
Abstract

The cries for healthcare reform or the reform of reform persist and will grow during the 2016 election year, guaranteeing an ongoing national perseveration about whether, what, and how the provision of healthcare in America will transform. Stakeholders in the complex system of providing and paying for America's healthcare have come to specialize in slicing off and manipulating sections of the system to further their own goals.
Politicians and the media, for their part, feed off simplification and the sensational flame-fanning that it enables. As complex technological, economic, and social forces reshape and transform the U.S. healthcare system, we need to move away from oversimplified and reductionist thinking, and we need to consider change in a holistic and systemic way in order to find possible interventions to improve the system. In other words, thinking more systemically and holistically about our system of healthcare only becomes more important in these times of change. Thinking in this way amounts to innovating by going back to the future, namely by employing older frameworks to see the current world both differently and, we argue, more productively.
Part 1 of this article presented a list of “elixirs in good standing”—commonly cited remedies to the U.S. dilemma of unsustainably high costs and relatively poor performance—and we illustrated several ways in which a systems perspective can provide a different, and perhaps more useful, framework for thinking about important healthcare issues than the reductionist sound-bite approach.
In Part 2, we further develop the systems perspective. We begin with Section 5 of the combined article and revisit the list of elixirs in good standing, and then we make some suggestions about how we might proceed from here.
Section 5: So What? Revisiting the Remedies
In Section 2 of Part 1 of this article, we presented a list of “elixirs in good standing and abundant supply.” Many of them have existed in various forms for a number of years. We list them again here for easy reference:
1. Provider consolidation will be good for you. It will bring the blessings of care coordination, economies of scale, and better care for lower costs. 2. We need to eliminate barriers to access and affordability so that every American can receive access to world-class healthcare at every point in his or her life. If we might provide health services, then we should provide the services. 3. The triple aim is the solution. We need to improve population health, decrease per capita expense, and improve the patient experience. That will solve our problems. 4. Healthcare consumers need skin in the game, and transparency will empower them and improve value dramatically. It will bring the power of the market to bear and drive providers toward efficiency and effectiveness. 5. We need more regulatory oversight of providers and insurers, as well as that of drug and device companies, and the government should use its purchasing power to keep costs in line.
In this second part of our article, we intend to develop further a systems perspective in order to enable us to avoid the pitfalls of experience so ably described by
The way in which we consider the list of elixirs, and complex problems in general, depends on how we frame them—how we organize our thinking about them, and how we simplify and choose information about them. Since, as a practical matter, we can't include all potentially relevant information, we use frames to provide a “theory of the case”—to simplify and make sense. These frames guide the way we filter information and think about important relationships. If we frame complex issues in ways that ignore important systemic relationships, then we risk making incorrect assumptions about the ways in which particular actions or interventions will influence the behavior of the system. For example, if an important goal of the Affordable Care Act (ACA) was to control costs, and if, because of dynamics like those articulated in Figure 2 in Part 1 of this article, the ACA ultimately is found to increase cost, then the question becomes, “How did that happen?” How could— and did— an attempt to decrease cost lead to increased costs?
A systems perspective does not guarantee alignment of intent and outcome, but it does make alignment more likely by encouraging careful thinking about key variables, their interactions, and their causal relationships—broadly rather than narrowly and in theory. The first step toward a systems perspective is framing the issue under consideration in a way that facilitates understanding of the behavior of the system as a whole. Since policy and strategy changes often involve changes in relationships between organizational entities, their descriptions often take the form of diagrams like that in Figure 5, which describes relationships created or influenced by the ACA.
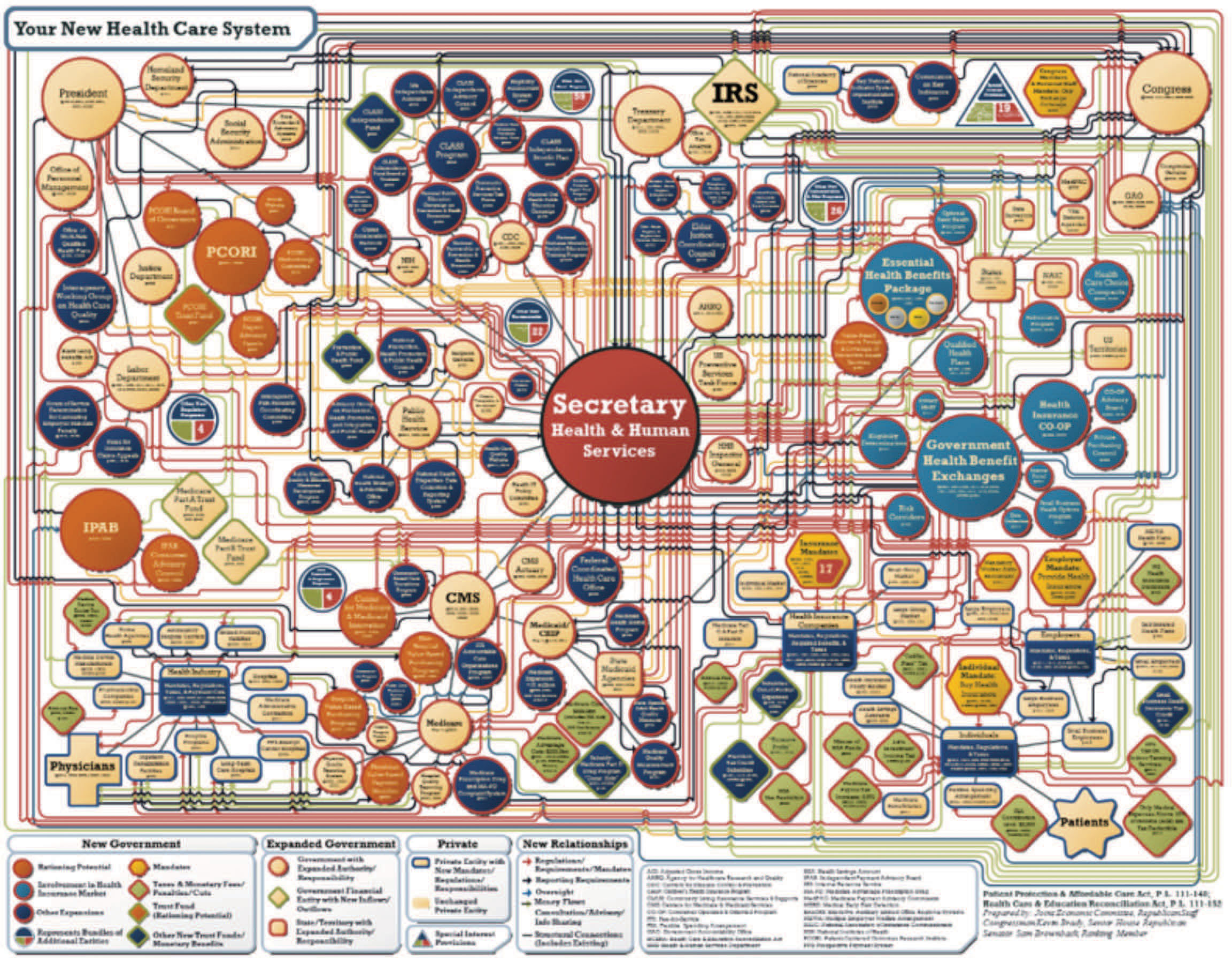
ACA organizational relationships.
While these sorts of diagrams provide useful information about organizational structure and relationships, they provide limited insights about the behavior of the system. They can capture and describe organizational complexity, and they can raise substantive questions (e.g., is the complexity warranted?). They do not, however, provide insights about the causal relationships between goals, interventions, or actions, and expected results.
This use of systems diagrams offers a way to “map the mind” or to make explicit the models that influence our understanding of the system and our actions based on that understanding.

An alternative approach, as illustrated by Figures 2 and 4 in Part 1 of this article, uses a series of simple diagrams that show causal relationships—links between and among variables that influence the main goals of an intervention and, thereby, show a possible causal path to the intended outcome. This use of systems diagrams offers a way to “map the mind” or to make explicit the models that influence our understanding of the system and our actions based on that understanding. For example, the benefits of the triple aim—simultaneously improving population health, decreasing per capita expense, and improving the patient experience—seem intuitively obvious, but we might want to consider how interventions in pursuit of those objectives might lead to unintended consequences.
If we combine elixir #2 (eliminate barriers to access and affordability) with elixir #3 (the triple aim), we might expect, and would hope, that universal access to world-class care (including population health management and provision of the right care at the right time in the right place) would improve population health, lower per capita expense, and improve the patient experience. Figure 6 depicts these wished-for relationships.
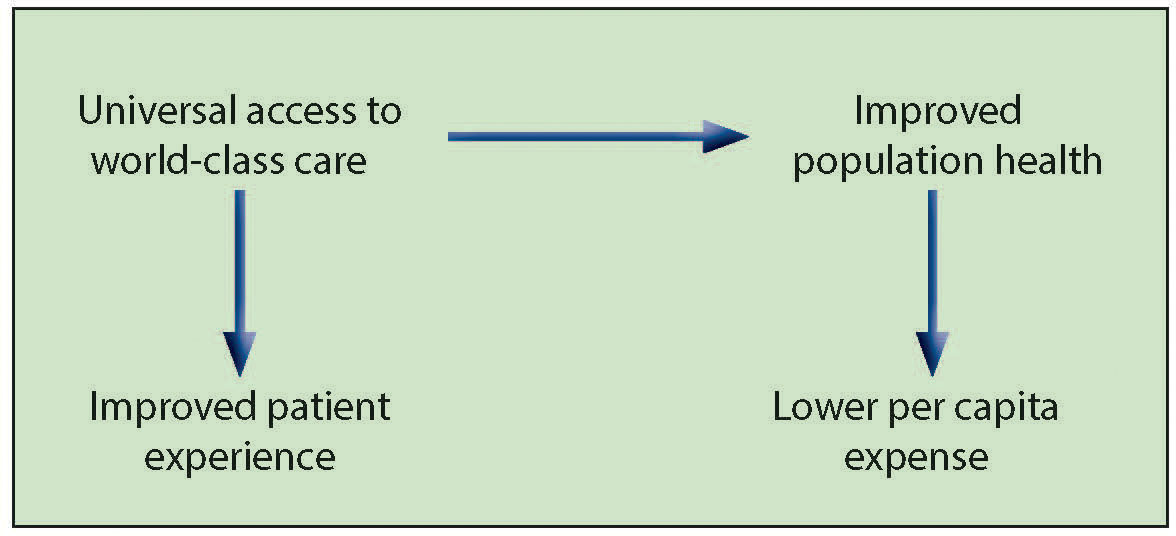
Access improves health and patient experience.
Figure 6 describes an ideal system in which access and appropriate care improve health and lower expense while at the same time improving patient experience. As with the other diagrams we've presented, this simple mapping articulates key assumptions, identifies important variables, and shows a hypothetical set of relationships among variables. The transparency inherent in this approach enhances our ability to question the conceptual structure of the model and to hold it up against the available empirical evidence.
For example, this model implicitly assumes no trade-off between improved patient experience and lower expense. In addition, it appears to assume that providers of care and suppliers of devices and pharmaceuticals focus their health improvement efforts in a way that lowers expense, and that population health is driven more strongly by access to care than it is by the myriad social and economic factors that influence population health for both better and worse. Figure 7 provides an alternative view.
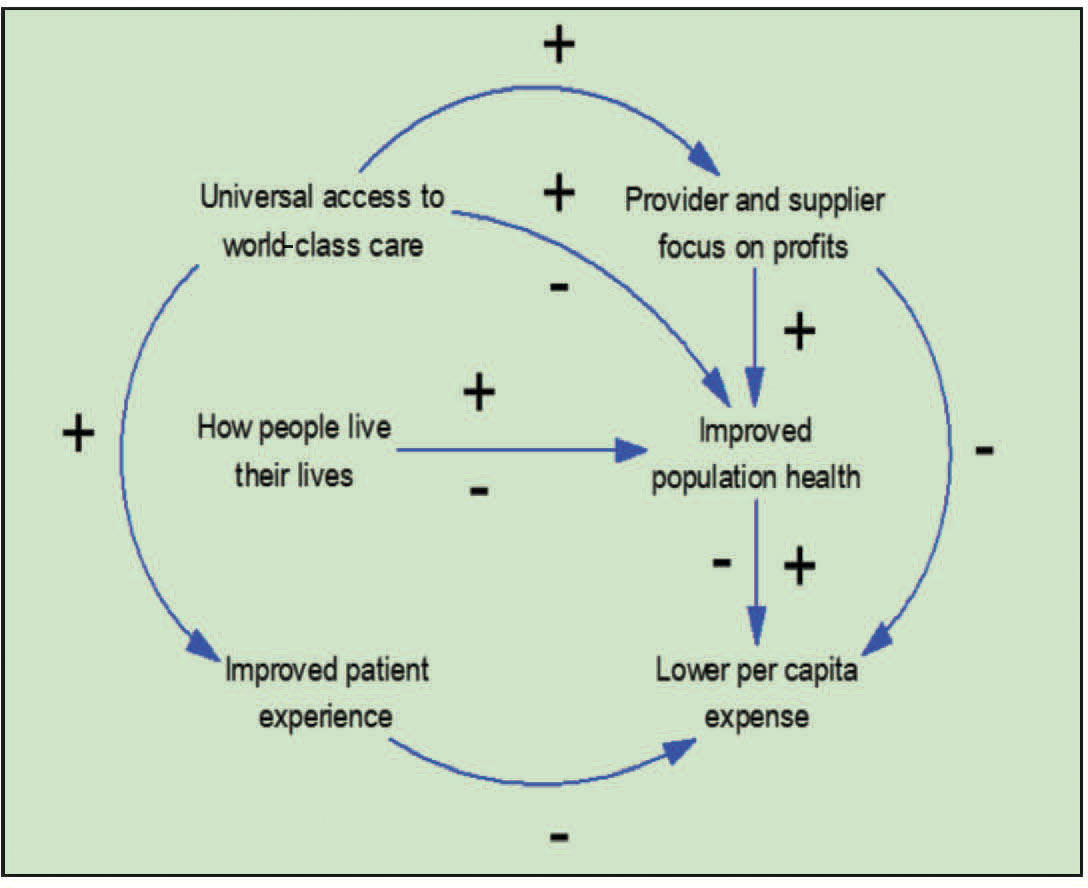
An alternative view of access and the triple aim objectives.
In this representation, broader access to care has the potential to improve population health, but it also has the potential to cause negative impacts on population health because of iatrogenic effects such as those described
Additionally, universal access to world-class care attracts providers and suppliers whose entrepreneurial focus encourages them to develop innovative products and services that can improve population health but that also maximize profits and drive up costs. Caregivers’ efforts to improve the patient experience can take the form of opulent facilities and amenities that increase the cost of care and frustrate efforts to lower per capita expense. Furthermore, improved population health does not necessarily translate into lower per capita expense.
In this model, costs may rise without a commensurate improvement in population health if providers and suppliers prove more successful at generating profits than at improving health. If access to care is increased by subsidies (e.g., insurance exchange subsidies, Medicaid expansion, etc.), then the subsidies may boost provider/supplier profitability more than population health. Furthermore, if subsidies are provided to select groups of people, then those without subsidies may be disadvantaged because they have greater financial exposure without improved health outcomes. 4
This model is not intended as an argument against expanded access or the triple aim objectives, but rather as a depiction of how competing interests of various groups of stakeholders could sidetrack well-intended efforts to attain laudable goals. The key outcomes—population health, per capita expense, and patient experience—come under the sway of various forces and not necessarily in a simple unidirectional way that supports our hopes and expectations. The behaviors of stakeholder groups may evolve in complex ways, and different stakeholders may have very different viewpoints and objectives that shape their behaviors. The explication of those dynamics in a systems model can increase understanding and inform action in pursuit of important social goals such as the triple aim.
For instance, since out-of-pocket payments are a small and decreasing share of total healthcare spending, many have argued that healthcare consumers need “skin in the game” (elixir #4), and that transparency will empower them and improve value. In Figure 8, increased financial exposure focuses the mind of the consumer of care, and increased transparency provides the consumer with better information about provider/supplier prices, outcomes, and customer satisfaction. This results in improved decision making about care and has a moderating effect on per capita healthcare expense.
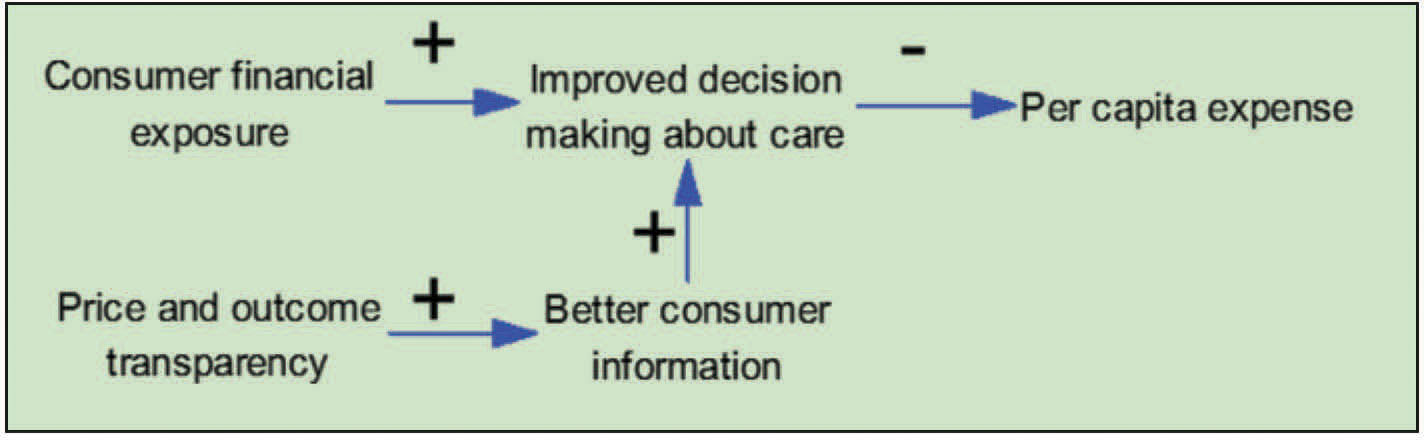
Skin in the game.
The relationships portrayed in Figure 8 clearly do not apply to many high-cost situations such as emergencies and complex care processes when consumer discretion is limited or even absent. Figure 8 also assumes that the combination of increased consumer financial exposure and increased transparency will result in improved decision making. Figure 9 provides an alternative viewpoint.

Skin in the game revisited.
In this representation, some forms of increased consumer financial exposure such as high deductibles and copays may increase the risk of financial distress (“financial toxicity”), which causes people to delay or forgo timely care. The manner in which population-wide financial exposure influences consumer decisions about obtaining care may lead to per capita expense ultimately rising if care is not provided at the right time in the right setting. For example, patients with chronic diseases may wait until becoming very sick to seek medical attention and then seek care in the emergency room. In addition, limited decision-making capacity due to limited medical literacy or inability to process complicated information may mitigate—and perhaps all but negate—the impact of increased transparency. This fairly simple model suggests reconsideration of, and perhaps reemphasis on, a set of interacting factors such as insurance plan design, the role of consumer education, and the use of care navigators.
Figure 9 also begs the question of how these dynamics would evolve over time. For instance, if consumer financial exposure increases much more quickly than consumer decision-making capacity, the result would be a disempowered and vulnerable consumer and, perhaps, an increasingly unhealthy one. Effective framing of the issue, simulation of behavior over time, and examination of the effects of delays and cumulative effects help expose key policy or strategy issues and identify potential unintended consequences.
The absence of a commonly shared systemic view of the U.S. healthcare system, the seemingly intractable combination of unsustainably high costs and relatively poor performance, and the complexity of stakeholder behaviors stimulate calls for centralized control in the form of increased governmental and regulatory action (elixir #5). An important part of Medicare's response to these calls is a shift from “pay for volume” toward a “pay for value” approach, which makes provider payments dependent upon performance related to process of care, outcomes, patient satisfaction, and efficiency. The shift toward pay for value by Medicare warrants particular attention because Medicare is about 14% of the federal budget, and Medicare payments represent close to half of the revenue of a typical hospital. Also, since private payors generally follow Medicare's lead, providers expect that the pay for value paradigm will eventually become the predominant payment model.
By the Numbers
14% of the U.S. federal budget goes to Medicare
50% of a typical hospital's revenue comes from Medicare payments

In Figure 10, pay for value focuses providers on improving care processes, quality, and appropriateness, and results in a positive impact on outcomes. Since better outcomes are incentivized (and since worse outcomes are penalized in some versions of pay for value), value increases. Figure 10, however, assumes a unidirectional beneficial effect from the pay for value approach, and it ignores stakeholder behaviors that interfere with that effect. Figure 11 provides an alternative model.
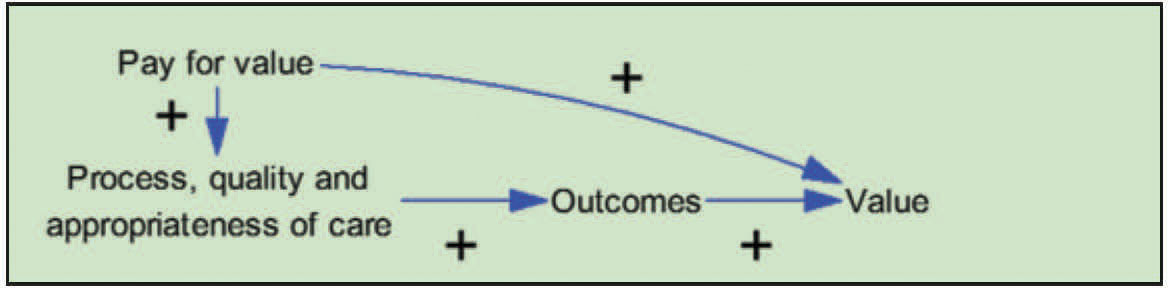
Pay for value focuses providers on value.

Stakeholder response influences the effects of pay for value (PFV).
In Figure 11, pay for value has a potential side effect of encouraging providers to increase efforts at regulatory capture. Provider involvement in the regulatory process may improve pay for value efforts in numerous ways, but it may also be used to shape pay for value efforts in a way that benefits providers in general, and politically powerful providers in particular.
The model in Figure 11 assumes that pay for value will indeed focus provider attention on the improvement of care processes, quality, and appropriateness. However, it also provides for the possibility that pay for value efforts will encourage provider gaming through changes in coding practices or patient selection. This type of gaming, by influencing outcome measurement, might overstate the outcome improvement that is actually achieved, and it might favor more sophisticated organizations that have the information infrastructure and resources needed to adapt to regulatory requirements. In addition, Figure 11 suggests that organizations with the best outcome performance may use their performance to build market share. This may, in turn, have the beneficial effect of driving more market share to high-performing organizations. It might also have the unintended consequence of increasing market concentration and pricing power. In short, while most healthcare stakeholder groups would agree that pay for value is a beneficial concept, particularly when implemented by Medicare in a methodologically rigorous way, the dynamics described in Figure 11 suggest that complex stakeholder dynamics could produce unintended consequences that are worthy of consideration as pay for value efforts proceed.
Figure 11 and the other models that we've presented show how we can use simple systems diagrams to describe and test the way in which various interventions such as elixirs #1–5 might play out in the complex U.S. healthcare system. In debates about policy and strategy issues, the implicit system often exists differently and unarticulated within the mind of the various beholders. Consequently, those beholders do not share or attempt to achieve an understanding about system boundaries, relationships, and dynamics. This lack of shared understanding precipitates adversarial arguments rather than the thoughtful consideration from a holistic viewpoint. By using systems diagrams to describe important cause and effect relationships and create an explicit theory of systemic behavior, we can build a shared understanding of systemic relationships that can recognize numerous stakeholder viewpoints and inform decision making.
As healthcare is transformed by a myriad of social, economic, and technological forces, the use of this approach in strategy and policy development can:
• Encourage a broad, whole-system viewpoint that provides context for consideration of more narrow issues; • Provide an explicit graphic representation of the system under consideration, so that the concept of the system can be viewed, tested, refined, and communicated; • Help stakeholders understand the perspectives of other stakeholders; • Describe potential feedback loops, trade-offs, and unintended consequences.
These models help us comprehend complexity by simplifying reality, but they also require that we omit information. This trade-off requires mindfulness about the construction of our models, that is, that we think carefully about what a model omits and that we test our models with diverse groups of stakeholders in order to determine what a model misses and the importance of those misses.
Section 6: A Whole-System View of Cost
We offer one more model for consideration—one that provides a whole-system viewpoint of cost drivers in the U.S. healthcare system. Suppose we conceptualized America's healthcare system in terms of consumer behavior, provider and supplier behavior, and financial stakeholders. The model presents consumers as the recipients of services and products, providers and suppliers as those who provide the services and products that are consumed, and financial stakeholders as those who pay for the products and services consumed.
Obviously, such large categories or buckets lump stakeholders with something in common, but also with much that differentiates them. However, this basic grouping can help to provide an overview of more than 17% of America's economy, that is, its vast and sprawling system of healthcare. Figure 12, therefore, presents one possible way, albeit a simplified one, of thinking about the relationships among consumers, providers and suppliers, and financial stakeholders. 5
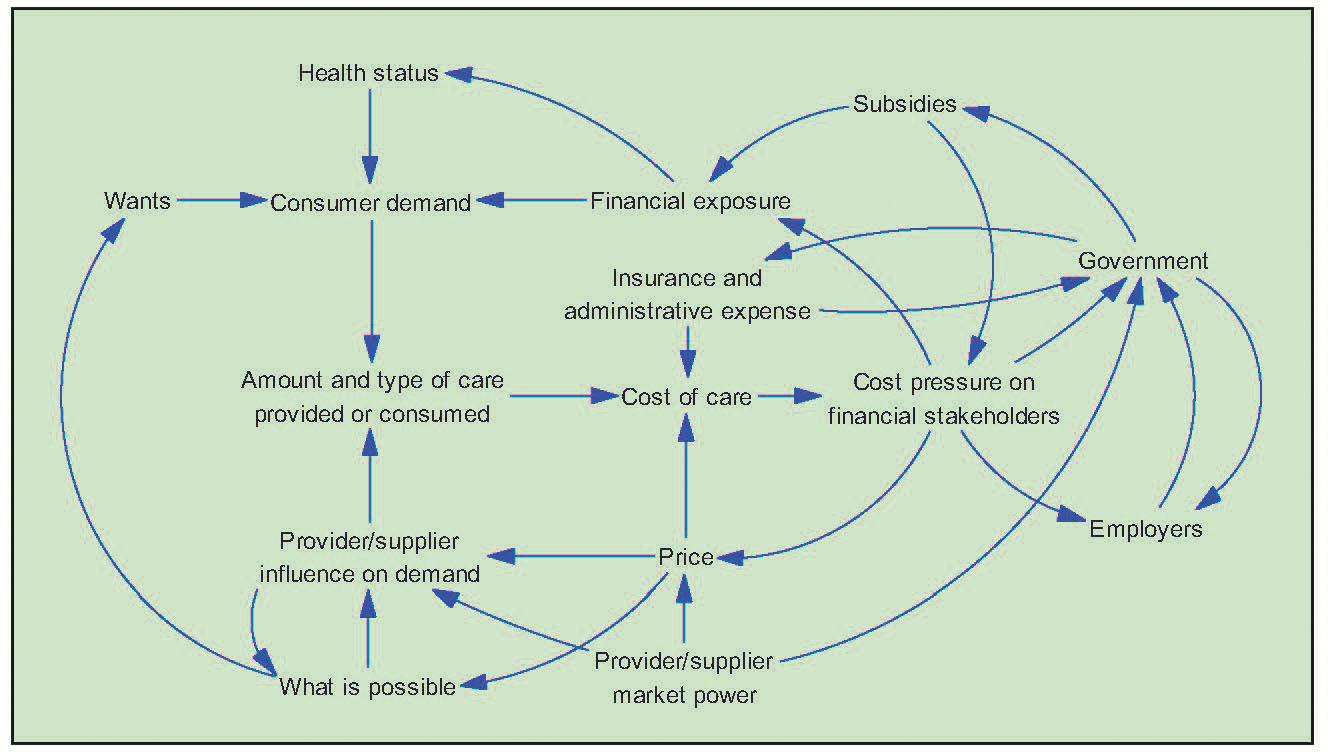
Consumers, providers and suppliers, and financial stakeholders.
In Figure 12, consumer demand interacts with influence by providers and suppliers to drive actual consumption of services and products. Health status (which influences which services and products are needed), wants (which influence the services and products that the consumer would like to receive), and financial exposure (the amount of out-of-pocket cost that the consumer will bear) combine to drive consumer demand. Providers and suppliers influence demand by continually expanding what is possible, by using market power to influence consumption, and by influencing government to cover services and products, provide subsidies, and so on. Employers and the government work to shift the financial burden to each other and to consumers of care. Government influences insurance and administrative expense through coverage mandates and numerous other forms of regulations; insurers, in turn, influence government policies about subsidies and many other regulatory matters.
This still relatively simple model suggests several tried and true ways for financial stakeholders to reduce cost pressure: by increasing consumer financial exposure (e.g., increased premiums, co-pays, and deductibles), by putting downward pressure on prices (e.g., price negotiations, government price controls), and by changing how the federal government pays for drugs. It also suggests that costs may be driven by several dynamics over which financial stakeholders have limited control:
• Innovation and the ongoing expansion of what is possible may result in better and less expensive care, but it may also produce expensive diagnostic and treatment technologies, which mainly serve to increase supplier and provider profits and which may not actually provide more effective or less expensive care. • Providers and suppliers may drive demand for expensive (and profitable) new products and technologies by influencing consumer wants (e.g., direct to consumer advertising). • Provider and supplier market power may influence prices and government policies about subsidies. It may also shape demand in a way that maximizes profitability, but does not necessarily benefit the consumer of care. • Health status, as we've discussed in previous examples, may be influenced strongly by how people live their lives.
The connections in this simple model suggest that the relief of cost pressure on financial stakeholders may require a set of coordinated and systemic interventions that influence not only consumer financial exposure and price, but also provider and supplier market power, consumer wants and knowledge, health status drivers, and perhaps the trajectory of technological development. This model and others like it can provide a straw-man concept of a system that can be challenged, modified, and refined. It begs the question of what variables and relationships should be added or omitted.
The process of refining a conceptual model like this one can lead to bringing it to life with a computer simulation populated with data. Such a simulation enables playing out complex systemic dynamics over time in order to evaluate the potential effects of various interventions into America's healthcare system. The process of developing a simulation requires the articulation of an explicit theory of the system and a discipline of intellectual honesty and transparency. Simulation development can serve to build shared understanding across stakeholder groups through a shared process of creating and validating the systems diagrams, selecting data, and, finally, examining the results of the simulation.
Section 7: Remedies and More Remedies—How to Think About What to Do
Changing how we see healthcare in America alters how we think about it and therefore what we would do to improve it. How might a systems thinking perspective change our consideration of the five elixirs we've been examining?
Assumed causality: Consolidation will improve coordination of care and provide economies of scale.
Systems perspective: Consolidation may also increase pricing power and drive up costs.
Implication: We need to consider the trade-offs between consolidation, care coordination, economies of scale, and increased prices.
Assumed causality: Removal of barriers and affordability, population health management, and provision of the right care at the right time in the right place will put downward pressure on per capita expense.
Systems perspective: Provider and supplier stakeholders may provide excellent care and products that also drive up costs.
Implication: We need to consider the ways in which increased access could have the most beneficial impacts on health status and costs.
Assumed causality: Improved population health will put downward pressure on per capita expense, and the patient experience will be improved without driving up per capita expense.
Systems perspective: Provider and supplier stakeholders may pursue the goals of improving population health and improving the patient experience in a way that drives up costs and provider/supplier profits.
Implication: We need to consider the ways in which competing stakeholder interests could interfere with the pursuit of the triple aim in order to anticipate and address realpolitik … and “economics-real” better.
Assumed causality: Increased out-of-pocket financial responsibility combined with more information transparency will result in more informed healthcare consumers who will then bring market forces to bear in making value-based purchasing decisions.
Systems perspective: Increased financial exposure may also cause individuals to delay or forgo necessary care, which might drive up expense because patients might be sicker and/or treated in more expensive settings such as the ER or as a hospital inpatient. In addition, an inability of many healthcare consumers to process complex decisions might mitigate some or all of the potential benefits of increased transparency.
Implication: We need to consider the ways in which increased financial exposure influences consumer behavior, and we need a better understanding of the ways in which healthcare consumers use (or don't use) information about price and quality.
Assumed causality: Governmental commitment to the good of the whole combined with its impartial competency will improve the operation of America's healthcare system.
Systems perspective: Regulatory oversight is not intrinsically good or bad, partial or impartial. Its impact needs to be understood from a systems perspective.
Implication: We need to consider the ways in which regulatory oversight influences the behavior of important stakeholder groups (regulators and regulated alike). In addition, we should evaluate separately the impact of the various governmental roles (e.g., buyer of products and services, provider of social welfare services, regulator of safety and efficacy of drugs and devices, and monitor of competitive behavior).
Section 8: Things to Do and a Caution or Two Before We Part Company
Perhaps the greatest choice at hand amounts to this analogy: Will the various stakeholders in American healthcare continue to argue about their relative seating in the Roman Senate as the Visigoths dismantle yet another aqueduct in their tightening siege of Rome? The Roman Senate was a grand body overflowing with the prominent and the wealthy. It also had long before lost a collective or shared sense of the whole. Reforming healthcare in America will require many a prominent and wealthy stakeholder—and a number who are neither—to step back and look at the whole. A systems approach can help those willing to do so. Implication: think systems … and don't stop.
We offer Table 1 as an example of how a systems perspective might be applied to some familiar healthcare industry sound bites. The table includes a familiar sound bite, a reasonable and legitimate rationale associated with the sound bite, a brief note about how a systems perspective might inform our consideration of the issue at hand, and a bit of “wisdom” from
Sound bites reconsidered
Where else might this approach lead? If various stakeholders in the American healthcare system were to take a systems approach, then how might they act? First, revisit the discussion of elixir #5 above. Second, be the change that you want to create.
Other stakeholders in America's healthcare system face a similar set of choices. Each will decide whether to scramble for better seating in an unsustainably underperforming system or to step back, think systemically, and consider the longer term. Stepping back would enable both different cognitive work, that is, considering how to recast the system and their role in it, and different relational work, that is, how to recast working relationships among stakeholders.
The recasting of current working relationships bears highlighting. In Part 1 of this article, we discussed how simplification leads to animated finger pointing and then to scapegoating. A reference to the Roman Senate during its waning days opened this section. Personalizing and demonizing drives out systemic thinking just as non-systemic thinking facilitates such personalization and demonization. The cognitive approach and the emotional experience foster and reinforce one another. Each stakeholder therefore chooses to further current reality or to change it, beginning with whether to explore examining the system as a system with any stakeholder willing to do so.
More specifically, stakeholders wishing to turn down the heat and to pursue thinking in a manner suggested here might have groups of stakeholders create simple systems diagrams, and then share them across groups. Stakeholders could use information from this process to test strategy and policy interventions. After stakeholders have created and discussed their systems diagrams, then they might explore the following questions:
• How will the relationships in the diagrams play out over time? • How much do we know about the relationships in the diagram? Are they linear? • What are the incentives of the various stakeholder groups, and how are they likely to respond to particular interventions? • What are the potential unintended consequences? • What are the most difficult trade-offs? • What system boundaries are unclear and may require particularly close monitoring and refinement? • How will we know how well a system redesign works? • If potential interventions do not work out as intended, how will the systemic burden be shifted? How will goals be shifted? • If potential interventions do not work out as intended, what types of emotional and/or personal attribution would we expect? What behaviors would likely arise over time?
Next, stakeholders might create simple computer simulations that allow the playing out of systemic dynamics over time and thereby better anticipate paths to a variety of “plausible futures.” Such simulation or machine-aided learning would go far beyond the possibilities of traditional scenario planning and could well aid collaborative system design and implementation.
Conclusion
American healthcare simply costs too much for what it delivers, not necessarily in any particular case but in its entirety. That reality can easily lead to frustration, even rage, and to associated name calling, finger pointing, and silver-bullet hunting. Systems thinking would offer that America's system of healthcare, like any other system, produces what it is designed to produce. Hence, to change American healthcare, change the system, and to change the system, first think system and then map the system. 6 Let that thinking and mapping guide efforts to alter what the system yields. Let that thinking and mapping also guide and inform consideration and discussion of American healthcare. Let it also guide the countless and ongoing refinements that will prove necessary.
Footnotes
Author Disclosure Statement
No financial conflicts of interest exist.