
Abstract
Lin, Tian, Huaping Jia, Yunming Li, Yongxing Xu, Bei Zhao, Dong Zheng, Hongfeng Yan, Meihui Zhao, Yanlei Li, Liping Xia, Fengxia Zhou, Cuiping Liu, Ke Ma, Ma Mi, and Jianwen Gu. Epidemiological survey of congenital heart disease among children aged from 2 to 18 in Suo County, Nagqu, Tibet. High Alt Med Biol. 00:000–000, 2024.
Background:
Studies have reported the prevalence of congenital heart disease (CHD) in parts of Tibet, but relative epidemiological surveys are rare. We aimed to explore the prevalence of CHD in children and its relationship with family history in Suo County, Nagqu, Tibet, an altitude of 3,980 meters.
Methods:
We recruited 4,002 children aged 2–18 years. Subjects underwent a family history investigation, cardiac auscultation, and clinical manifestation examination and then received echocardiographic screening.
Results:
The prevalence of CHD among children in Suo County was 0.97% (39 cases), much higher than the prevalence at sea level. The most common subtype was atrial septal defect, accounting for 53.9% of CHD, followed by patent ductus arteriosus (33.3%) and ventricular septal defect (12.8%). We also found that children whose mothers had previously borne children with CHD had a higher risk of CHD than those without (p = 0.002); other factors related to CHD during pregnancy, such as smoking, drinking, drug use, and viral infection, showed no statistical differences between children with and without CHD.
Conclusions:
The prevalence of CHD in children in Suo County is much higher than at low altitude, consisting mostly of simple forms with left-to-right shunt, with rare complex CHD. These results support implementing diagnostic and treatment plans to prevent CHD in Suo County.
Introduction
Congenital heart disease (CHD) is the abnormity of heart structure, vascular morphology, and function caused by various reasons during embryonic development. It accounts for one-third of the common birth defects in China, seriously endangering children’s health and causing economic and mental burden to society and families (Matthews et al., 2015; van der Linde et al., 2011). The incidence of CHD is strongly related to the area in which patients are born and live, being much higher in high-altitude areas than in low-altitude areas and increasing with altitude (Hoffman, 2013; Hu et al., 2014). This has been attributed to low oxygen, cold temperature, ionizing radiation, and strong ultraviolet radiation environment at high altitude (Ma et al., 2018; Whayne, 2014; Zheng et al., 2017). Suo County is located at the junction of the northern Tibetan high-altitude area and the eastern Tibetan canyon, with an average altitude of 3,980 meters. To date, there have been only a few reports on the prevalence of CHD in children in Suo County and no relevant systematic epidemiological investigations (Chun et al., 2019). Therefore, using echocardiography as the main screening method, we designed an epidemiological questionnaire and performed CHD screening among children in Suo County in order to investigate the prevalence of CHD and provide information for the prevention and treatment of CHD in this area.
Methods
Study population
We carried out this investigation among all the children in kindergarten and primary school in Suo County, including two kindergartens and two primary schools.
Demographic data and physical examination
From September to November 2020, professional medical staff from Strategic Support Force Medical Center conducted the epidemiological investigation and physical examination on the enrolled children, including collection of data on medical history, family history, living environment, pregnancy and perinatal conditions, general physical examination during pregnancy, and cardiac auscultation. All parents were informed of the study information and signed informed consent prior to participation.
Echocardiography
Transthoracic echocardiography was performed on all children in left recumbent position by the same sonographer, using a color doppler ultrasound system (CHISON Q8, Wuxi, China) equipped with a 2.5 MHz transthoracic transducer (CHISON D3P64L).
The section views of echocardiography included parasternal long-axis view, artery short-axis view, series of left ventricular short-axis view, parasternal four-chamber and five-chamber view, apical four-chamber and five-chamber view, apical left ventricular long-axis and two-chamber view, inferior xiphoid series view, and superior sternal fossa view.
Two-dimensional imaging with color doppler flow mapping depicted the location and size of the defect. Diagnostic criteria were based on Clinical Echocardiography (third edition), and the result was qualitative diagnosis, including normal and abnormal (Liu and Xiong, 2014). Abnormalities were given with definite diagnosis, such as atrial septal defect (ASD), patent ductus arteriosus (PDA), ventricular septal defect (VSD), and patent foramen ovale (PFO).
Statistical analysis
All data were analyzed using SPSS software for windows (version 25.0, IBM Corp, Armonk, NY, USA). The measurement data conforming to normal distribution were represented by
Results
Total prevalence of CHD and PFO
In total, 4,002 children were enrolled, including 2,025 boys (50.6%) with an average age of 8.73 ± 2.38 years (with a range of 3–17 years) and 1,977 girls (49.4%) with an average age of 8.74 ± 2.40 years (range 2–18 years). Heart murmurs were heard in nine children, and two children were diagnosed with primary pulmonary hypertension. Cardiac anomalies were detected in 108 children, among whom 39 cases of CHD were confirmed, for a prevalence of 0.97%. There were 20 boys with a prevalence of 0.99% and 19 girls with a prevalence of 0.96%. The difference was not statistically significant between boys and girls (p > 0.05). PFO was detected in 69 children, for an overall prevalence of 1.72%, including 31 boys (1.53%) and 38 girls (1.92%), with no significant difference between boys and girls (p > 0.05).
Prevalence of CHD subtypes and PFO by age and sex
Among the 39 cases of CHD in Suo County, 21 cases (53.9%) were ASD, followed by 13 cases (33.3%) of PDA and five cases (12.8%) of VSD. There was no significant difference in the prevalence of each subtype of CHD between boys and girls (p > 0.05) (Table 1 and Fig. 1).
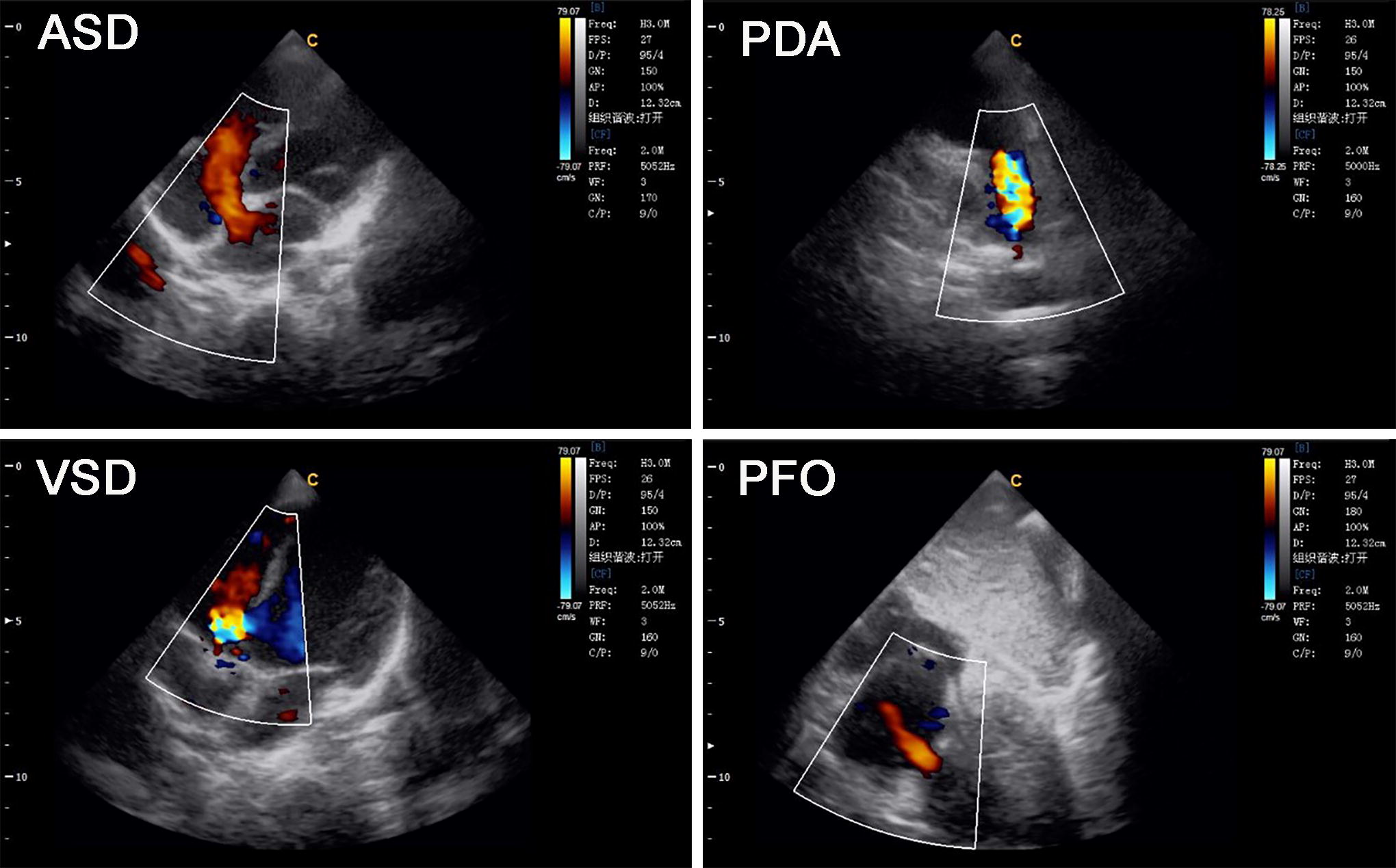
Echocardiographic images of different types of children with abnormal hearts. ASD, atrial septal defect; PDA, patent ductus arteriosus; PFO, patent foramen ovale; VSD, ventricular septal defect.
Subtypes of Abnormal Cases According to Children’s Sex and Age
Values are presented as n (%).
ASD, atrial septal defect; CHD, congenital heart disease; PDA, patent ductus arteriosus; PFO, patent foramen ovale; VSD, ventricular septal defect.
The prevalence rates and subtypes of CHD were different in various age-groups. The 4,002 enrolled children were divided by age into the childhood group (<7 years) and the juvenile group (≥7 years); the corresponding numbers were 447 (11.2%) and 3,555 (88.8%), respectively. We found no statistical difference in the prevalence of CHD between the age-groups (0.89% vs. 0.98%). Children with CHD in childhood group were all diagnosed as PDA (0.89%), and no other subtypes were observed. However, the most common subtype in the juvenile group was ASD (0.59%), followed by PDA (0.25%) and VSD (0.14%). The prevalence of PDA in children under 7 years was significantly higher than that in children over 7 years (0.89% vs. 0.25%; p = 0.048). The prevalence of PFO was also significantly different in the two age-groups, at 3.36% in children under 7 years versus 1.52% in children over 7 years (p = 0.010) (Table 1 and Fig. 1).
Analysis of related factors during pregnancy and perinatal period in CHD and PFO cases
The occurrence of CHD and PFO is related to a variety of factors, including family genetic history, environmental factors, intrauterine infection in pregnant women, and drug use in the first 3 months of pregnancy (Sun et al., 2015). Owing to the lack of some data in some individual samples, 3,994 valid samples were included in this part, divided into the control group (3,886 cases) and the abnormal group (108 cases) according to the results of the cardiac ultrasound examination. We found that there were four cases in the abnormal group whose mothers had been pregnant with CHD children (3.7%), whereas there were 17 cases (0.4%) in the control group; this difference was statistically significant (p = 0.002). However, there were no statistical differences between the two groups in other risk factors related to pregnancy and the perinatal period (p > 0.05) (Table 2).
Analysis of Related Factors During Pregnancy and Perinatal Period in CHD and PFO Cases
Values are presented as n (%).
Fisher’s exact test.
t-test.
Mann–Whitney U test.
BMI, body mass index; CHD, congenital heart disease; CT, computed tomography; PFO, patent foramen ovale.
Discussion
Studies have reported significant geographical differences in the incidences and subtypes of CHD (Hoffman and Kaplan, 2002). A recent article reported that the average birth prevalence of total CHD in China during 1980–2019 was 0.25 per 100 births and found significant differences in CHD prevalence among children in different regions of China (Zhao et al., 2020). In another study, cardiac ultrasonography was performed on potential CHD children in 11 cities in eastern China. The total birth prevalence of CHD was 0.58 per 100 births (Pan et al., 2022). However, most of the data above are from low-altitude areas. The high-altitude region has a unique environment, and therefore, the prevalence rates and subtypes of CHD may differ from low-altitude regions. Currently, reports on CHD prevalence at high altitude are rare. A recent cross-sectional study was conducted among school-aged children in Qinghai province, which found that the overall prevalence of CHD in Qinghai province was 0.67%, and higher altitudes (odds ratio, 2.28) were shown to be independently associated with CHD prevalence (He et al., 2022). Another study, of 7,088 children aged 4–17 years in Tibet, reported CHD prevalence rates of 0.46%, 1.08%, and 1.34% at altitudes of 2,800–4,200 meters, 4,200–4,700 meters, and above 4,700 meters, respectively, suggesting that the prevalence of CHD rises with increasing altitude (Zheng et al., 2017). Except for high altitudes in China, another article analyzed the relationship between high altitude, identified in several cities in Ecuador, and the prevalence of CHD. A correlation coefficient of 0.914 showed the direct relationship between high altitude and prevalence rates of CHD. For each year elapsed, the prevalence of CHD increased by 3.33 cases per 10,000 live newborns (Gonzalez-Andrade, 2020).
The present study was a cross-sectional survey of CHD prevalence among children aged 2–18 years in Suo County, Nagqu, Tibet, an altitude of 3,980 meters. We found that the prevalence of CHD was 0.97%, much higher than that in low-altitude areas, which may be attributed to some factors unique to high altitude, including low oxygen, cold ambient temperature, ionizing radiation, and strong ultraviolet rays. At high altitude, the combined effects of low oxygen partial pressure, high pulmonary vascular resistance, high central systolic pressure, and increased arteriosclerosis lead to delayed or even failed defect closure (Häcker et al., 2018; Triedman and Newburger, 2016). One study published in 2019 reported that the prevalence of CHD in Suo County was 0.16%, much lower than that in our study (Chun et al., 2019). In that study, children first underwent physical examination and heart sound auscultation, and echocardiography was performed only on children suspected of CHD (e.g., heart murmur and cyanosis) to confirm the diagnosis; this may have underestimated the prevalence of CHD (Seldon et al., 1962). Echocardiography was performed on all the participants in our study, and the missed diagnosis rate was low, therefore more accurately reflecting the prevalence of the CHD in local children.
The composition of the CHD spectrum is disparate at different altitudes. VSD is the most common subtype of CHD in low-altitude areas, accounting for about 40% of all subtypes, and critical CHD accounts for 15%–25% of all patients (Hoffman and Kaplan, 2002; van der Linde et al., 2011). However, studies show that ASD is the most common heart defect in Tibetan children living below 4,200 meters, whereas above 4,200 meters, the majority of CHD is PDA (Zheng et al., 2017; Zheng et al., 2013). In this study, we found that ASD (53.9%) was the most prevalent subtype of CHD in Suo County, followed by PDA (33.3%) and VSD (12.8%), consistent with previous reports. Decreased arterial oxygen content at high altitude and the lack of strong stimulation for the constriction and closure of the ductus arteriosus in newborn infants, coupled with the persistence of arterial hypertension and low systemic circulation pressure after birth, are the reasons for the difficult closure of the ductus arteriosus (Dice and Bhatia, 2007; Miao et al., 1988; Penaloza et al., 2008). VSD, the most common heart defect at low altitude, accounted for a smaller proportion in our study. The reason may be that children with VSD at high altitude are more likely to develop pulmonary hypertension than those in low-altitude areas, and persistent pulmonary hypertension puts children at higher risk of right heart failure and early death (Chen et al., 2011).
Increasing evidence shows that PFO is not always benign and is often associated with ischemic stroke, migraine, decompression sickness, peripheral embolism, and obstructive sleep apnea (Kutty et al., 2012). In residents at high altitude, PFO may have special significance owing to the higher pulmonary artery pressure and right heart pressure; it is also closely associated with high-altitude pulmonary edema (West et al., 2019). There have been few epidemiological investigations on the prevalence of PFO in children in high-altitude areas. Our study was the first epidemiological survey on the prevalence of PFO in children in Suo County, finding a prevalence of 1.72%. Because transthoracic echocardiography has certain rate of misdiagnosis of PFO (Mojadidi et al., 2014b), more sensitive detection methods, potentially including transesophageal echocardiography and the agitated saline bubble test, should be adopted for children with symptoms and complications (Mojadidi et al., 2014a; Taramasso et al., 2016).
The prevalence of CHD differs by sex and age. Studies have shown that the prevalence of CHD in women is significantly higher than that in men, and the difference becomes more obvious with increased altitude (Chun et al., 2019; Zheng et al., 2013). However, our study did not find significant sex differences; this discrepancy with previous results may be related to the differences in the survey area and population. In addition, the prevalence and subtypes of CHD in the two age-groups were different in this survey, with the prevalence of PFO and PDA in the childhood group being significantly higher than that in the juvenile group. The differences in the two age-groups may reflect the gradual closure of foramen ovale and ductus arteriosus with age; effective follow-up will be needed in the coming years.
The etiology of CHD is not completely understood but is currently believed to be the result of interactions of environmental and genetic factors (Sun et al., 2015; Triedman and Newburger, 2016). An epidemiological study found that specific congenital heart defects showed highly variable but strong familial clustering in first-degree relatives, ranging from 3-fold to 80-fold compared with the population prevalence (Oyen et al., 2010; Oyen et al., 2009). In this study, we found that the proportion of children whose mothers had given birth to a child with CHD was significantly higher in the children with abnormal hearts than that without, indicating that genetic factors play an important role in the occurrence of CHD in the high-altitude environment. Maternal smoking, alcohol consumption, drug use, pregnancy complication, radiation exposure during pregnancy (Forest and Priest, 2016; Oyen et al., 2016; Zegkos et al., 2020), and viral infection in the first trimester of pregnancy (Ye et al., 2019) are all risk factors for CHD in infants that have been widely recognized in relevant studies in low-altitude areas. Folic acid is thought to be a protective factor for CHD in children (Mao et al., 2017). The above factors were also analyzed in this study, but no statistical differences were found between the children with and without abnormal hearts. The reason may be that the number of people with these exposures in the study population was very small (less than 5%). In addition, ASD and PDA are the most common subtypes of CHD in Suo County, and their formation is largely associated with delayed cardiac pathway constriction and closure after birth, suggesting that postnatal causes such as altitude hypoxia, rather than risk factors during pregnancy, may be the key factors for CHD formation in Suo County. These speculations could be confirmed by further examination in the future, such as via prenatal ultrasound.
Untreated CHD is a major cause of pulmonary hypertension and heart failure in children at high altitude. A retrospective study in Qinghai province showed that 58% of 1,178 patients with CHD aged 1–69 years with simple left-to-right shunt developed moderate to severe pulmonary hypertension and that incidence and severity increased progressively with altitude and age (Chen et al., 2011). Therefore, screening for CHD in children at high altitude is necessary for early detection and treatment of CHD. This study was the first large-scale epidemiological survey of CHD in children in Suo County. Almost all the participants were native Tibetan, therefore reflecting the prevalence, disease spectrum, and risk factors of CHD in local indigenous people.
There were some limitations in this study. Because the study did not include newborns, information regarding CHD among newborns in the region was not available. Furthermore, many unexplained infant deaths were not clearly diagnosed. Hence, it was difficult to obtain the true incidence of CHD at birth in the region from the available data. Moreover, because of the low level of education among the local population, information bias may exist in this survey.
The prevalence of CHD in Suo County was slightly higher than that in low-altitude areas, but all the affected children had single abnormalities without complex malformations, which was contrary to our expectations. Although the local population has a low level of education and living standards, and health guidance for pregnancy is far from universal, this did not lead to a significant increase in the prevalence of CHD and severe heart malformations. This may be partially attributable to the better genetic tolerance of the local population to the special environment of the high altitude. A large number of reports suggest that the indigenous peoples of the Qinghai-Tibet region, especially the Tibetan people, are genetically adapted to hypoxic environments (Wu et al., 2005a). Compared with immigrants to the area, the indigenous peoples have lower hemoglobin, lower pulmonary artery pressure, and higher oxygen uptake and utilization (Wu et al., 2005a; Wu et al., 2005b). In addition, local dietary habits may account for part of the reason. Cordyceps is an edible fungus that grows in the Himalayan region and is widely recognized in traditional medicine. Studies have shown that cordyceps can enhance hypoxia tolerance and improve hypoxia-related pulmonary hypertension (Gao et al., 2010; Singh et al., 2013). Suo County is rich in cordyceps, and whether it plays a role in the pathogenesis of CHD in the local area should be explored in future studies.
Footnotes
Acknowledgments
The authors wish to thank all the staff members at the health committee, People’s Hospital, complete primary school, second complete primary school, bilingual kindergarten, and Yala town bilingual kindergarten of Suo County for their strong support of this study. We thank John Daniel from Liwen Bianji (Edanz) (![]() ) for editing the English text of a draft of this article.
) for editing the English text of a draft of this article.
Authors’ Contributions
T.L. and H.J. contributed equally to this work. J.G. designed and conducted the study. H.J. performed echocardiography. T.L., D.Z., H.Y., and M.Z. were responsible for physical examination. Y.L., L.X., F.Z., and C.L. were responsible for epidemiological investigation and data collection. Y.L. designed and conducted statistical analysis. Y.X. and B.Z. were responsible for revising the article. K.M. and M.M. assisted in designing and conducting the study. T.L. wrote the first draft of the article to which all authors subsequently contributed. All authors read and revised the article for important intellectual content and approved the final article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.