
Abstract

Residing at altitudes can lead to high-altitude pulmonary hypertension (HAPH) (Humbert et al., 2022; Singh et al., 1965). The simple electrocardiogram (ECG), due to its ubiquitous availability and easy and inexpensive performance, can contribute to the early diagnosis of HAPH in a high-altitude situation and ideally improve the prognosis of HAPH patients.
Case 1 is a 21-year-old man exposed to an altitude of 4,820 meters for 5 months. He experienced exertional dyspnea for about 1 month with no other uncomfortable symptoms. He was hypoxic (SpO2, 86% on ambient air). Cyanosis was observed on his lips. A hyperactive second heart sound of the pulmonary valve and a grade 3/6 systolic blowing murmur in the tricuspid auscultation zone was detected.
Case 2 is a 33-year-old man exposed to an altitude of 4,820 meters for 11 months. He experienced exertional dyspnea for about 5 months, along with dizziness and panic symptoms. His blood pressure was high (146/92 mmHg) and hypoxic (SpO2, 84% on ambient air). Cyanosis was observed on his lips, and the heart border widened to the sides. A hyperactive second heart sound of the pulmonary valve and general splitting were detected, along with a grade 4/6 systolic blowing murmur in the tricuspid auscultation zone.
Medical standard, resting 12-lead ECG was performed, and echocardiographic recordings were obtained based on the symptoms and physical examinations of the two cases. Figure 1A illustrates the right axis deviation in the QRS axis (112 degrees), an R/S ratio =1 in lead aVR, and TWI in leads V1–V3. Figure 1B demonstrates the right axis deviation in the QRS axis (179 degrees), an R/S ratio >1 in lead aVR, R wave in lead V1 > 5 mm, and TWI in leads V1–V3. Overall, TWI in leads V1–V3 is consistent across the two ECG readings.
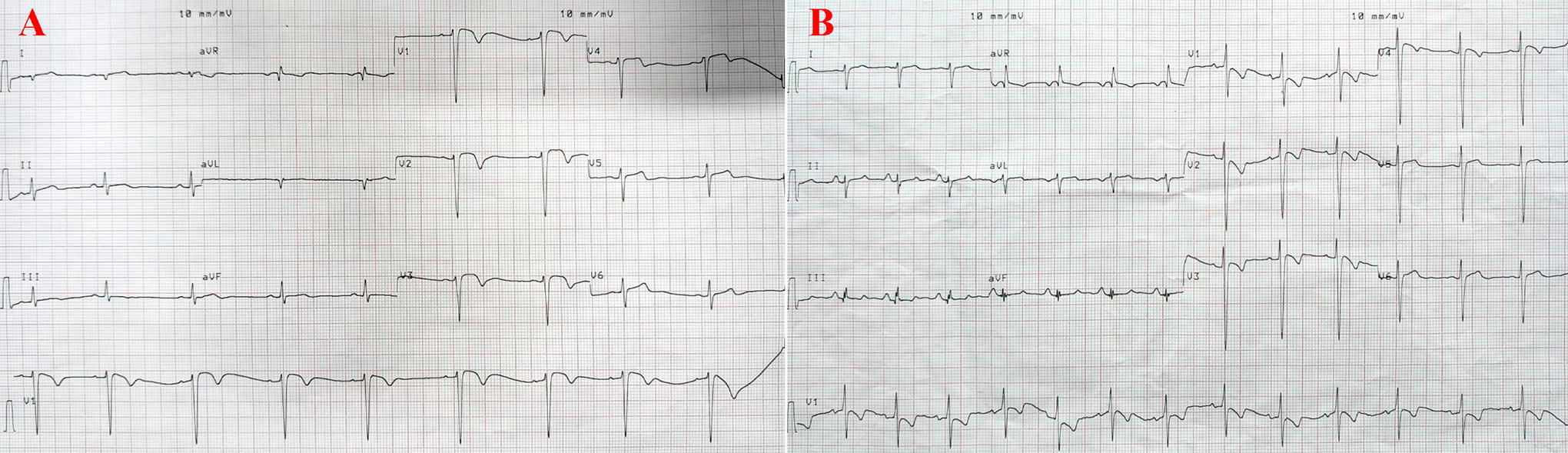
ECG of the two cases. A, Case 1; B, Case 2. ECG, electrocardiogram
The echocardiogram of the cases showed tricuspid regurgitation, elevated tricuspid regurgitation pressure gradient of 26 mmHg and 50 mmHg, respectively, and estimated pulmonary artery systolic pressure of 34 mmHg and 60 mmHg, respectively.
HAPH is a public health problem in mountainous areas worldwide. Timely identification of suspected HAPH and systematic screening of high-risk patient groups are crucial for early diagnosis and treatment. The lack of specialized equipment and technicians in the high-altitude environment makes right heart catheterization and cardiac ultrasound often unavailable for practical use in HAPH screening. Therefore, due to its ubiquitous availability and easy and inexpensive performance, the simple ECG assessment is a good alternative approach to the early diagnosis of HAPH in a high-altitude situation.
ECG has been used in the research of HAPH in many studies (Aeschbacher et al., 2020; Negi et al., 2014; Rotta and Lopez, 1959; Singh et al., 1965).
TWI is an important indicator of ventricular repolarization dysfunction and may represent the initial expression of underlying cardiomyopathies. However, there have been few reports on TWI in individuals with HAPH. This study found two young Chinese males with TWI in leads V1–V3 after exposure to an altitude of 4,820 m for 5 and 11 months, respectively (Fig. 1). The echocardiogram of the two cases indicated HAPH.
The prevalence of TWI in leads V1–V2 among individuals from an altitude of 3,000–4,200 m was 1.5% (Negi et al., 2014), which is lower than the rate observed in our study (2 out of 39). The variance in altitude between our study (4,820 m) and the study conducted by Negi et al. (3,000–4,200 m) may have contributed to this difference.
Based on a previous study (Singh et al., 1965), we also observed that subjects with an exposure duration of 5 months developed HAPH. While genetic predisposition is likely a significant factor in increasing the risk of HAPH in high-altitude residents, the duration of exposure to high altitudes may also be a contributing risk factor for the development of HAPH (Negi et al., 2014). Therefore, we believe that screening for HAPH in individuals exposed to high altitudes using ECG should be conducted whenever possible, particularly when the duration of high-altitude exposure is <5 months, to facilitate early detection of suspected HAPH. In the future, a more comprehensive investigation concentrating on TWI in leads V1–V3 might be advantageous to identify HAPH in a high-altitude setting.
Footnotes
Authors’ Contributions
X.T. and L.L.: Conception and design, development of methodology; X.T., Z.W., X.W., and R.Z.: acquisition of data (acquired and managed patients, provided facilities, etc.); X.T., J.W., and L.L.: analysis and interpretation of data; X.T., J.W., and L.L.: writing, review, and/or revision of the article; X.T. and L.L.: administrative, technical, or material support; L.L.: study supervision.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study did not receive any grant funding.