
Abstract
Background:
Pulmonary hypertension (PH) is a prevalent adverse cardiovascular event at high-altitude environments. Prolonged exposure to high altitudes may result in myocardial injury, which is associated with poor clinical outcomes. This study aims to investigate the clinical characteristics of myocardial injury in patients with PH at high altitude.
Methods:
Consecutive patients admitted to a general tertiary hospital at the altitude of 3,650 m were selected into this retrospective study. Clinical and biochemical data were collected, as well as based on cardiac troponin I (cTnI) and echocardiography, patients were divided into myocardial injury group and non-myocardial injury group.
Results:
A total of 231 patients were enrolled, among whom 29 (12.6%) had myocardial injury. We found that body mass index, left ventricular end-diastolic dimension, and serum level of creatine kinase-MB (CK-MB) in myocardial injury group were significantly higher than non-myocardial injury group. Spearman correlation analysis revealed that cTnI has a significant positive correlation with CK-MB and lactic dehydrogenase instead of aspartate aminotransferase. A receiver operating characteristic curve was drawn to demonstrate that CK-MB could significantly predict the occurrence of myocardial injury with an area under the curve of 0.749, and a level of 3.035 (sensitivity = 59.3%, specificity = 90.5%) was optimal cutoff value.
Conclusion:
The incidence of myocardial injury in highlanders with PH is significant. CK-MB, as a convenient and efficient marker, has been found to be closely associated with cTnI and plays a predictive role in the occurrence of myocardial injury with PH in individuals exposed to high altitude.
Introduction
The number of people visiting and residing in high altitudes has witnessed a surge in recent years. It is estimated that 81.6 million people reside above an altitude of 2,500 while 14.4 million individuals live at or above 3,500 m (Tremblay and Ainslie, 2021). High-altitude environments are characterized by hypobaric conditions and hypoxia. Hypoxia poses a significant risk to the heart, as prolonged exposure to chronic hypoxia associated with high altitudes can lead to myocardial injury, which manifests as varying degrees of elevation in serum myocardial enzymes. Pulmonary hypertension (PH) often develops because of increased resistance in pulmonary circulation caused by the high-altitude environment and represents one of the most prevalent cardiovascular complications (Hou et al., 2022). Hypoxia-induced PH is a major health problem at high-altitude regions of the world. Previous study on Kyrgyz highlanders has reported PH prevalence rates ranging from 14% to 20% with their population (Aldashev et al., 2002). Furian et al. (Furian et al., 2021) suggested that highlanders with PH living at high altitude may face an elevated risk of cardiovascular mortality and morbidity. Consequently, greater attention should be devoted to understanding myocardial injury alongside PH among individuals residing at higher elevations.
Myocardial injury is a severe complication in population exposed to high altitude, which can lead to malignant arrhythmias, heart failure, and even sudden death (Lüscher, 2018). Our previous study found that the incidence of myocardial injury was as high as 33.2% in population transferring from high altitude (He et al., 2021). Hypoxic and hypobaric environments can cause damage to cardiac cells, resulting in varying degrees of elevation of serum myocardial enzymes (Neves et al., 2016). Cardiac troponins I (cTnI) and T (cTnT), expressed almost exclusively in the heart, are preferred biomarkers of myocardial injury with high specificity and sensitivity (Mair et al., 2018) and have been regarded as the gold-standard marker for myocardial injury prevention and diagnosis (Park et al., 2017). However, detecting cTnI is challenging because of instrument limitations at high altitudes. Thus, investigating other classical markers such as creatine kinase (CK), lactic dehydrogenase (LDH), and aspartate aminotransferase (AST) is crucial for preventing and diagnosing myocardial injury at high altitude (Parsanathan and Jain, 2020). Several studies have used these myocardial enzymes as indicators for evaluating myocardial injury at high altitude. He et al. (He et al., 2013) found that CK, CK-MB, and LDH levels altered in high-altitude de-acclimatization syndrome after exposure to high altitudes. Zhou et al. (Zhou et al., 2012) suggested that the cardiac function index was negatively correlated with the levels of creatine kinase-MB (CK-MB) and LDH.
In this study, population exposed to high altitude with PH was included and was analyzed to understand the differences between myocardial injury and nonmyocardial injury. Our aim was to investigate the diagnostic value of various myocardial markers for detecting myocardial injury in patients with PH at high altitude, thereby providing a theoretical basis for early clinical prevention and treatment.
Materials and Methods
Study settings
Consecutive patients admitted to the department of cardiovascular medicine in a general tertiary hospital at an altitude of 3,650 m were included. Inclusion criteria: (1) Based on ESC/ERS Guidelines for the diagnosis and treatment of PH (Humbert et al., 2022), all included patients were diagnosed with PH by using echocardiography with the criteria of tricuspid valve regurgitation (TVR) peak velocity >280 cm/s; (2) adult patients aged >18 years old; (3) living continuously at high altitude (>3,000 m) more than one year. Exclusion criteria: (1) all kinds of cardiomyopathy, including ischemic, dilated, hypertrophic, and so on; (2) pulmonary embolism; (3) myocarditis; and (4) congenital heart disease. According to the fourth universal definition of myocardial infarction (Thygesen et al., 2018), patients were diagnosed with myocardial injury once the serum level of cTnI was greater than 0.1 ng/ml, who were classified into myocardial injury group while the others were classified into non-myocardial injury group.
Data collection
Basic information of patients was collected through electronic medical record, including age, gender, body mass index (BMI), living altitude, aborigines, and smoke. Echocardiography and electrocardiogram were performed after admission, and then we could get the indexes including TVR velocity, left ventricular end-diastolic dimension (LVEDD), and heart rate. Early morning fasting blood was drawn from all patients after admission for examination to acquire the data about red blood cell count, hemoglobin (Hb), platelet count, red blood cell distribution width, platelet distribution width, alanine transaminase, AST, total bilirubin, direct bilirubin, albumin, globulin, urea nitrogen, creatinine, uric acid, total cholesterol, triglyceride, high-density lipoprotein cholesterin, low-density lipoprotein cholesterin, apolipoprotein A1, apolipoprotein B, LDH, CK-MB, prothrombin time (PT), activated partial thromboplastin time and D-dimer (D-D).
Statistical analysis
The software SPSS version 25.0 was used to perform statistical analysis, and difference was considered to be significant once p value was lower than 0.05. Normal distribution was examined according to Kolmogorov–Smirnov test. Normally distributed measurement data were expressed as mean value ± standard deviation, and comparisons between groups were analyzed by using t test. Abnormally distributed measurement data were expressed as median value (Q1-Q3), and comparisons between groups were analyzed by using Mann–Whitney U test. Comparisons of enumeration data between groups were analyzed by using chi-square test. Spearman analysis was used to evaluate the correlation between two indexes. Diagnostic accuracy was evaluated by receiver operating characteristic (ROC) curve as assessed by area under the ROC curve (AUC). The optimal cutoff values were determined by using the Youden index.
Results
Clinical features of myocardial injury with PH patients at high altitude
A total of 231 patients at high altitude with PH were included in the present study, of which 29 patients were diagnosed with myocardial injury, accounting for 12.6%. The flow chart for inclusion of patients is shown in Figure 1. As shown in Table 1, patients in myocardial injury group had higher BMI than those in nonmyocardial injury group [(26.1 ± 4.0) kg/m2 vs. (24.4 ± 4.2) kg/m2, p = 0.045]. LVEDD was significantly increased in myocardial injury group compared with non-myocardial injury group [44 (41.5–52.5) mm vs. 42 (40–45) mm, p = 0.005]. Once myocardial injury occurred, the serum level of CK-MB could also significantly upregulate [3.47 (2.1–7.6) U/L vs. 1.37 (1.1–2.4) U/L, p = 0.001].
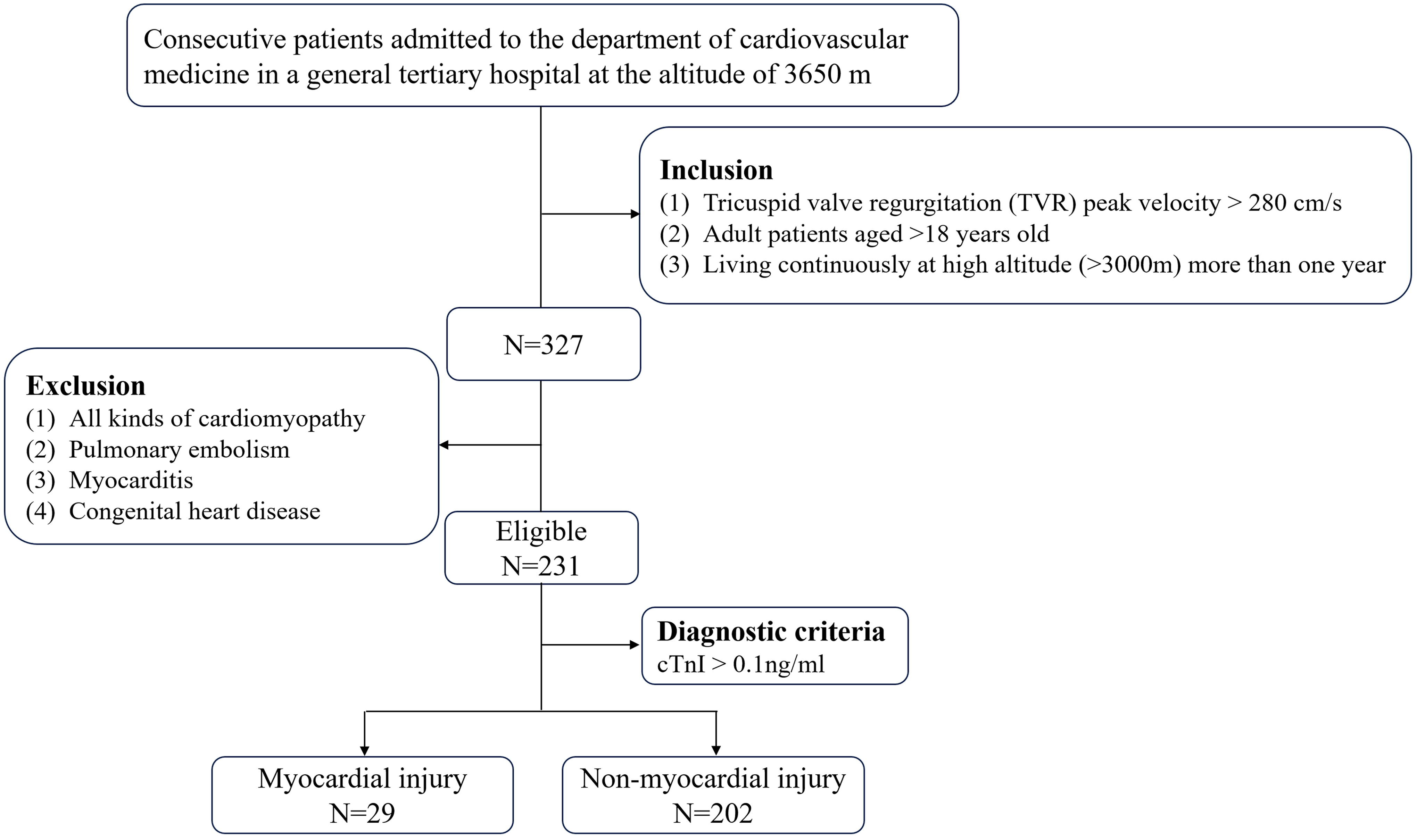
Flow chart of patients inclusion.
Comparisons of Clinical Data between MI Group and non-MI Group
ALT, alanine transaminase; ApoA1, apolipoprotein A1; ApoB, apolipoprotein B; APTT, activated partial thromboplastin time; AST, aspartate aminotransferase; BMI, body mass index; CK-MB, creatine kinase-MB; D-D, D-dimer; HDL-C, high-density lipoprotein cholesterin; HR, heart rate; LDL-C, low-density lipoprotein cholesterin; LDH, lactate dehydrogenase; LVEF, left ventricular ejection fractions; MI, myocardial injury; PDW, platelet distribution width; RBC, red blood cell count; PT, prothrombin time; RDW, red blood cell distribution width; TVR, tricuspid valve regurgitation.
Indicates significance at level 0.05.
Indicates significance at level 0.01.
Bold value indicates the difference is significant.
Correlation between cTnI and other myocardial enzymes
As Table 2 shows, the level of cTnI was positively correlated with the level of CK-MB (r = 0.571, p = 0.000) and LDH (r = 0.212, p = 0.001). There was no significant correlation between the level of AST and cTnI.
Correlation between cTnI and other myocardial enzymes.
CK-MB, creatine kinase-MB; AST, aspartate aminotransferase; LDH, lactate dehydrogenase.
Bold values indicate the difference is significant.
Diagnostic value of myocardial markers
ROC curves were drawn to evaluate the usefulness of classical myocardial markers including CK-MB, AST, and LDH in diagnosing myocardial injury, as shown in Figure 2. As shown in Table 3, only CK-MB had a significant diagnostic value in myocardial injury with AUC of 0.749 at the optimal cutoff value of 3.035 (p = 0.000). The sensitivity was 0.593, and the specificity was 0.905. AST and LDH had no diagnostic significance for myocardial injury in PH patients at high altitude.
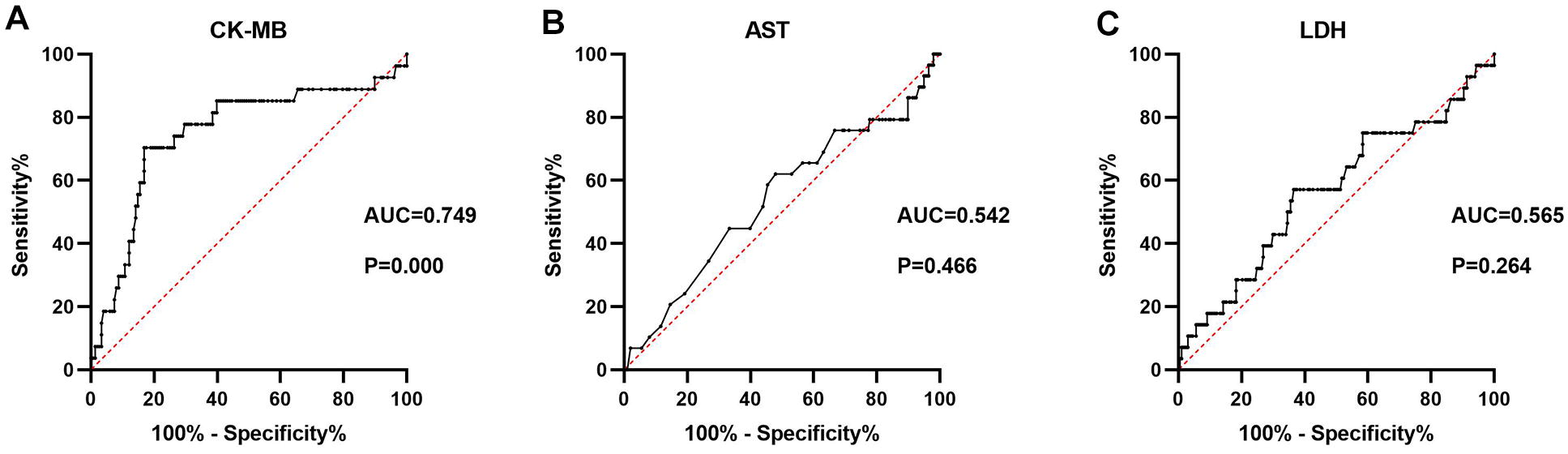
ROC curve for the values of
Diagnostic value of CK-MB, AST, and LDH for MI.
CK-MB, creatine kinase-MB; AST, aspartate aminotransferase; LDH, lactate dehydrogenase; MI, myocardial injury; AUC, area under curve.
Bold value indicates the difference is significant.
Discussion
Millions of tourists and climbers visit high altitudes annually, Where many healthy individuals may suffer from altitude illnesses such as acute mountain sickness (AMS), high-altitude cerebral edema, and high-altitude pulmonary edema, and notably, PH, which can eventually lead to right ventricle hypertrophy and heart failure (Pena et al., 2022). Furthermore, increased pulmonary artery pressures, acute hypoxia, increased myocardial work, and elevated epinephrine release may cause or exacerbate myocardial injury at high altitude (Higgins et al., 2010). At present, there are few studies focusing on myocardial injury with PH at high altitude. In the present research, the prevalence of myocardial injury was found to be 12.6%, which is lower than our previous study (He et al., 2021, He et al., 2023). One possible reason for the lower prevalence could be attributed to different diagnostic standards were used. Specifically, because of limitations imposed by the high-altitude environment in previous studies, CK, CK-MB, LDH, and AST were used for diagnosing myocardial injury, whereas cTnI was used in present study. Furthermore, altitude acclimatization may serve as a significant contributing factor. This study primarily included population with prolonged exposure to high altitude and indigenous population, thus potentially leading to adaptive changes in the cardiovascular system that enhance the tolerance of heart toward hypoxia. Adaptation to high-altitude hypoxia augments the cardiac resilience of highlanders against major detrimental consequences associated with acute hypoxia. The process of myocardial adaptation to high altitude involves crucial pathways such as hypoxia-inducible factor (HIF) pathway, mitochondrial synthesis pathway, blood oxygen transport pathway, tissue oxygen transport pathway, energy metabolism pathway, among others (Ostadal and Kolar, 2007). Evidence suggests that modifications of the HIF pathway are a crucial mechanism in altitude acclimatization. EGLN1 and EPAS1 encode key components of the HIF transcriptional pathway that coordinates an organism’s response to hypoxia (Petousi et al., 2014, Xiang et al., 2013, Xin et al., 2020). In a high-altitude hypoxic environment, the hearts initiate transcriptional programs to increase reliance on carbohydrates rather than fatty acid for ATP production, while also experiencing altered mitochondrial structure and function that improve metabolic efficiency and reduce ROS generation. In addition, beneficial changes occur in glycogen storage and high-energy phosphate system to regulate the balance between energy demand and supply when oxygen availability is limited (Su et al., 2021). In addition, Schweizer et al. (2019) reported that heart rate increased to improve the delivery of circulating oxygen at high altitude, whereas attenuation of catecholamine release improves tissue blood flow during hypoxia. The changes in Hb function, oxygen transport, and aerobic capacity under high altitude are crucial for hypoxic adaptation (Storz, 2021), including the evolution of higher rates of alveolar ventilation and respiratory oxygen uptake (Ivy and Scott, 2017), higher Hb O2 affinity (Storz et al., 2010), as well as altered skeletal muscle phenotypes enhance the ability of tissue O2 diffusion and O2 utilization (Mahalingam et al., 2017, Scott et al., 2015).
It is widely acknowledged that obesity has adverse effects on cardiovascular hemodynamics and cardiac structure and function, thereby increasing the incidence of adverse cardiovascular events (Lavie et al., 2017). Evidence suggests that obesity is a risk factors for AMS and is associated with its development (Caravedo et al., 2022). In the present study, myocardial injury group had a higher BMI than the non-myocardial injury group. Thus, elevated BMI may be a risk factor for myocardial injury exposed to high altitude. Previous study demonstrated that among individuals without cardiovascular disease, higher BMI was independently linearly associated with subclinical myocardial injury (Ndumele et al., 2014). Obesity leads to myocardial dysfunction by endocrine and inflammatory effects of adipose tissue (Martin et al., 2008). However, it is interesting to note that obesity appeared to be associated with a lower risk of death once cardiovascular disease is present (Buettner et al., 2007), which has been referred to as the “obesity para-dox” phenomenon (Hidvegi et al., 2020).
In this retrospective research, we also observed a significant alteration in LVEDD in myocardial injury with PH under high-altitude exposure. Left ventricular dilatation is typically the consequence of multiple pathological changes that occur during progressive heart failure-induced myocardial remodeling. Myocardial injury leads to outward remodeling of the left ventricular myocardium, resulting in left ventricular dilatation (Konstam et al., 2011). Our findings suggest that increased LVEDD in patients with myocardial injury may indicate the heart was going into the decompensation phase. Dilated LVEDD is related to left ventricular dysfunction and can serve as an indicator of advanced heart disease (Aleong et al., 2015). Furthermore, left ventricular dilatation independently predicts myocardial injury (Yeboah et al., 2014). Chen et al. (Chen et al., 2022) proposed that LVEDD may be used to identify heart failure patients who require more aggressive therapeutic interventions. In addition, left ventricular enlargement serves as an independent predictor for cardiovascular events among patients, and incorporating left ventricular volumes into left ventricular diameters increased the predictive value for cardiovascular outcomes (Ito et al., 2021). Therefore, screening for LVEDD dilatation in the general population at high altitude may identify a high-risk population for preventive treatment.
Troponin serves as a well-established biomarker for myocardial injury (Halvorsen et al., 2022). Consistent with expectations, our findings demonstrate that the disparity in troponin levels between the myocardial injury and non- myocardial injury cohorts is greater than that observed for CK-MB. This discrepancy arises primarily because of the higher molar mass of CK-MB compared with troponin. Consequently, troponin exhibits a higher propensity for release from stressed myocardial cells, even in instances where cellular integrity remains intact or apoptosis has commenced. In contrast, CK-MB is predominantly released following the occurrence of myocardial necrosis (Beranek, 2002, Wu, 2001). Although troponin has been regarded as the gold-standard biomarker for myocardial injury (Thygesen et al., 2012), alternative myocardial enzymes may prove beneficial in cases where troponin detection is not feasible. CK-MB is relatively specific for myocardial tissue, and its diagnostic value for myocardial infarction is highest when skeletal muscle injury or disease is excluded, but the expression of AST and LDH in a wide variety of tissues significantly affects its specificity for myocardial injury (Tilea et al., 2021). Our findings suggest that CK-MB and LDH were closely associated with the expression of cTnI. Furthermore, ROC curve was drawn to demonstrate that CK-MB level could predict the occurrence of myocardial injury with an AUC of 0.749 to a limited extent. Similarly, previous studies have suggested that CK-MB provides a reliable and specific diagnosis with high accuracy in the initial hours following cardiac symptoms onset (Danese and Montagnana, 2016). However, because of a lack of specificity in diagnosing acute myocardial infarction, AST and LDH were excluded (Penttilä et al., 2000). Thus, we suggest that CK-MB may serve as a valuable diagnostic marker when measuring cTnI proves challenging in high-altitude regions.
Conclusion
In conclusion, the incidence of myocardial injury with PH is significantly elevated in population at high altitude. Notably, BMI, LVEDD, and CK-MB levels exhibit significant alterations significantly in patients with myocardial injury associated with PH under high-altitude exposure. As a convenient marker, CK-MB was found to be closely associated with cTnI and have an effective diagnostic value in the high-altitude-induced myocardial injury with PH. However, the biggest limitation in our present study is that only patients with PH are included. Thus, further investigations are required to determine whether the findings can be extrapolated to the entire population at high altitude.
Publisher’s Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors, and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Footnotes
Authors’ Contribution
M.Z.: Data curation, formal analysis, and writing—original draft; Q.W.: data curation, validation, and visualization; W.D.: data curation and writing—original draft; J.S.: data curation and validation; W.Y.: data curation and validation; Y.S.: data curation and validation; X.Z.: formal analysis and writing—reviewing and editing; J.Z.: supervision, writing—reviewing and editing; and S.H.: conceptualization, supervision, funding acquisition, and writing—reviewing and editing.
Funding Information
This study was funded by Natural Science Foundation of Sichuan Province (No. 2022NSFSC1295), the 2021 Annual Project of the General Hospital of Western Theater Command (No. 2021-XZYG-B31).
Author Disclosure Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.