
Abstract
Van Ochten, Natalie, Eric W. Rudofker, and William K. Cornwell. Altitude adversities: is it safe for people with cardiovascular disease to travel to moderate-high altitude? High Alt Med Biol. 26:328–334, 2025.—The risk of acute cardiac events increases following acute exposure to hypoxia associated with travel to moderate-high altitudes. Herein, we present seven illustrative cases among lowlanders who presented to our center (1,609 m, equivalent fraction of inspired oxygen [FIO2] ∼0.17) with acute cardiac emergencies during travel to moderate-high altitude. We also provide a concise, yet comprehensive, review of the relevant physiology pertaining to the impact of acute hypoxia on cardiovascular physiology and mechanisms by which altitude exposure may increase the risk of adverse events.
Introduction
Over 100 million people travel to mountainous areas annually for work or pleasure (Cornwell et al., 2021). Oxygen availability is reduced at popular tourist destinations located at moderate (2,000–3,000 m) and high (3,000–5,000 m) altitudes compared to sea level (Table 1). Approximately 108 million individuals in the United States have hypertension, 18.2 million have coronary artery disease (CAD), and 6.2 million have heart failure (NIH, 2022). These individuals, when acutely exposed to hypoxia, are at risk of adverse cardiac events. There is an inverse relationship between elevation above sea level and the partial pressure of oxygen. Air travel is one common example of acute altitude exposure, as commercial aircraft cabin environments are pressurized to a maximum of 2,438 m, a fraction of inspired oxygen (FIO2) of ∼0.15. Pre-travel medical consultation before flying or visiting a moderate-high altitude destination is not common, although individuals with pre-existing cardiovascular diseases are at high risk for suffering adverse events during or following acute altitude exposure. In this retrospective case series, we present several illustrative cases of cardiovascular complications that occurred during acute hypoxic exposure among lowlanders traveling to higher altitudes. These cases are meant to raise awareness surrounding an underappreciated but clinically important problem—namely, that patients with cardiovascular disease and/or risk factors may be at an increased risk of major adverse cardiovascular events following exposure to hypoxia.
Altitude Classifications with Respective Percent Reduction in Functional Capacity According to Maximal Oxygen Consumption (VO2max) as Altitude Increases and Associated Reductions in the Fraction of Inspired Oxygen (FIO2) Relative to Sea Level
Examples of popular travel destinations are provided.
Case 1
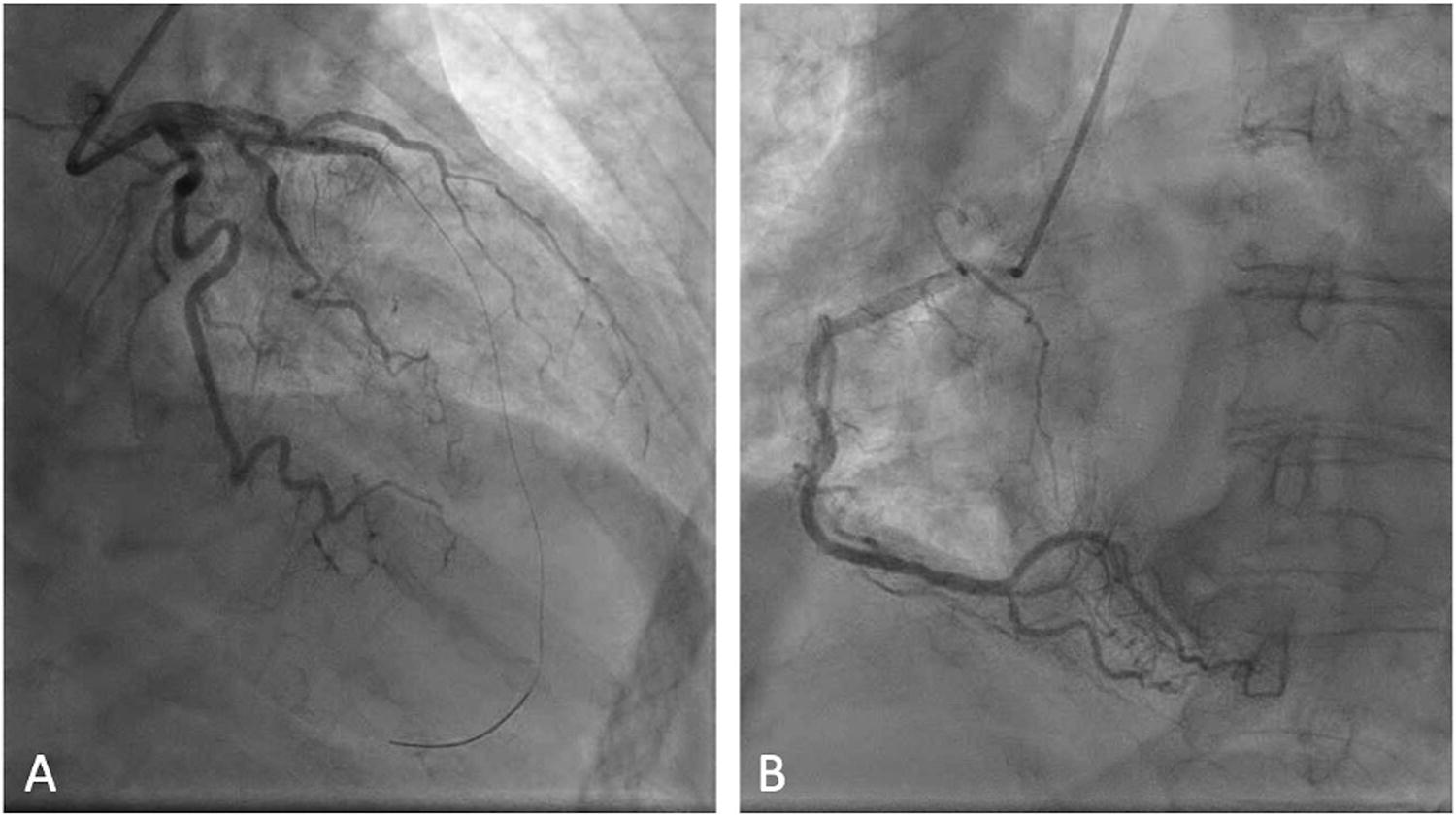
A 63-year-old woman with type two diabetes mellitus (hemoglobin A1c 10.7%) was visiting Durango, Colorado (1,985 m), from Maryland (106 m). After two days of exposure to altitude, she developed chest tightness, nausea, and diaphoresis. At a local emergency department (ED), she was hemodynamically stable and was given fluids, inhaled albuterol, and a recommendation to seek lower altitude (no electrocardiogram [ECG] or troponin was completed at that time). Four days later at Denver International Airport (1,609 m), in anticipation of traveling home, she developed severe chest pain and was transported to our ED. On arrival, ECG was consistent with anterior ST-segment elevation myocardial infarction (STEMI). Initial hs-troponin-I was 1,236 ng/l and peaked at 9,950 ng/l (Fig. 1). She was in cardiogenic shock as evidenced by hypotension and a lactate of 3.5 mmol/l. Coronary angiogram demonstrated a patent proximal left anterior descending (LAD) that terminated with a thrombotic occlusion and nonobstructive disease of the right coronary artery (RCA) and circumflex. Balloon angioplasty and thrombectomy were performed, but thrombolysis in myocardial infarction 0 flow remained (Fig. 2). A transfemoral Impella CP was placed for hemodynamic stabilization, later upgraded to a transaxillary Impella 5.5, and eventually veno-arterial extracorporeal membrane oxygenation (VA-ECMO) for hemodynamic support. Heart transplant evaluation was initiated, but due to a progressive decline in status, the family withdrew care, and she died after 6 days of hemodynamic support.
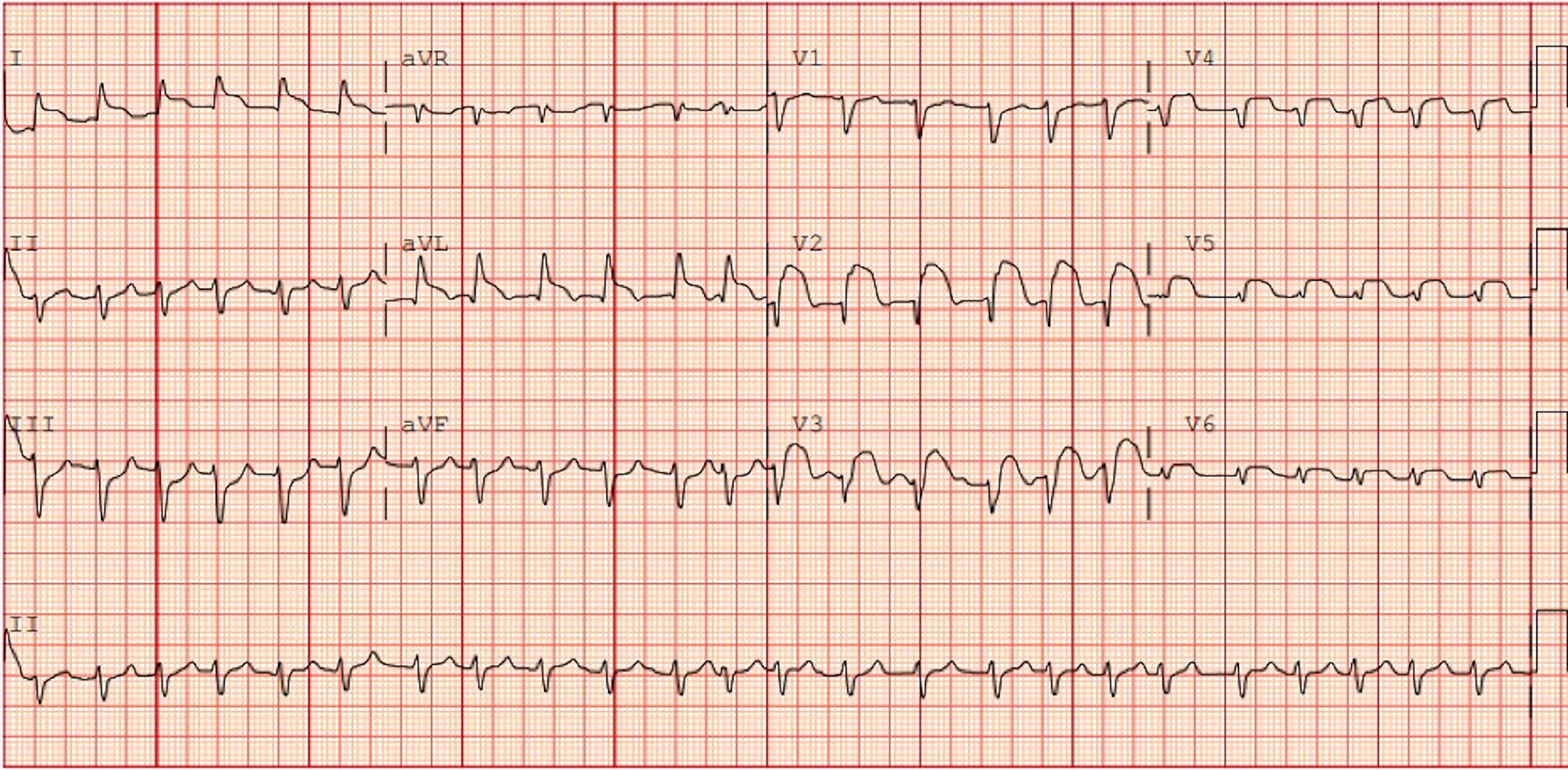
ECG at presentation notable for ST-segment elevations concerning for an anterior STEMI. ECG, electrocardiogram; STEMI, ST-segment elevation myocardial infarction.
(
Case 2
A 38-year-old man with type two diabetes mellitus (hemoglobin A1c 12.2%) was visiting Denver, Colorado (1,609 m), from San Antonio, Texas (202 m). After staying in Denver for approximately four weeks, he presented to the ED with acute chest pain and dyspnea. ECG suggested anterior STEMI (hs-troponin-I >125,000 ng/l, peak >270,170 ng/l). Labs were notable for glucose 738 mg/dl and pH 7.23, suggesting diabetic ketoacidosis. He was also in cardiogenic shock with lactate 10.8 mmol/l and mean arterial pressure <65 mmHg. Emergent coronary angiogram revealed a 100% occlusion of the mid-LAD [successful percutaneous coronary intervention (PCI) was performed] and chronic total occlusion (CTO) of the mid-RCA, obtuse marginal (OM) 1, and OM2 (Fig. 3). Transfemoral Impella was placed due to worsening hemodynamics, and he was intubated for airway protection and hypoxemia. On arrival to the intensive care unit, he developed ventricular fibrillation with return of spontaneous circulation after receiving two minutes of advanced cardiac life support, and VA-ECMO was initiated. He required continuous renal replacement therapy for acute kidney injury. Emergent evaluation for advanced therapies was completed; however, he was determined to not be a candidate for heart transplant or left ventricular assist device due to multiple comorbidities, including uncontrolled diabetes, severe right ventricular dysfunction, and acute kidney injury. After family meetings and shared decision-making, he was transitioned to comfort care and died after 25 days of hemodynamic support.
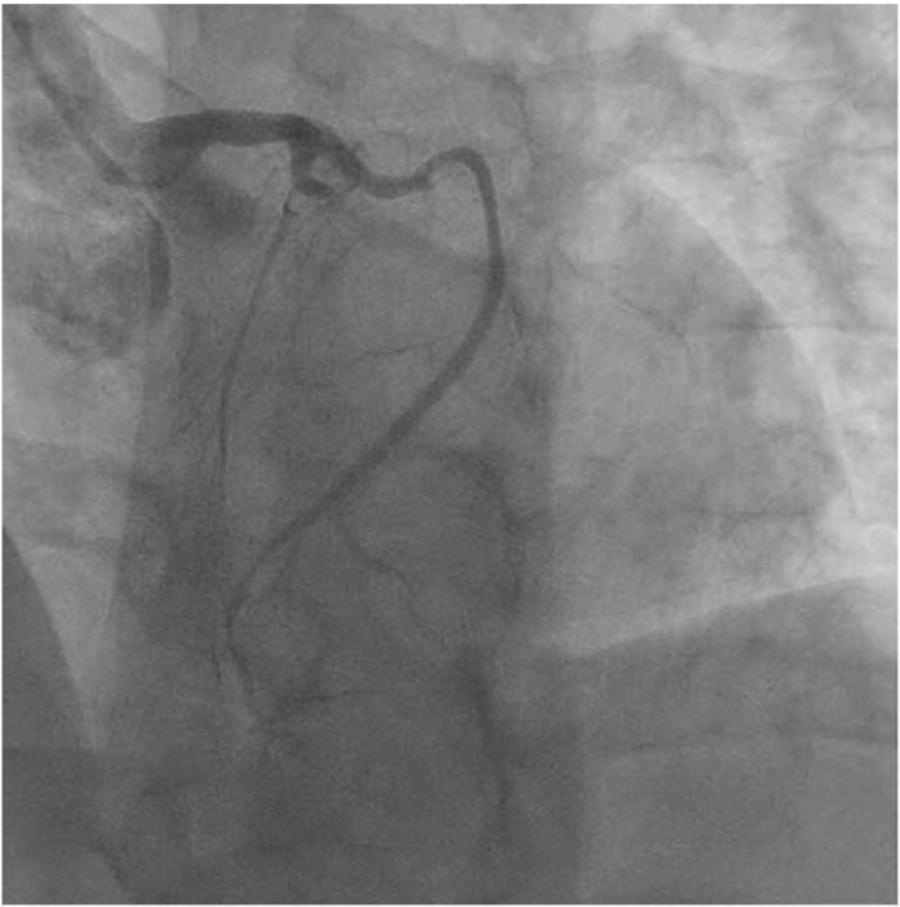
Coronary angiography demonstrating a 100% occlusion of the mid-LAD and CTO of the mid-RCA, OM1, and OM2. CTO, chronic total occlusion; OM, obtuse marginal.
Case 3
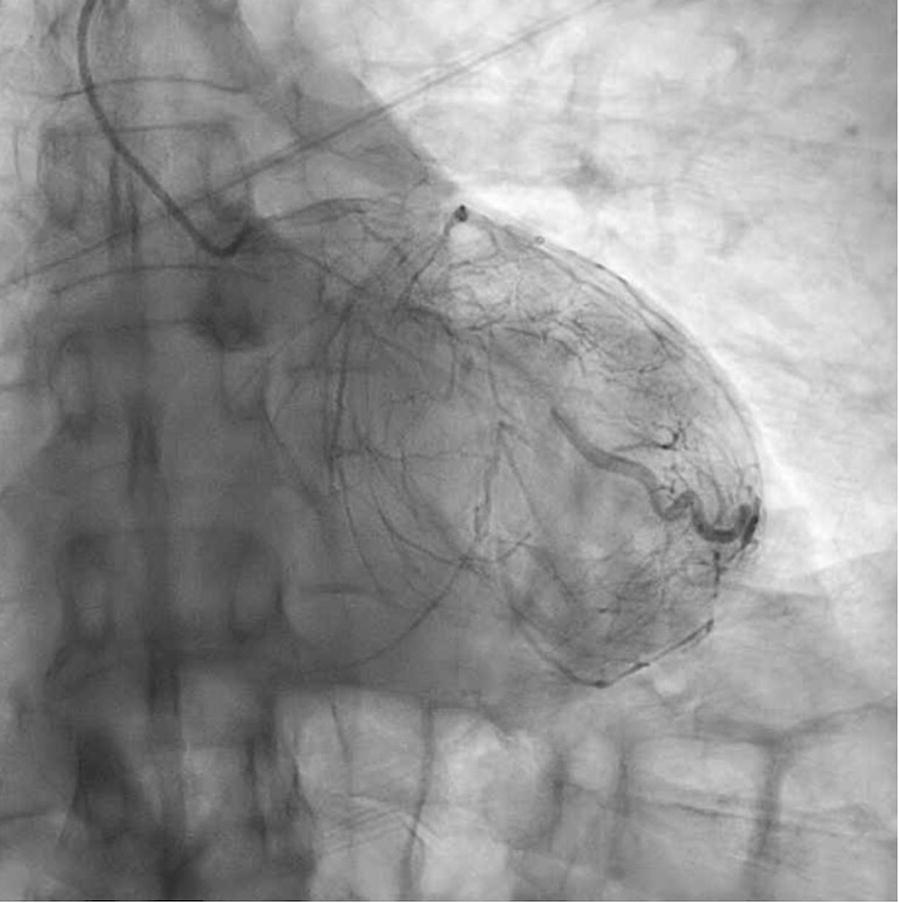
A 78-year-old man with hypertension and type two diabetes mellitus (hemoglobin A1c 8.0%) traveling from Fort Myers, Florida (sea level), developed exertional chest pain immediately after landing at Denver International Airport. One month prior to travel, he had undergone a coronary angiogram for evaluation of near-syncopal events, which demonstrated severe multivessel coronary artery disease with severe mid-LAD and diagonal artery stenoses, severe mid-circumflex stenosis, and severe posterior descending artery (PDA) disease. He presented to our ED for evaluation of chest pain and was hemodynamically stable. Hs-troponin-I was 126 ng/l and increased to a peak of 2,210 ng/l. ECG demonstrated right bundle branch block and Q waves in V3-V4. Transthoracic echocardiogram (TTE) revealed a left ventricular ejection fraction (LVEF) of 37% with akinesis of the mid-inferior wall, dyskinesis of the entire apex, a severely calcified mitral valve with moderate-to-severe mitral stenosis, and moderate tricuspid regurgitation. Prior TTE in Florida was notable for LVEF of 55–60% with no wall motion abnormalities. Brain natriuretic peptide was 1,035 pg/ml. Coronary angiogram was repeated at our institution and was consistent with his prior study without a clear culprit lesion or intervenable target (Fig. 4). He was found to have a porcelain aorta, and after multidisciplinary discussion with the patient and his family, non-surgical management was pursued. He was discharged on guideline-directed medical therapy and dual antiplatelet therapy for management of heart failure with reduced ejection fraction and non-STEMI, respectively.

Coronary angiography noting severe multivessel coronary artery disease with severe mid-LAD and diagonal stenoses, severe mid circumflex stenosis, and severe PDA disease. PDA, posterior descending artery.
Case 4
A 72-year-old man with hypertension presented from Denver International Airport with acute onset of presyncope during a layover from Washington, DC (125 m) to Maui, Hawaii. A similar episode had occurred one month prior to travel without cardiac evaluation. In the ED, the ECG showed dynamic ST-segment depressions, and the initial hs-troponin-I was 88 ng/l, increasing to a peak of 3,871 ng/l. An echocardiogram was unremarkable; LVEF was 58% without wall motion abnormalities. A coronary angiogram was performed and notable for severe three-vessel disease (mid-LAD CTO, diagonal 1 80%, OM1 70%, mid-left circumflex CTO, and RCA serial severe proximal and distal severe 80% stenoses) (Fig. 5). On hospital day 3, he underwent successful coronary artery bypass grafting (CABG) [left internal mammary artery to LAD, saphenous venous graft (SVG) to OM, SVG to PDA]. He was eventually discharged back to his home in Washington, DC, on hospital day 8.
Coronary angiography with severe multivessel coronary artery with high anatomical complexity: mid-LAD CTO, diagonal 1 80% stenosis, OM1 70% stenosis, mid-LCx CTO, and RCA serial severe proximal and distal severe 80% stenoses. LCx, mid-left circumflex.
Case 5
A 76-year-old man with a prior CABG in 2014 from Clearwater, Florida (9.1 m) presented from Denver International Airport with acute onset of chest pain after rushing to his gate for a flight connection. ECG suggested inferior STEMI; initial hs-troponin-I was 8,756 ng/l and rose to a peak of 11,801 ng/l. Coronary angiogram was notable for chronic total occlusion of a dominant RCA, aneurysmal disease of the left main coronary artery, and plaque rupture with subtotal occlusion of the distal SVG supplying the PDA. PCI was performed, and he was discharged on hospital day 2 after an unremarkable course.
Case 6
A 69-year-old man with hyperlipidemia and hypertension presented to our center after suffering an in-flight episode of unresponsiveness while en route from Chicago, Illinois (182 m) to San Jose, California, requiring emergency diversion to Denver International Airport. He had known aortic stenosis, graded as moderate to severe on an echocardiogram performed shortly before travel (maximum aortic valve velocity [AVmax] 3.78 m/s, mean gradient 33 mmHg, dimensionless index [DI] 0.23, aortic valve area [AVA] 1.02 cm2), and was notable for moderate aortic regurgitation with preserved systolic function (LVEF 67%). In flight, he received approximately 10 minutes of bystander cardiopulmonary resuscitation before regaining consciousness. At our facility, repeat echocardiogram suggested bicuspid aortic valve morphology with severe aortic stenosis (AVmax 4.9 m/s, mean gradient 57 mmHg, DI 0.20, AVA 0.57 cm2) with moderate to severe aortic regurgitation and normal systolic function. He underwent successful surgical aortic valve repair on hospital day 7 and was discharged to return home to Illinois on hospital day 12.
Case 7
A 68-year-old man with no prior medical history traveled from his home in Nashville, Tennessee (159 m), to Winter Park, Colorado (2,759 m), for recreational downhill skiing. He developed an upper respiratory infection after arriving. During his first day of skiing at Winter Park, he developed acute retrosternal chest pressure and sought care at a local ED. The initial ECG was normal, and point-of-care troponin-I was initially 0.05 ng/ml but rose to 0.30 ng/ml one hour later, prompting emergent transfer to a PCI-capable center in Denver, Colorado. There, hs-troponin-I was 8,004 ng/l, peak 13,515 ng/l. A repeat ECG did not show any dynamic ST-segment changes or evidence of acute infarction. However, the coronary angiogram demonstrated a subtotal thrombotic occlusion of the proximal LAD, with mild to moderate residual disease in the distal LAD and no other atherosclerosis. He underwent PCI without complication. Echocardiogram demonstrated mild left ventricular hypertrophy, LVEF 54% with hypokinesis of the LAD territory, and no valvular abnormalities. He was discharged on dual antiplatelet therapy and metoprolol succinate and returned to his home several days later.
Discussion
As our case series demonstrates, cardiovascular events may occur during, or in response to, a number of scenarios, including brief layovers in airports at increased altitudes, en route to destinations during cross-country flights, or shortly after arrival to higher altitude environments (Table 2). Each 100 m increase in altitude over 1,500 m leads to a 1% decrease in maximal oxygen uptake (Erdmann et al., 1998). While healthy individuals often compensate well in response to hypoxia, those with cardiovascular disease and/or risk factors may have difficulty completing basic activities of daily living in moderate to high altitude environments (Erdmann et al., 1998).
Summary of Characteristics of Each Patient in Cases 1–7, Their Significant Interventions, and Their Outcomes
CABG, coronary artery bypass grafting; MCS: mechanical circulatory support; NSTEMI, non-ST elevation myocardial infarction; OM, obtuse marginal; PCI, percutaneous coronary intervention; SAVR, surgical aortic valve repair; STEMI, ST-segment elevation myocardial infarction.
Among individuals without heart disease, traveling to moderate to high altitude causes coronary artery vasodilation, and thus, increased coronary blood flow; however, those with CAD may exhibit paradoxical vasoconstriction of these vessels at altitude, increasing the likelihood of a coronary stenosis becoming ischemic at altitude that would have otherwise been asymptomatic at sea level (Levine, 2015; Levy et al., 1938). It has been previously recommended that following revascularization of CAD, patients should wait at least 6 months before traveling to altitude (Cornwell et al., 2021; Dehnert and Bärtsch, 2010; Erdmann et al., 1998).
The acute response to hypoxia is dominated by a chemoreceptor-mediated increase in sympathetic tone that increases in concert with the degree of hypoxia (Levine, 2015). The increased sympathetic tone increases heart rate, stroke volume, and cardiac output. This increase in sympathetic tone, combined with other physiological responses to hypoxia, such as hypoxic pulmonary vasoconstriction, may not be tolerated by patients with cardiovascular disease and, more specifically, heart failure and pulmonary hypertension (Cornwell et al., 2021). It is well established that transient hypotension occurs in healthy individuals due to arterial vasodilatation, which may precipitate heart failure decompensation in patients with inadequate contractile reserve owing to baseline left ventricular systolic dysfunction. Environmental factors (thermal stress, dehydration) and exercise all work together to increase external stress placed on the cardiovascular system at higher altitudes.
There are some data to suggest that hypoxia reduces platelet count and promotes platelets aggregation (Chen et al., 2016). These observations raise concern that hypoxia may increase the risk of ACS (Chen et al., 2016). However, data are insufficient to determine whether hypoxia promotes a prothrombotic state or could cause a stable coronary plaque to become unstable. That said, providers should recognize at-risk patients may still be at an increased risk of adverse cardiovascular events. More data on the specific impact of hypoxia on platelet activity, the coagulation cascade, and the characteristics of coronary plaque are needed.
Syncope is another common symptom associated with acute exposure to even moderate altitude, frequently occurring <24 hours after ascent. Syncope at altitude is usually benign and results from hypoxia-induced vasodilation, compounded by cerebral vasoconstriction from hyperventilation-induced hypocapnia (Nicholas et al., 1992). Additionally, post-exertional syncope, which occurs at sea-level, may also occur at altitude as a result of exercise-induced vasodilation (Nicholas et al., 1992). Patients with aortic valve disease, such as case 6 above, have a fixed outflow obstruction and may lack the ability to sufficiently augment cardiac output in response to a reduction of systemic vascular resistance, leading to an overt syncopal event.
Travel itineraries should include an acclimatization period immediately after arrival to altitude and precede exercise in hypoxic environments (Cornwell et al., 2021). The Tenth Mountain Division Study showed that compared to exercise at low altitude/sea level, exercise during acute hypoxic exposure (2,480 m) lowered the ischemic threshold (Levine et al., 1997). However, after a five-day period of acclimatization to 2,500 m, the ischemic threshold normalized compared to sea-level conditions (Levine et al., 1997). Additionally, a study of 301 sudden cardiac deaths among subjects traveling to the Austrian Alps for mountaineering activities found half of the events to occur within the first day of activity at altitude, with the risk of sudden cardiac death significantly decreased by spending one night sleeping above 1,000 m (Lo et al., 2013). Risk factors for sudden cardiac death include previous myocardial infarctions, CAD risk factors, intense physical activity before acclimatization, and poor food and water intake (Burtscher, 2017).
The physiological response to hypoxia may increase the risk of adverse cardiac events. Outcomes following acute events that occur at altitude may be compromised if travel is to a remote area with limited access to care. As such, providers and patients should work to optimize medical therapy, treat any uncontrolled symptoms, and develop travel itineraries incorporating acclimatization periods and identifying access points for care in case of an event during travel (Fig. 6). Additional considerations for pre-travel planning include identifying plans for descent, bringing additional medications, and identifying wearable technologies that may assist in monitoring (e.g., heart rate and oxygen monitors, blood pressure cuffs) that may provide helpful information while at altitude.
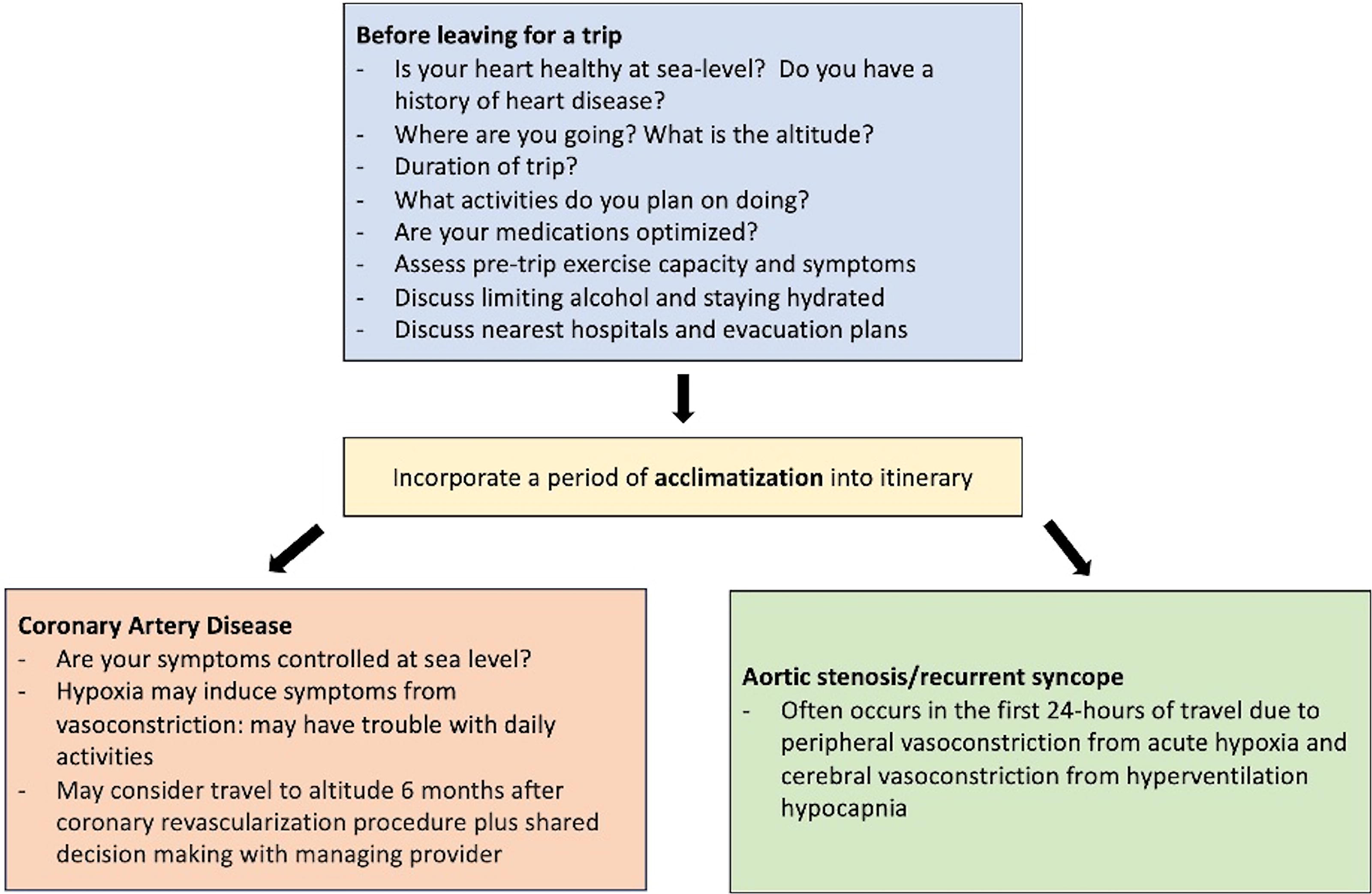
Pre-travel considerations for physicians to discuss with their patients with coronary artery disease or aortic stenosis/recurrent syncope before traveling to altitude.
There are limitations to this article. First, this is a retrospective case series, and as such, we are unable to establish causation. However, it is plausible that the very well-described physiological response to hypoxia may increase the risk of major adverse cardiovascular events in at-risk populations. Our case series supports this concept and demonstrates that individuals with either established disease or risk factors may be at an increased risk of adverse events when traveling to higher altitudes. Second, our case series, by definition, is small and may be limited in generalizability. However, our intent was to present illustrative cases of patients with a diversity of backgrounds related to a history of cardiovascular disease, and in this regard, this series is very illustrative. Specifically, our data suggest that patients with comorbidities such as valvular disease, a history of atherosclerotic cardiovascular disease, or risk factors such as uncontrolled diabetes may be at an increased risk of adverse events. Larger studies are required to establish a causal role. In addition, future prospective studies on this topic are needed to further define the specific impact of acute hypoxia on patients with established cardiovascular disease and/or risk factors.
In conclusion, patients with established cardiovascular disease and/or risk factors may be at an increased risk of adverse cardiovascular events when exposed to hypoxia, such as occurs when traveling to high altitude environments. Pre-travel arrangements should include an evaluation to ensure that risk factors are optimized, and travel itineraries should include a period of acclimatization to further reduce this risk.
Footnotes
Acknowledgment
The authors would like to express a deep gratitude for the patients and families who provided permission to use their cases in this article and the wonderful faculty and staff who helped care for them in the hospital.
Consent
Verbal and written consent was obtained from each patient, or a patient’s original MDPOA if they had passed away.
Authors’ Contributions
N.V.O.: Conceptualization, investigation, data curation, writing original draft, visualization, project administration. E.R.: Conceptualization, validation, writing review and editing, supervision. W.C.: Conceptualization, validation, writing review and editing, supervision, project administration.
Author Disclosures Statement
The authors have nothing to disclose.
Funding Information
There was no funding for this work.