking (Vinnikov et al., 2015), altitude at the destination (Hundt et al., 2022), and transportation (Anderson et al., 2015). Of these factors, the association between smoking and AMS has not reached consensus. One cohort study targeting occupational populations reported that smoking increased the likelihood of AMS (Vinnikov et al., 2015), whereas other studies showed that smokers had a lower incidence of AMS, suggesting that smoking is a protective factor against AMS (Sánchez-Mascuñano et al., 2017; Wu et al., 2012). Moreover, no significant association between smoking and the risk of AMS has been reported in other cross-sectional or prospective studies (Mairer et al., 2010; Macinnis et al., 2013).
Inconsistent associations have also been reported in related systematic reviews. Although no significant association between smoking and the risk of AMS was previously reported (Masuet-Aumatell et al., 2017), the latest systematic review concluded that smoking lowers the risk of AMS (Huang, 2019). In addition, it is necessary to consider the latest primary evidence (Ke et al., 2020; Chen et al., 2021; Yuan et al., 2021). Therefore, this systematic review and meta-analysis aimed to assess the association between smoking and the risk of AMS and explore the underlying heterogeneities for inconsistent results.
Materials and Methods
This systematic review has been registered in PROSPERO (ID:CRD42021286841) and was conducted according to the Preferred reporting items for systematic review and meta-analysis (PRISMA) guidelines (Moher et al., 2009).
Search strategy
We systematically searched PubMed, Embase, and the Cochrane Library from database inception to October 19, 2021. The search strategy (Supplementary Table S1 in the supplementary material) comprised two parts: one part included “altitude illness,” “altitude sickness,” “mountain sickness,” “mountain illness,” “high altitude cerebral edema,” “high altitude pulmonary edema,” and “high altitude pulmonary edema,” and the other part included “risk*,” “factor*,” “influen*,” “impact*,” “reason*,” “predict*,” “cause*,” “characteristic*,” “induc*,” and “indict*.” In addition, the literature in previous related systematic reviews was checked for eligibility.
Study inclusion
Paired reviewers independently reviewed each record during the study and data extraction. Abstracts reporting risk factors for AMS, HACE, or HAPE were retained for full-text review. Studies were included if they met the following inclusion criteria: study population (adults aged ≥ 18 years), exposure (the data provided on the smoking status of the population were sufficient to analyze), outcome (the number of AMS patients and non-AMS individuals that were reported), and the strength of the association between smoking and the risk of AMS, or the exact number of participants for both smoking status and AMS. The exclusion criteria were as follows: studies that did not report the estimated coefficients or number of respective participants for the exposure/outcome of interest, full text was not available, and studies not written in English. Inconsistency in study inclusion or data extraction was resolved by a third reviewer.
Data extraction
Information on the study (i.e., publication year), population characteristics (i.e., nationality, age, sex), study settings (i.e., study design, sample size), smoking exposure (the exact number of participants with smoking exposure or not, dose), AMS outcomes (incidence, diagnostic criteria), covariates (i.e., altitude of the plateau, speed of ascending, purpose of going to the plateau), and the estimated coefficients of the association between smoking and the risk of AMS were extracted. When this information was unavailable in the literature, we contacted the authors for the original data.
Assessment on study quality
Study quality was assessed using the Meta-Analysis of Observational Studies in Epidemiology statement (Stroup et al., 2000). Each study was evaluated using the following seven questions on whether: (1) the purpose or hypothesis was clearly stated; (2) the inclusion and exclusion criteria were clear; (3) the sample size was estimated in advance, and the participants were continuously recruited; (4) the definition of smoking exposure was clear; (5) the diagnostic criteria for AMS were clear; (6) the evaluation of the outcomes was objective, and the main findings of the study were clearly described; and (7) appropriate statistical methods were used for the main outcome and subgroup analyses. Each question was scored 1 point for “yes” and 0 for “no.” Articles with a final score >5 were defined as high quality.
Statistical analysis
The study population was divided into smoking and nonsmoking groups. The effect of smoking on the risk of AMS was calculated using unadjusted and adjusted relative risks(RRs) and their corresponding 95% confidence intervals (CIs). Meta-regression was conducted to explore potential factors causing heterogeneity. The heterogeneity of the studies was assessed using the I2 statistic and χ2 tests. For studies with low (I2 ≤ 50% and p value of χ2 test ≥ 0.05) and high (I2 > 50% and p value of χ2 test < 0.05) heterogeneity, fixed-effect and random-effect models were used to calculate the pooled RR. Stratified RRs and 95% CIs were reported through subgroup analyses of nationality, age, sex, sample size, altitude, speed of ascending, diagnostic criteria, study design, purpose of going to plateau, original type of estimates of coefficients used in the article, and study quality. Publication bias was assessed for both unadjusted and adjusted RRs using funnel plots. Statistical analysis was performed using Stata MP software (College Station, Texas, USA, version 16.0).
Results
Basic information on articles included
A total of 28 eligible articles were finally included (Fig. 1) after a double-blind two-stage review of 5,381 original records using the search strategy. Overall, 31 studies were included in the meta-analysis because four articles involved two sets of data for analysis; thus, they were regarded as different independent studies (Table 1). Regarding the study design of the included articles, 18 were cross-sectional studies (Bian et al., 2015; Gaillard et al., 2004; Gonggalanzi et al., 2016; Honigman et al., 1993; Kayser, 1991; Mahomed et al., 2015; Mairer et al., 2010; Mairer et al., 2009; Mcdevitt et al., 2014; Pesce et al., 2005; Schneider et al., 2002; Tang et al., 2014; Wagner et al., 2006; Wagner et al., 2008; Li et al., 2015; Wu et al., 2012), 2 were case–control studies (D et al., 2014; Ke et al., 2020), and 11 were cohort studies (Chen et al., 2021; Jafarian et al., 2008; Macinnis et al., 2013; Ren et al., 2015; Sánchez-Mascuñano et al., 2017; Shen et al., 2020; Yuan et al., 2021; Qiu et al., 2017; You et al., 2012). The mean age of the study population was 20–40 years in most of the studies (21 articles). Of the 31 studies, 9 (29%) recruited only young male participants, and 26 (84%) reached a relatively high altitude of over 3,500 m. The Lake Louise AMS scoring system was the most widely adopted definition criteria for AMS diagnosis (24 studies). Half of the included studies were of relatively good quality (Supplementary Table S2 of the Supplementary Data S1).

Flowchart of study selection.
Characteristics of the 28 Eligible Articles Meeting the Inclusion Criteria (31 Studies)
Note.
I: This study analyzed the data of the two groups separately. One was the acute exposure group (a), and the other was the pre-acclimatization group (b).
II: This study focused on two populations separately, one in the Eastern Alps (a) and the other in the Western Alps (b).
III: This study analyzed two sets of data separately. One sample was collected in 1996 and 1998 (a), and the other was collected in 2000 (b). ESQ was used to diagnose AMS in this article.
AMS, acute mountain sickness; LLS, Lake Louise Scoring System; ESQ-III, Environmental Statistical Questionnaire III AMS-C score.
The “Occupational” category of Purpose of going to plateau includes workers, soldiers, professional trekkers, and mountaineers; the “Not occupational” category includes amateur travelers, pilgrims, and participants without specific recruiting statements.
Meta-analysis
Of the 31 studies included (smoking group, n = 2,691; nonsmoking group, n = 10,710), smoking showed no significant effect on the risk of AMS (unadjusted RR = 0.88, 95% CI: 0.78–1.01, I2 = 72.2%; adjusted RR = 0.87, 95% CI: 0.77–0.90, I2 = 67.2%) (Fig. 2). Publication bias was found among the 31 studies (p = 0.016); however, after excluding eight studies with a total sample size of less than 100 participants, publication bias was eliminated (p = 0.055) (Fig. 3).
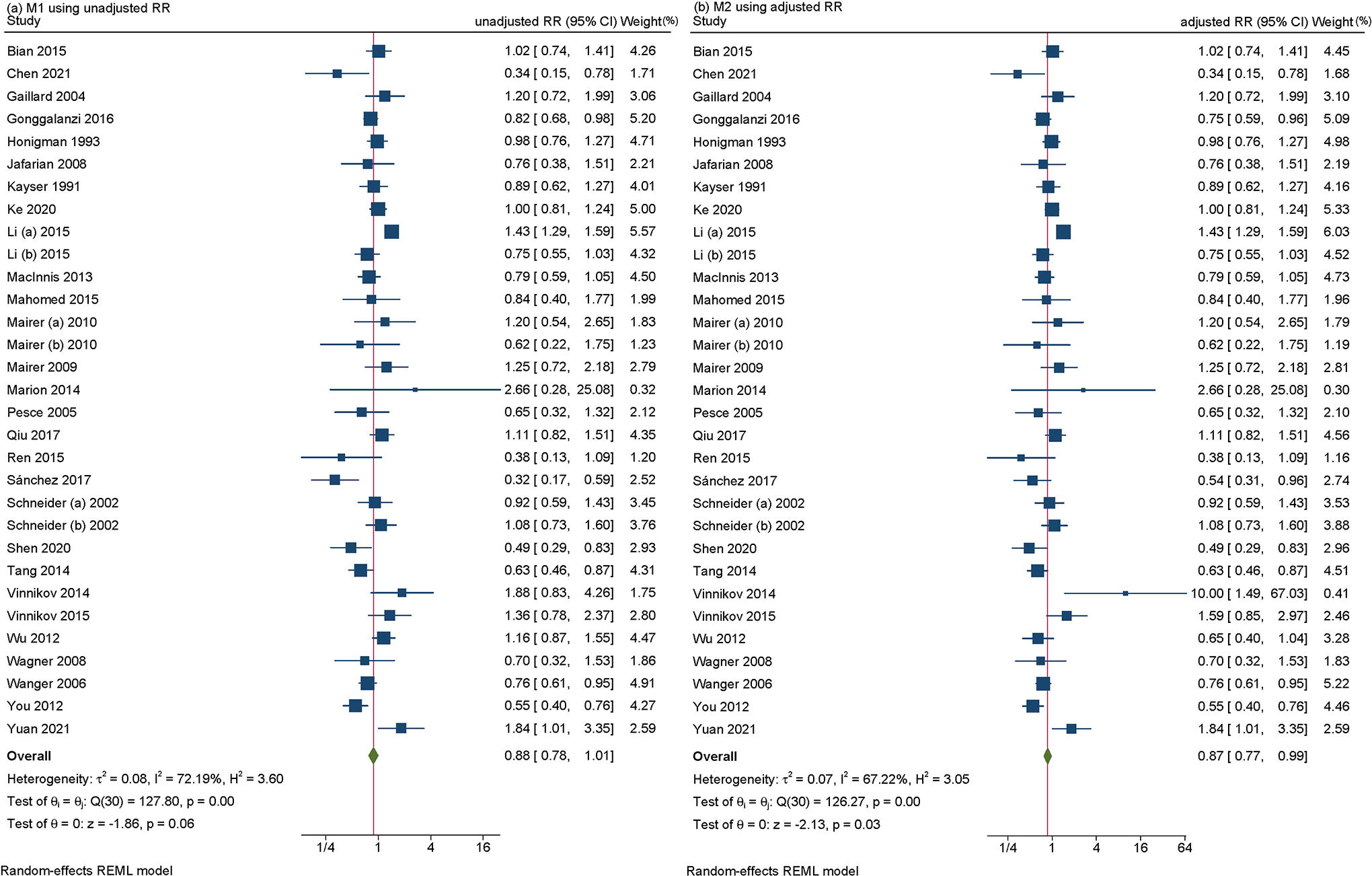
Forest plot of pooled effect value.
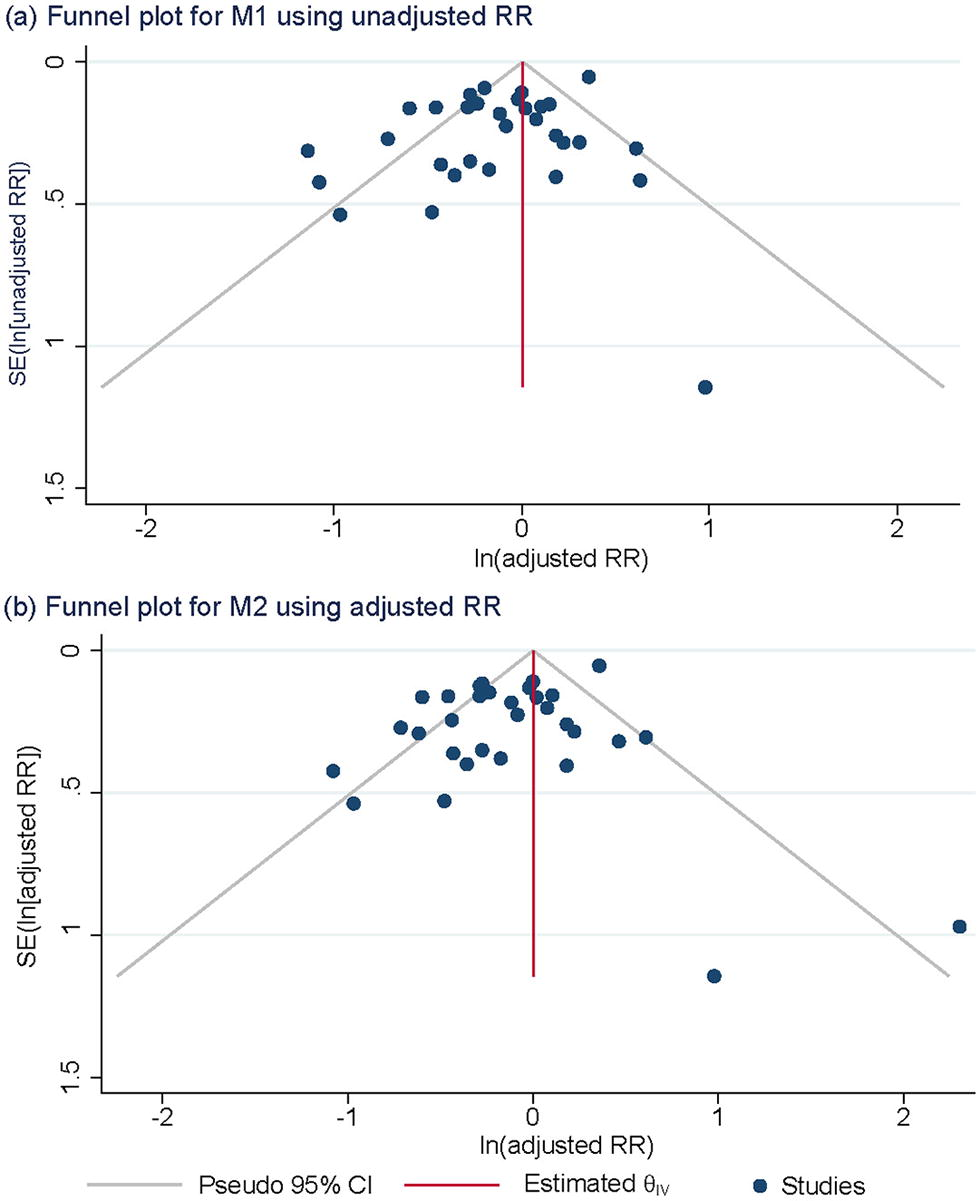
Funnel plot.
Meta-regression and stratified analysis
Meta-regression showed that plateau altitude and sex of the participants were likely to be the cause of heterogeneity (p < 0.1) (Table 2, Supplementary Figures S1-S10). High heterogeneity was found in almost all the stratifications. The effect of smoking on the risk of AMS was inconsistent, as some stratifications showed statistically significant protective effects, whereas others showed no significance (Table 3). The meta-analysis stratified by plateau altitude showed a slight protective effect of smoking on the risk of AMS in the group of altitude ≥ 3,500 m, although with high heterogeneity (I2 = 72% in the unadjusted model and 71% in the adjusted model). In contrast, no significant risk effect was observed in the group of altitude < 3,500 m, with low heterogeneity (I2 = 0% in both unadjusted and adjusted models). The meta-analysis stratified by sex reported a significant protective effect for the group of “composed of both males and females” (unadjusted RR = 0.84 [95% CI = 0.73–0.96], adjusted RR = 0.84 [0.75–0.94]), whereas no significant protective effects were observed in the “only males” group (unadjusted RR = 0.98 [95% CI: 0.77–1.23], adjusted RR = 0.92 [95% CI: 0.72–1.18]).
Results of Meta-Regression
Note.
Mu1: included each variable separately entered into the model using unadjusted coefficients of estimates (i.e., relative ratio, also called univariate RR, uRR, in the original studies that met the inclusion criteria).
Mu2: included Plateau altitude + Sex together entered into the model using unadjusted coefficients of estimates.
Mu3: included Nationality + Plateau altitude + Sex together entered into the model using unadjusted coefficients of estimates.
Mu4: included all variables together entered into the model using unadjusted coefficients of estimates.
For included studies which offered odds ratio (OR) as the estimates of coefficients, rather than RR, we first transformed OR to RR using the following formula: uRR = uOR/([1 − prevalence rate in the control group] × [prevalence rate in the control group × uOR]).
Mad1: included each variable separately entered into the model using adjusted coefficients of estimates (i.e., relative ratio, also called multivariate RR, adRR, in the original studies that met the inclusion criteria, which were to be pooled in the subsequent stratified meta-analysis).
Mad2: included Plateau altitude + Sex together entered into the model using adjusted coefficients of estimates.
Mad3: included Nationality + Plateau altitude + Sex together entered into the model using adjusted coefficients of estimates.
Mad4: included all variables together entered into the model using adjusted coefficients of estimates.
AMS, acute mountain sickness; LLS, Lake Louise Scoring System.
Results of the Stratified Meta-Analysis
Note.
In the meta regression, “Nationality” was found as a statistically significant variable for the cause of heterogeneity. “Study design” and “Study with adjusted estimates” were considered as the potential variables for heterogeneity. Therefore, forest plots for the above three variables were additionally conducted for showing their stratified meta-analysis.
M1 was the model that used not adjusted relative ratio (also, univariate RR [uRR] in the original studies that met the inclusion criteria) as the estimates of coefficients in exponential form, which were to be pooled in the subsequent stratified meta-analysis. For included studies which offered odds ratio (OR) as the estimates of coefficients in exponential form, rather than RR, we first transformed OR to RR using the following formula: uRR = uOR/([1 − prevalence rate in the comparison group] × [prevalence rate in the comparison group × uOR]).
M2 was the model that used adjusted RR (also, multivariate RR in the original studies that met the inclusion criteria) as the estimates of coefficients in exponential form, which were to be pooled in the subsequent stratified meta-analysis. There were only 5 studies that offered adjusted RR in the original literature.
CI, confidence interval; AMS, acute mountain sickness; LLS, Lake Louise Scoring System.
Discussion
This study showed an inconclusive effect of smoking on the risk of AMS due to high heterogeneity, and the stratified RRs showed inconsistent effects in some subgroups. To explore the source of heterogeneity and reduce its impact on the results of the main outcome, we performed meta-regression and stratified analyses. Through meta-regression, ascending altitude and sex composition of the participants were the possible causes of heterogeneity. Stratification analysis showed an inconsistent protective effect of smoking, with both significance and insignificance in each variable, although majority of the results showed a significant protective effect of smoking, with high heterogeneity.
The high heterogeneity might also contribute to the publication bias detected among the 31 studies; however, after excluding eight studies with sample sizes smaller than 100 participants, publication bias was effectively eliminated. This shows that existing studies were conducted using different methodologies, which might be the underlying reason for the inconsistent effect of smoking on AMS. Moreover, we considered all the potential factors causing heterogeneity from the perspective of study design (including sample size, diagnostic criteria, methodological design, and study quality), study setting (including plateau altitude, speed of ascending, purpose of going to plateau, and type of reported estimates of coefficients in the original article), and study population (including nationality, age, and sex composition). However, except for the slight effect of altitude and sex composition on heterogeneity, the high heterogeneity of the included studies still needs in-depth exploration. This might be a challenge for future studies.
The inconsistent effects found in this study mirror those of previous studies. Meta-analyses by Huang et al. and Xu et al. reported that smoking had a protective effect against AMS (Xu et al., 2016; Huang, 2019). However, Vinnikov et al. and Masuet-Aumatell et al. indicated that smoking was not associated with the risk of AMS (Vinnikov et al., 2016; Masuet-Aumatell et al., 2017). The characteristics of the included studies may have influenced the results. The results of the “altitude ≥ 3,500 m” stratification and the “cut-off sample size = 500 participants” were parallel to the protective result in the studies by Huang et al. and Xu et al. As for the systematic review by Masuet-Aumatell et al., most included studies (72.7%) were cross sectional, and their pooled effect showed no significance. This finding was also consistent with the stratification results of our study (insignificant effect and high heterogeneity). In addition, the purpose of going to an altitude was closely related to the terminated altitude and composition of the participants, which might have contributed to heterogeneity. Therefore, the ascending purpose and ascending speed were both considered in the meta-analysis, although smoking was reported as an insignificant protector in both stratifications.
Although there were insignificant stratified RRs in some groups, we attempted to explore potential mechanisms for the significant effect of smoking on the risk of AMS shown in other stratified and pooled RRs. This might shed light on the underlying mechanisms of smoking and risk of AMS. First, a high concentration of nitric oxide, which is one of the main substances generated from smoking, leads to a compensatory increase in hemoglobin in cigarette smokers, allowing smokers to more rapidly adapt to the plateau (Sharma et al., 2019). Second, the lower the blood velocity, the lower the risk of cerebral edema (Kalfaoglu et al., 2017), and overstimulated intracranial nerves (Burtscher et al., 2021) were found in smokers. These metabolic pathways should be explored in future studies.
The incidence of AMS was high in studies meeting the inclusion criteria, indicating that AMS is a prevalent disease among people who go to the plateaus for activities such as travel and work. In addition, the proportion of smokers was high. Fifteen studies had a proportion of >20%. In the stratified analysis, the majority of stratifications of all potential factors (nationality, age, sex, sample size, plateau altitude, speed of ascent, diagnostic criteria, study design, purpose of going to plateau, type of reported estimates of coefficients, and study quality) reported the potential protective effect of smoking on the risk of AMS, although most had high heterogeneity. However, a relatively large discrepancy may be seen in the stratifications of study design, in which both cross-sectional and cohort studies showed protective effects, whereas case–control studies reported smoking as a risk factor. This inconsistency may be caused by sample size restriction, which is also an important factor contributing to publication bias in all included studies. The sample size of all included case–control studies was 634, whereas the other two designs had over 3,000 and 10,000 participants. However, smoking cannot be recommended as a practical health intervention for AMS, not only due to the insignificant protective finding but also the fact that smoking is harmful to health, including impairments in lung function, which may affect altitude acclimatization during prolonged stays at high altitude (Wu et al., 2012).
Our results have practical significance. Although the effect of smoking on the risk of AMS was insignificant, the enhancement of AMS prevention among nonsmokers and the general population should be highlighted, which might have been overlooked in the past as health campaigns always focus on smokers. Therefore, more attention is needed on risk prevention among nonsmokers when they ascend to altitudes (recommending slow ascent), which include acclimatization by ascending to moderate or higher altitudes during either continuous or intermittent altitude preexposure (Lopez et al., 2013), low-speed transportation (travel by air is not recommended) (Gonggalanzi et al., 2016; Vinnikov et al., 2014), and taking acetazolamide (Marmura and Hernandez, 2015; Lopez et al., 2013). Of note, it is more economically beneficial for health education on AMS, as nonsmokers account for the majority of the general population compared with smokers.
Our study has four main advantages. First, the effect value was assessed based on 28 studies, including 2,691 smokers and 10,710 nonsmokers, which is more comprehensive than any previous review of the same topic. Second, the study designs of the included studies were diverse; one-third were cohort studies (11 articles). Third, we discussed the source of heterogeneity by combining meta-regression and stratified analyses. Finally, we summarized the characteristics of the studies included in previous meta-analyses and discussed the possible mechanisms to shed light on further studies. However, this meta-analysis has some limitations. First, more than half of the included articles did not focus directly on the association between smoking and AMS. Smoking was not the primary exposure of interest in most studies. The definition of smoking exposure was unclear or lacking. Moreover, detailed data on the severity of smoking exposure (i.e., dose and frequency of smoking) could not be collected from all the included studies, except for Wu et al. (2012). Meanwhile, exposure information from all included studies was self-reported, which is inevitably influenced by subjective factors that may induce reporting bias. Although inherent difficulties exist in measuring exhaled carbon monoxide/cotinine in urine in population-based epidemiological studies, precise biological tests (such as exhaled carbon monoxide or cotinine in urine) can be performed in future studies to avoid reporting bias. This is also reflected in the existence of publication bias when all 31 studies were included, regardless of the sample size. More importantly, smoking is harmful to health. Therefore, smoking cannot be recommended as a practical prevention method for AMS.
Conclusion
The association between smoking and the risk of AMS remains inconclusive because of the inconsistency observed in different stratifications, high-heterogeneity of the studies included in the meta-analysis, and limited measurements of smoking exposure in the original articles. Further studies on smoking with more detailed measurements, as well as the underlying mechanisms between smoking and the risk of AMS, should be explored.
Footnotes
Authors’ Contributions
Q.G. conceived and designed the study. Y.Y., P.G., L.X., and K.W. performed the literature search, extracted the data, and assessed the study quality. Y.Y., P.G., and D.D. performed statistical analyses and wrote the article. Y.Y. revised the article. Y.Y. re-extracted and confirmed the data, assessed the study quality, performed statistical analysis, and responded to the reviewers in the revision process.
Author Disclosure Statement
The authors had no competing interest.
Funding Information
This work was supported by the
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.