
Abstract
Su, Ping, Masako Taniike, Yuko Ohno, and Ikuko Mohri. The effects of high altitude on children’s sleep: a community-based study on preschoolers in the Tibetan Plateau. High Alt Med Biol. 26:187–194, 2025.
Objective/Background:
It has been reported that high altitude affects breathing during sleep in children. To evaluate the symptoms suspected sleep-disordered breathing (SDB) and sleep quality of preschool children living in high altitude of 2,261–3,800 m above sea level (masl) in the Tibetan Plateau, we conducted the community-based survey using a questionnaire.
Patients/Methods:
Sleep problems were assessed in 3,113 children aged 3–6 years in Qinghai province using the Chinese version of the Japanese Sleep Questionnaire for Preschoolers (JSQ-P-C), focusing on obstructive sleep apnea (OSA) and OSA-related symptoms. The effect of altitude on these scores was analyzed.
Results:
The subscale scores of OSA, morning symptoms, and daytime excessive sleepiness in the JSQ-P-C were higher in children living in areas above 3,000 masl than in those living below 3,000 masl and in Japanese children. Altitude, but not family income or maternal education level, significantly affected the scores of OSA, morning symptoms, and daytime excessive sleepiness.
Conclusions:
Living at altitudes higher than 3,000 masl may adversely affect children’s sleep quality.
Introduction
Children have longer nocturnal sleep duration and deeper sleep compared with adults (Roffwarg et al., 1966), emphasizing the importance of sleep during brain development (Wang et al., 2011). Sleep deprivation leads to difficulties in concentration, impulse control, and goal-directed behaviors (Arnedt et al., 2005); impaired emotional control (Zohar et al., 2005); and memory formation and consolidation (Yoo et al., 2007). Therefore, nocturnal sleep abnormalities in early childhood have been associated with subsequent hyperactivity (Touchette et al., 2009) and cognitive dysfunction later in life (Suzuki et al., 2005). In addition, children with obstructive sleep apnea (OSA) and resultant poor sleep quality exhibit more behavioral problems during the day, such as hyperactivity, impulsivity (American Academy of Sleep Medicine, 2005), and poorer academic performance (O’Brien & Gozal, 2002). Sleep-related breathing disorders showed adverse effects on neurocognitive function in children (Hunter et al., 2016).
In high-altitude areas, hypoxia is caused by a decrease in atmospheric pressure. The oxygen concentration was ∼21% in the plains and high-altitude areas. However, the partial pressure of oxygen decreased at higher altitudes from 159 mmHg in the plains to 115 mmHg at 2,000 m and 111 mmHg at 3,000 m. Decreased partial pressure of oxygen leads to hypobaric hypoxia. At high-altitude areas, hypoxia causes compensatory hyperventilation, which causes hypocapnia. Hypocapnia results in hypoventilation and hypoxia (Taylor, 2011). If periodic breathing (PB) and breathing instability, with periods of deep and rapid breathing alternating with central sleep apnea, occur, blood CO2 levels can drop to extremely low levels, which can switch off the drive to breathe. Breathing begins again only after the body senses a further decrease in oxygen levels. PB arises from an instable control system through a hypoxic drive or response to CO2 (Johnson et al., 2010; Weil, 2004). In patients with OSA, hypobaric hypoxia promotes frequent central apneas besides obstructive events, resulting in more severe respiratory compromise (Bloch et al., 2015).
Several sleep questionnaires, such as the Children’s Sleep Habit Questionnaire (Owens et al., 2000), the Pediatric Sleep Questionnaire (Chervin et al., 2000), and the Sleep Disturbance Scale for Children (Bruni et al., 1996), have been developed for clinical and research purposes in Western countries. However, these questionnaires were originally developed in the context of Western sleep culture. Since sleep is largely influenced by environmental factors, such as lifestyle or sleep culture, these questionnaires may not fully capture important cultural differences. For example, cosleeping or sharing a room or bedding is common in many Asian countries. The Japanese-style “futon” bedding facilitates movement to the parents’ “futon” during sleep. In this context, bedtime resistance is more common among infants and preschoolers who share a bed or room (Latz et al., 1999). Therefore, we developed the Japanese Sleep Questionnaire for Preschoolers (JSQ-P), which is adapted to the Japanese sleep culture and enables the detection of sleep disorders and problematic sleep habits (Shimizu et al. 2014). The JSQ-P consists of (1) demographic data, such as bedtime, wake time, dinner time, TV time, and gaming time, and (2) 39 items on sleep-related behaviors observed by the child’s parent. Participants complete the 39 items by rating them on a 6-point Likert scale, as previously described (Shimizu et al., 2014). The 39 items were classified into 10 subscales: I, Restless Legs Syndrome (RLS) Sensory Symptoms; II, RLS-Motor Symptoms; III, OSA; IV, Parasomnias; V, Insomnia/Circadian Rhythm Disorder; VI, Morning Symptoms; VII, Daytime Excessive Sleepiness; VIII, Daytime Behaviors; IX, Sleep Habits; and X, Insufficient Sleep (Supp table). The JSQ-P has been used to study the sleep habits of Japanese preschoolers (Mituboshi et al., 2012), assess sleep problems in children with developmental disabilities (Hirata et al., 2016), investigate the prevalence of bruxism (Tachibana et al., 2016), and conduct an international comparison between Malaysia and Japanese preschoolers (Jayanath et al., 2022).
Qinghai province is in the eastern hinterland of the Qinghai–Tibet Plateau in western China at an altitude of 2,000 m above sea level (masl). Tibetan children also have a cosleeping culture; therefore, we assessed the sleep habits of Tibetan preschoolers using the Chinese version of the JSQ-P (JSQ-P-C), which was developed by translating the JSQ-P into Chinese and confirming its accuracy by backtranslating as previously described (Su et al., 2022).
In this study, we conducted a community-based evaluation on the effect of high altitude on sleep quality in preschooler children using the JSQ-P-C.
Participants and Methods
Participants
A total of 3,113 children aged 3–6 years attending kindergartens in four cities in Qinghai province, People’s Republic of China, namely Xining City, Gonghe County, Xinghai County, and Maqin County, were included in the study. Xining is the capital of Qinghai province and is located at an altitude 2,261 masl. Gonghe, Xinghai, and Maqin are located at 2,862, 3,303, and 3,800 masl, respectively. In Xining and Gonghe, which are below 3,000 masl, the resting peripheral capillary oxygen saturation (SpO2) is >90%. In contrast, in Xinghai and Maqin, which are above 3,000 masl, the resting SpO2 is <90% (Andrade et al., 2020; Subhi et al., 2009).
The survey was administered in kindergartens, where the principals agreed to distribute the questionnaires after explanation by the researchers. In the districts included in this study, almost all children attended kindergartens. The children’s caregivers were informed that participation was free; they were asked to complete the questionnaire anonymously and to return it 2 days later. Submission of the questionnaire was considered consent to participate. The survey was conducted between mid-September and mid-October 2019, a relatively stable period with fewer school events and community festivals.
To make an international comparison between Asian countries, we used data from Tibetan children and data from Japanese children who were aged 3–6 years (n = 2,553), as previously reported (Shimizu et al., 2014).
Because high altitude leads to lower partial oxygen pressure, OSA and sleep quality may be exacerbated in children living in highland. To investigate whether higher altitude affects OSA and sleep quality, we compared the total scores of three JSQ-P-C subscales, such as OSA, Morning symptoms and Excessive daytime sleepiness, between areas above 3,000 masl (Xinghai and Maqin), high altitude but below 3,000 masl (Xining and Gonghe) and low altitude (Japan).
The study protocol and questionnaire were approved by the Human Research Ethics Committee of the Institutional Review Board of Osaka University Hospital (#19007). This study was conducted in accordance with the code of ethics for experiments involving human subjects as defined by the Declaration of Helsinki for experiments involving humans.
Measurements
Because high altitude affects OSA (Pagel et al., 2011; Block et al., 2015), we focused on sleep-disordered breathing (SDB)-suspect symptoms using subscales: III, OSA; VI, morning symptoms; and VII, daytime excessive sleepiness of the JSQ-P-C. Subscales VI and VII were selected because they are directly affected by OSA symptoms or insufficient sleep in children. The items for subscales III, VI, and VII are shown in Supplementary Table S1.
Statistical analysis
Sleep-related life schedules were compared among three age groups of children in Qinghai using the Fisher’s least significant difference test. Effect sizes (Cohen’s d) were calculated for variables with significant differences. Sleep and sleep habits were compared among the four areas in Qinghai province using the chi-squared test and the Kruskal–Wallis test. Sleep and sleep habits were compared between 3-year-old children in Qinghai province and Japan using the Mann–Whitney U test. After calculating the sum of the scores for each subscale, we compared the scores and effect sizes (η2) between the four areas using analysis of variance (ANOVA).
Potential interaction effects of three independent variables, such as altitude, maternal education, family income with nocturnal sleep time, TV-viewing time, gaming time, the scores of OSA, morning symptoms, and daytime excessive sleepiness of the JSQ-P, were assessed using the three-way ANOVA. A path diagram was constructed, and the goodness-of-fit index (GFI), adjusted GFI (AGFI), comparative fit index (CFI), and root mean square error of approximation (RMSEA) were used to assess the degree of fit. SPSS version 26 and AMOS version 26 (IBM Japan Ltd) were used to analyze the data and build the model.
Results
Participant characteristics
A total of 5,244 questionnaires were distributed to kindergartens in four regions (Xining, Gonghe, Xinghai, and Maqin) of Qinghai province in China. A total of 3,827 questionnaires were collected, and the response rate was 72.8% (Table 1). The demographic data of the participants and the family background including the age and education level of the caregivers and the family income are shown in Table 1. Of the 3,827 questionnaires, 180 were excluded due to blank responses, 458 due to missing age, and 76 due to missing gender. A total of 3,113 questionnaires were analyzed.
Demographic Data of the Participants
Sleep habits and duration of sleep of children and parents in Qinghai province
In Qinghai, 91.7% of children slept in the same room as their family, and 76.9% slept with their parents. In all counties of Qinghai province, the median duration of nocturnal sleep was 10.0 hours (interquartile range 9.5–10.5 hours). The median time spent watching TV and gaming time was 60.0 minutes and 0 minutes, respectively.
Comparison of sleep-related daily schedules and the scores of JSQ-P-C in the four counties in Qinghai province
The four counties analyzed in this study had considerably different altitudes. We compared the daily time related to sleep between the four regions (Table 2). The Kruskal–Wallis test showed significant differences but with small effect sizes between the four regions in terms of wake-up time, bedtime, and nocturnal sleep duration.
Comparison of Sleep-Related Daily Schedules and the Scores of JSQ-P-C in the Four Districts in Qinghai Province
JSQ-P-C, Chinese version of the Japanese Sleep Questionnaire for Preschoolers; SD, standard deviation.
Considering the OSA score, there is a regional difference as shown in Table 3. The OSA score of Xinghai and Maqin was higher than that of Xining and Gonghe. This regional tendency was also observed in the scores of morning symptoms and excessive daytime sleepiness.
Comparison of the Nocturnal Sleep Duration and the Scores of Three JSQ-P-C Subscales Among Two Altitudes of Qinghai Province and Japan
OSA, obstructive sleep apnea.
Comparison of the score on subscales related to OSA and sleep problems in high-altitude areas and in Japan
As shown in Table 3, the nocturnal sleep duration is longest in regions >3,000 masl and longer in regions <3,000 masl than in Japan. The subscale score for OSA was not significantly different between <3,000 masl regions and Japan but was higher in >3,000 masl regions than other two regions (Cohen’s d = 0.6). Subscale scores for morning symptoms and excessive daytime sleepiness were highest in regions at >3,000 masl and was higher in <3,000 masl regions than in Japan.
Factors associated with sleep duration and subscale scores in Tibet
It has been reported that sleep-related habits, family income, or parental education level may influence sleep quality (Plancoulaine et al., 2018). Therefore, we conducted further analyses to clarify the factors associated with sleep duration and subscale scores (Table 4).
Factors Associated with Sleep Duration and Subscale Scores in Tibet
Bolded values p < 0.05 is significant.
We conducted a three-way ANOVA to clarify the effects of five fixed factors (county representing altitude, mother’s highest level of education, family income, TV-viewing time, and gaming time) on four dependent variables of children (Table 4). We calculated Pillai’s trace and observed that nocturnal sleep duration was associated with TV-viewing time. Altitudes were strongly associated with scores on all three subscales but not with nocturnal sleep duration.
Figure 1 illustrates a conceptual pathway used to examine the associations of altitude, family income, and gaming time on the scores of OSA, morning symptoms, and excessive daytime sleepiness. We were unable to calculate the GFI and AGFI due to missing values. We developed an ideal structural equation model (CFI = 0.993, RMSEA = 0.028), which showed a significant positive association of altitude (β = 1.75, p < 0.005) and the marginal effect of gaming time (β = 0.03, p < 0.005) with OSA. Morning symptoms scores were influenced by OSA (β = 0.25, p < 0.005). Excessive daytime sleepiness was associated with OSA (β = 0.25, p < 0.005) and morning symptoms (β = 0.20, p < 0.005). Altitude (β = 0.26, p < 0.05) was weakly associated with excessive daytime sleepiness. Family income and gaming time were not associated based on the three subscales. Family income was influenced by maternal education level (β = 0.59, p < 0.005) and altitude (β =−0.30, p < 0.005) but did not show positive effects on the three subscale scores (Fig. 1).
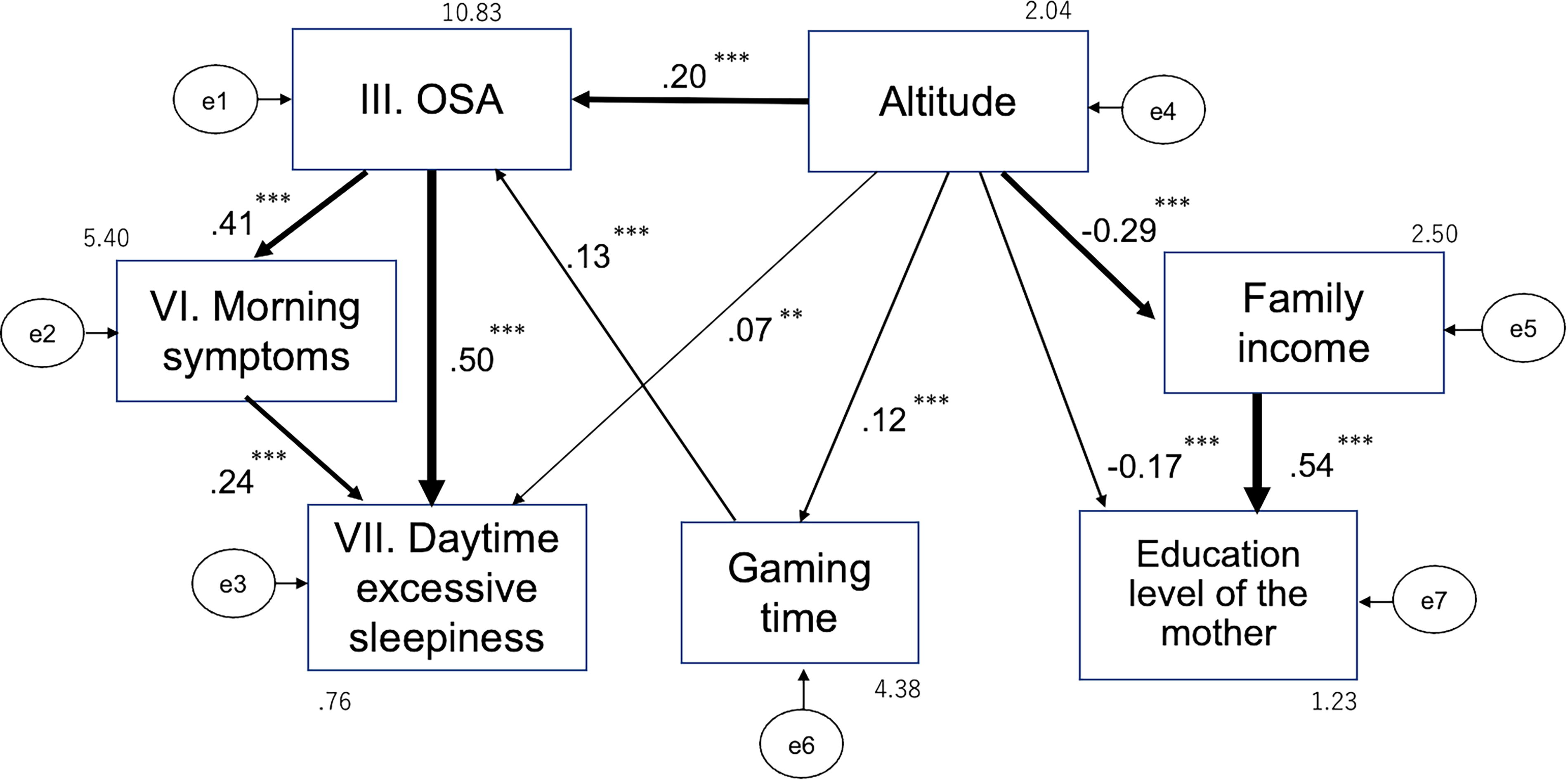
Path model with significant standardized path coefficients. Rectangles indicate the observed variable. **p < 0.005; ***p < 0.001.
Discussion
Sleep habits of children in Qinghai province
In Qinghai Province, 91.7% of children slept in the same room as their families. In other regions of China, 62–88.6% of children slept in the same room as their parents (Chen et al., 2021; Huang et al., 2010). Because children are influenced by traditional concepts and lifestyles of child rearing, caregivers are sufficiently reliable observers of children’s breathing and sleeping conditions during the night to allow accurate assessment of JSQ-P-C scores.
Deterioration of sleep quality in higher altitude areas
Nocturnal sleep duration is longest in >3,000 masl regions and longer in <3,000 masl regions than in Japan. However, the indices of sleep deprivation or sleep quality problems estimated by three subscales are highest in >3,000 masl regions and higher in <3,000 masl regions than in Japan. This may suggest that sleep quality is poorest in children living at regions >3,000 masl and poorer in regions <3,000 masl than in Japan yet longer sleep time. The higher the altitude, the lower the SpO2. SpO2 may decrease further during sleep. Some PSG data have shown that high altitude affects ventilation during sleep; healthy infants (aged ≤18 months) living at high-altitude areas showed higher apnea–hypopnea indices and more pronounced desaturation during respiratory events and SpO2 was less stable (Duenas-Meza, et al. 2015). Moreover, children living in high-altitude areas have greater 3% and 4% oxygen desaturation indices (Hill, et al., 2016) and significantly higher indices of apnea–hypopnea, central apnea–hypopnea, mean end-tidal CO2 level, and desaturation (Burg, et al., 2013). High altitude significantly affects SDB in children, with an increased frequency of obstructive breathing events at bedtime compared with that at lower altitudes, and patients have a significantly higher prevalence and severity of OSA (Hughes et al., 2017). Therefore, at higher altitudes, abnormal breathing during sleep may be prolonged, resulting in higher scores on the three subscales despite longer nocturnal sleep duration.
In this study, subjects residing at altitudes below 3,000 and above 3,000 masl were compared, and the OSA scores were markedly worse in the subjects residing above 3,000 masl. The compensatory ventilatory response to hypoxemia may not function adequately at >3,000 masl. The participants living at 2,000–3,000 masl appeared to have more symptoms than those living closer to sea level. The normative data for sleep respiratory parameters at high altitudes have been reported in healthy preschool healthy children; 3% oxygen desaturation index was 0.1, 8.0, 11.2, and 8.1 at 6–477 masl (Scholle et al., 2011), 1,600 masl (Burgst et al.), 2,560 masl (Ucrós et al. 2015), and 3,700 masl (Hill et al., 2016), respectively. These data suggest that respiratory instability increases with increasing altitude. Therefore, whether there is an inflection point or a linear “dose-dependent” effect of altitude is unclear.
Alternatively, chronic exposure to biomass fuel has been proposed as a cause of SDB (Accinelli et al., 2015). In Tibet, the consumption rates of animal dung, agricultural residues, and electricity were 52.9%, 46.8%, and 0.3%, respectively (Wen and Tu, 2011). Recent data indicated that gas penetration was 91.67%, 52.69%, 52.69%, and 50.44% in Xining, Gonghe, Xinghai, and Maqin, respectively (https://www.china5e.com/news/news-1005213-1.html). Fuels besides gas are mainly electricity. However, as mentioned, electricity use is low, and rural areas still use charcoal stoves. Gonghe is located <3,000 masl and rather than in a rural area, but its OSA score is not high. We do not have accurate data on the type of fuel used; hence, further investigations are required.
In this study, we found that sleep quality may be impaired in children living at extremely high altitudes. It has been previously reported that hypoxia and insomnia at high altitude could cause cognition and mood impairment (Shukitt & Banderet, 1988; Shukitt-Hale et al., 1998). In a comparison of neurocognitive scores between groups of low landers tested at low and high altitudes after acute ascent versus high-altitude-dwelling children chronically exposed to and tested at high altitude, the worst neurocognitive outcomes were found in chronic high-altitude dwellers tested at high altitudes (Rimoldi et al., 2016). Additionally, processing and attention speeds were significantly slower in high-altitude residents than in low-altitude residents (Hill et al., 2014). In addition, anxiety has been reported to correlate with high-altitude sleep (Dong et al., 2013). The prevalence of depression among Tibetans on the Qinghai–Tibet Plateau is higher than that of the general Chinese population (Wang et al., 2019). Reasons for this phenomenon include relatively weak community support due to low population density and lack of access to mental health resources. In addition, exposure to high altitude has been reported to have a detrimental effect on cognitive function (McMorris et al., 2017). Taken together, these findings underscore the need for increased attention to sleep quality in children living at high altitude. To minimize sleep problems in children living at high altitudes, early detection and treatment of SDB or OSA are needed.
Limitations
This study has several limitations. The sample size and response rate differed among the surveyed areas (Table 1). In large cities in the Qinghai province, Tibetans also use Han Chinese as an official language in kindergarten. However, in rural areas, some parents do not use Han Chinese. The questionnaire used in this study was written in Han Chinese and may not have been accessible to parents in Maqin, where Tibetan is mainly spoken. This suggests the possibility of selection bias and may explain the low response rate in Maqin. The highest education level of the parents differed significantly between Maqin and Gonghe/Xinghai but with a small effect size. In addition, family income in Maqin did not differ from that in Gonghe and Xinghai. Therefore, the differences in recovery rate were not considered in further analyses. Second, comparison of Japanese data (Shimizu et al., 2014) is limited by differences in genetics and time intervals between studies. Third, the main outcome measure of this study was the questionnaire data provided by the caregivers, which may have introduced information bias. At present, it remains unclear whether the different mechanisms of altitude adaptation led to differences in sleep. Therefore, a more objective and quantitative assessment may be needed to confirm our findings.
Conclusions
This is the first report to document community-based evidence that high altitude may adversely affect sleep quality in children. More attention to sleep is needed to promote good mental health in Asian children living in extremely high-altitude areas.
Footnotes
Acknowledgment
Authors’ Contributions
Conceptualization, I.M.; Methodology, I.M. and M.T.; Software, P.S.; Validation, Y.O. and P.S.; Formal Analysis, P.S.; Investigation, P.S.; Resources, P.S.; Data Curation, P.S.; Writing—Original Draft Preparation, P.S.; Writing—Review & Editing, I.M. and M.T.; Visualization, P.S.; Supervision, M.T. and Y.O.; Project Administration, I.M.; Funding Ac-quisition, M.T.
Data Availability
Data are not available due to ethical restrictions.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported in part by
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.