
Abstract
Anthrax response plans, exercises, and assessments over the past decade have focused almost exclusively on the first 48 hours of the public health response following a jurisdiction-wide exposure and provision of an initial 10-day supply of antibiotics from the Strategic National Stockpile (SNS). But mass dispensing of the subsequent 50-day course of antibiotics and administration of the 3-dose vaccine series have received considerably less attention, although these follow-up activities may prove even more complex. In 2014, the Philadelphia Department of Public Health (PDPH) made its first foray into this next frontier of mass prophylaxis planning by: (1) researching patient safety and adherence considerations relevant to the antibiotics in the SNS; (2) designing a model for a second-visit antibiotic and vaccine point of dispensing (POD), including development of an enhanced screening protocol that assumes a higher level of medical responsibility; and (3) field testing this model during a real seasonal influenza vaccination clinic to assess throughput and accuracy and to evaluate the resources needed to operationalize this model. While the observations and data presented here provide some framework for local long-term mass prophylaxis planning efforts, many areas remain undefined, including the distribution of responsibilities among the public health and healthcare communities to ensure patient safety. In addition to presenting findings, the larger intent of this article is to initiate a dialogue with other stakeholders at the local, state, and federal levels to advance long-term mass prophylaxis planning.
Anthrax response plans, exercises, and assessments over the past decade have focused almost exclusively on the first 48 hours of the public health response. But mass dispensing of the subsequent 50-day course of antibiotics and administration of the 3-dose vaccine series have received considerably less attention, although these follow-up activities may prove even more complex. The Philadelphia Department of Public Health researched patient safety and adherence considerations relevant to the antibiotics in the SNS and designed a model for a second-visit antibiotic and vaccine point of dispensing (POD). They field tested this model during a real seasonal influenza vaccination clinic to assess throughput and accuracy and to evaluate the resources needed to operationalize this model.
S
In 2014, the Philadelphia Department of Public Health (PDPH) made its first foray into this next frontier of mass prophylaxis planning by: (1) researching patient safety and adherence considerations relevant to the antibiotics in the SNS that would likely be used as anthrax postexposure prophylaxis; (2) designing a model for follow-up antibiotic and vaccine dispensing that addresses these considerations, including development of an enhanced screening protocol that assumes a higher level of medical responsibility to decrease adverse events and ensure patient compliance; and (3) field testing this model during a real seasonal influenza vaccination clinic to assess throughput and accuracy and to evaluate the resources needed to effectively operationalize such a model. This article describes the thinking behind the expanded screening model, outlines the exercise methods and findings, and proposes directions for future planning, as there is still much work to be done.
Inhalational anthrax has a 90% mortality rate if left untreated, and the incubation of the disease may be very short, typically ranging from 1 to 7 days, although a prolonged incubation period of up to 60 days is possible.3,4 The current recommendation for postexposure prophylaxis is a 60-day course of antibiotics and 3 doses of anthrax vaccine to produce long-term immunity. 3 Anthrax spores can remain viable in the lungs up to 100 days following exposure; thus, it is necessary to adhere to the prescribed antibiotic regimen until the completion of 3 doses of anthrax vaccine, plus an additional 2-week period after the final dose, to mount sufficient immunity. 3
The high mortality rate of inhalational anthrax, coupled with a potentially very short incubation period, will demand a swift and decisive response from public health agencies. The urgency of the public health response will dramatically alter the traditional patient–clinical provider model. In order to expedite the provision of hundreds, thousands, or even millions of antibiotic regimens to all potentially exposed people prior to disease onset, public health agencies must implement an emergency medication dispensing strategy that significantly truncates the screening process to just a few essential questions. In effect, assessment for the disease of interest, patient histories, and physical examinations will be greatly curtailed or omitted completely during an emergency medication screening process under emergency authorizations. Consequently, some conditions and/or potential complications may go unaddressed during the initial screening process. Specifically, current medical conditions, concomitant medications that may interact with doxycycline or ciprofloxacin (the primary and secondary prophylactic drugs for anthrax in the SNS), and dosing considerations related to conditions such as renal insufficiency may not be addressed during the initial screening encounter. These issues may result in a variety of negative patient outcomes with varying levels of risk and severity when prolonged antibiotic therapy is indicated.
As evidenced by historical postexposure anthrax responses and through studies of antibiotic compliance, adverse events from antibiotic medications are common and adherence is frequently poor.5-7 Following the anthrax letter attacks of 2001, 10,000 people were recommended to receive 60-day courses of doxycycline, ciprofloxacin, or amoxicillin. According to a retrospective cohort questionnaire, 3,032 of the 5,343 respondents who took at least 1 dose of antimicrobial prophylaxis (57%) reported adverse events. 5 Among those who experienced an adverse event, 32% reported diarrhea or stomach pain, 27% reported nausea or vomiting, 25% reported headache, and 22% reported dizziness. 5 The most common reasons for discontinuing prophylaxis (n=2,631) were the onset of adverse events (43%), the perceived low risk of developing anthrax disease (25%), and the fear of long-term side effects (7%). 5 Adherence among postal workers who received long-term prophylaxis regimens of doxycycline, ciprofloxacin, or amoxicillin ranged from 40% full adherence, to 42% spotty adherence, to 18% discontinuing prophylaxis. 6 Other potential adverse events associated with these antibiotics include pseudomembranous colitis, vaginal candidiasis, photosensitivity/skin erythema, blood abnormalities, theoretical cartilage damage/arthropathy, lower seizure threshold, central nervous system events, myesthenic exacerbation, liver enzyme elevation, serum creatinine elevation, and permanent tooth discoloration (children under the age of 8 and pregnant women in the last half of pregnancy).8-10
Taking these antibiotics for an extended period also poses increased health risks to some groups. Both doxycycline and ciprofloxacin (pregnancy classes D and C, respectively) pose potential risks to unborn babies and children (eg, enamel hypoplasia and tendon damage).8,9 Amoxicillin is generally considered a safer alternative for these groups and is routinely used for both pediatric and pregnant populations (pregnancy class B).3,10 Older people and immunocompromised individuals are at greater risk for superinfection, including potentially severe diseases like pseudomembranous colitis associated with Clostridium difficile and other bacterial or fungal organisms. 11 In addition, individuals with kidney disease may be at risk while on long-term prophylactic regimens because renal elimination may be impaired.9,10 Thus, patients with renal disease would require monitoring and potential antibiotic dose adjustments to prevent toxicity. Perhaps most significantly, many commonly prescribed medications have warnings associated with concomitant use with the antibiotics for anthrax prophylaxis contained in the SNS. For doxycycline, contraindicated medications include anticoagulants, oral contraceptives, phenytoin, carbamazepine, and barbiturates; for ciprofloxacin they include anticoagulants, theophylline, phenytoin, glyburide, and cyclosporine.8,9
This list of contraindicated medications illustrates the potential dangers of an abbreviated initial screening process that may not include questions about current medication usage. Anticoagulants, for example, are widely used and can potentially interact with both the primary and secondary drugs in the SNS. Approximately 30 million prescriptions for warfarin were written in 2004, and 18.1% of people aged 65 and older were prescribed at least 1 anticoagulant from 2007 to 2010.12,13 Notably, the package inserts for both doxycycline and ciprofloxacin contain warnings against concomitant use with anticoagulants because this combination can produce an enhanced anticlotting effect, which may increase the risk for bleeding events.8,9,14-16 Similarly, theophylline, a drug used to treat many common respiratory conditions including asthma, is contraindicated for use with ciprofloxacin as concomitant use with quinolones can lead to elevated blood levels of theophylline, which can cause seizures and cardiac arrhythmias.8,17 While illustrative rather than exhaustive, these few examples demonstrate some of the potential hazards of an abbreviated initial screening process that may result in simultaneous use of contraindicated medications in some patients. Additional modeling to project types and rates of adverse events that could present during a large-scale, long-term mass prophylaxis response using antibiotics from the stockpile would be of great value to both preparedness planners and the healthcare community.
Three courses of anthrax vaccine, given at weeks 0, 2, and 4 postexposure, are also indicated as part of the current CDC recommended postexposure prophylaxis regimen. 3 Although there is little published data about anthrax vaccine adverse events, a report published by the General Accounting Office indicated that 85% of US military personnel who received anthrax vaccine or vaccine components had 1 or more adverse reactions. 18 As such, screening for previous reactions to anthrax vaccines and monitoring for vaccine-related adverse events are other considerations for inclusion as part of the screening process.
Many health departments plan to use a combination of emergency dispensing strategies to provide the first 10-day course of antibiotics. These include public points of dispensing (PODs), first responder and prioritized population dispensing sites, select clinical provider venues (eg, health centers, pharmacies, hospitals), and closed PODs at government agencies and businesses, which often lack their own on-site medical staff. All of these rapid dispensing options can compromise patient safety by using an emergency screening process that may inadvertently miss some potentially injurious factors. Several of these options may further increase adverse events by dispensing only 1 medication to all or relying on nonmedical staff to conduct screening and dispensing, as is the case in many closed PODs and which has been shown to decrease dispensing accuracy. 19 An additional problem affecting patient safety is that paper-based records may be used during the urgent response, thus making patient tracking and individual follow-up burdensome and potentially even unmanageable in a large-scale response. One final challenge is that public health agencies may expect that the healthcare community will assume responsibility for addressing complications and ensuring compliance for prolonged courses of antibiotics among large populations, though patient surge and demand for health resources following a bioterror event would likely overwhelm existing capacity. 20 Roles, responsibilities, and processes for ensuring patient safety through systematic tracking protocols and follow-up care have not been clearly delineated and remain nebulous.
While a great deal of planning has centered on providing the first 10-day course of postexposure antibiotics, less consideration has been given to the complexities associated with the follow-up visits that will need to occur to provide additional antibiotics and anthrax vaccine. Assuming that the public health response begins by putting all exposed people on a 10-day regimen of antibiotics within the first 48 hours following the detection of an event, there will be a 5- to 7-day window to provide the additional 50-day supply before the initial 10-day regimen is depleted.
Given this expanded timeframe, more thorough screening protocols to ensure patient safety and compliance can and should be instituted during the second visit. To increase understanding of what this process might entail, PDPH developed an emergency medication screening protocol for subsequent visits and conducted a dual-model POD clinic to simulate and evaluate the provision of the follow-up 50-day course of antibiotics and the first dose of anthrax vaccine. The main objective was to estimate the level of increased medical responsibility of the local health department for completion of postexposure prophylaxis given a longer timeframe (5-7 days) by: (1) developing and testing an expanded disease and antibiotic screening process designed to identify breakthrough cases, ensure medication compliance, minimize adverse events, and dispense complete antibiotic regimens; (2) incorporating the second component of a dual-model POD by including screening for and provision of a first dose of injectable vaccine; (3) using an electronic patient record system in the field for tracking and long-term follow-up for both interventions; and (4) testing the staff and logistical requirements needed to complete the dual medication model in the desired timeframe.
The clinic presented an opportunity to test the expanded antibiotic screening process to obtain data on both dual-model clinic throughput and medication screening accuracy. Additionally, a new staffing model, new staff functions, a new screening algorithm, and new electronic data capture methods were evaluated as part of this activity. To our knowledge, no data have previously been published regarding how long this extended screening process might take, which questions and how many questions should be included during follow-up screening to reduce complications, and how accurately medication determinations are made during an expanded screening process. With respect to both the timeframe and resources needed to successfully execute an emergency long-term mass prophylaxis response at the local level, there are many unknown variables. Here we provide a framework, including presentation of initial baseline data, that can be used by other public health agencies to estimate their own capacity, inform their own long-term mass prophylaxis plans, and further evaluate the realistic distribution of responsibilities between public health agencies and the healthcare community in ensuring patient safety and administering follow-up care during such a response.
Methods
Dual-Model Antibiotic and Vaccination Clinic
In January 2014, PDPH conducted a dual-model (pills and vaccine) dispensing clinic at an all-boys Jewish boarding school, where the maximum expected population for vaccination was 200 people over 3 hours. Clinic encounters consisted of a 2-station process: antibiotic medication screening and dispensing followed by screening for and administration of vaccine. The clinic was designed to simulate the second patient visit following an anthrax exposure, when people would be provided with a 50-day additional course of antibiotics and the first of dose of anthrax vaccine. Kosher candy was provided as a proxy for additional antibiotics, and seasonal influenza vaccine was administered by injection to simulate administration of anthrax vaccine. Doxycycline was presumed to be the primary antibiotic dispensed in the initial mass medication response, with some populations receiving ciprofloxacin. The clinic model assumed that 50-day regimens of a third and safer antibiotic (amoxicillin) were effective and available in large amounts from the federal stockpile. It was assumed that patient data would have been collected on paper forms during the initial POD visit but would be captured electronically at the second visit to the antibiotic dispensing/vaccination clinic.
Clinic Staff, School Population, and Script Demographics
Students at the school were all males between the ages of 13 and 21. Clinic staff included health department employees and 2 Medical Reserve Corps (MRC) volunteers who served as vaccinators. A patient script key was crafted to reflect an accurate cross-section of the expected population, based on disease prevalence data, prescription medication data, medication-related adverse event data, and county census demographic data.5,19,21-27 The script key also documented the correct 50-day medication assignment for the patient based on a medication screening algorithm. One hundred unique patient scripts were developed from the script key, which documented patient age, weight, initial antibiotic provided, date patient began using antibiotic, antibiotic compliance information, adverse event and disease symptoms, patient medical conditions, and current medications.
Expanded Antibiotic Screening Protocol
The expanded screening protocol was developed to ensure that any individuals indicated for long-term prophylaxis take the safest antibiotic for the duration of their regimen. To streamline this expanded screening process, PDPH used a custom-designed electronic database that prompted screeners to complete 5 main steps: (1) capturing patient contact information; (2) screening for symptoms of the disease; (3) assessing current medication regimen for adherence, side effects, and contraindications and assigning a safer antibiotic if indicated; (4) ensuring the correct dose for pediatric patients; and (5) identifying patients with renal impairment who would need to follow up with their primary or specialty care provider for monitoring and dose adjustments (see Figure 1). Conditions screened for were age, seizure disorder, pregnancy, breastfeeding status, other currently prescribed medications of interest, antibiotic allergies, and renal disease. Based on the answers to this question set, an antibiotic medication assignment was made by the screeners using an algorithm. Pediatric dosage was determined by screeners using a set of pediatric dosing guidelines. Patients who identified themselves as having renal impairment or as being on dialysis were given a patient information sheet with instructions to follow up with their healthcare provider. Answers to all screening questions and medication assignments were documented in the antibiotic screening database and on the patient script, which was collected prior to each patient's exiting the clinic.
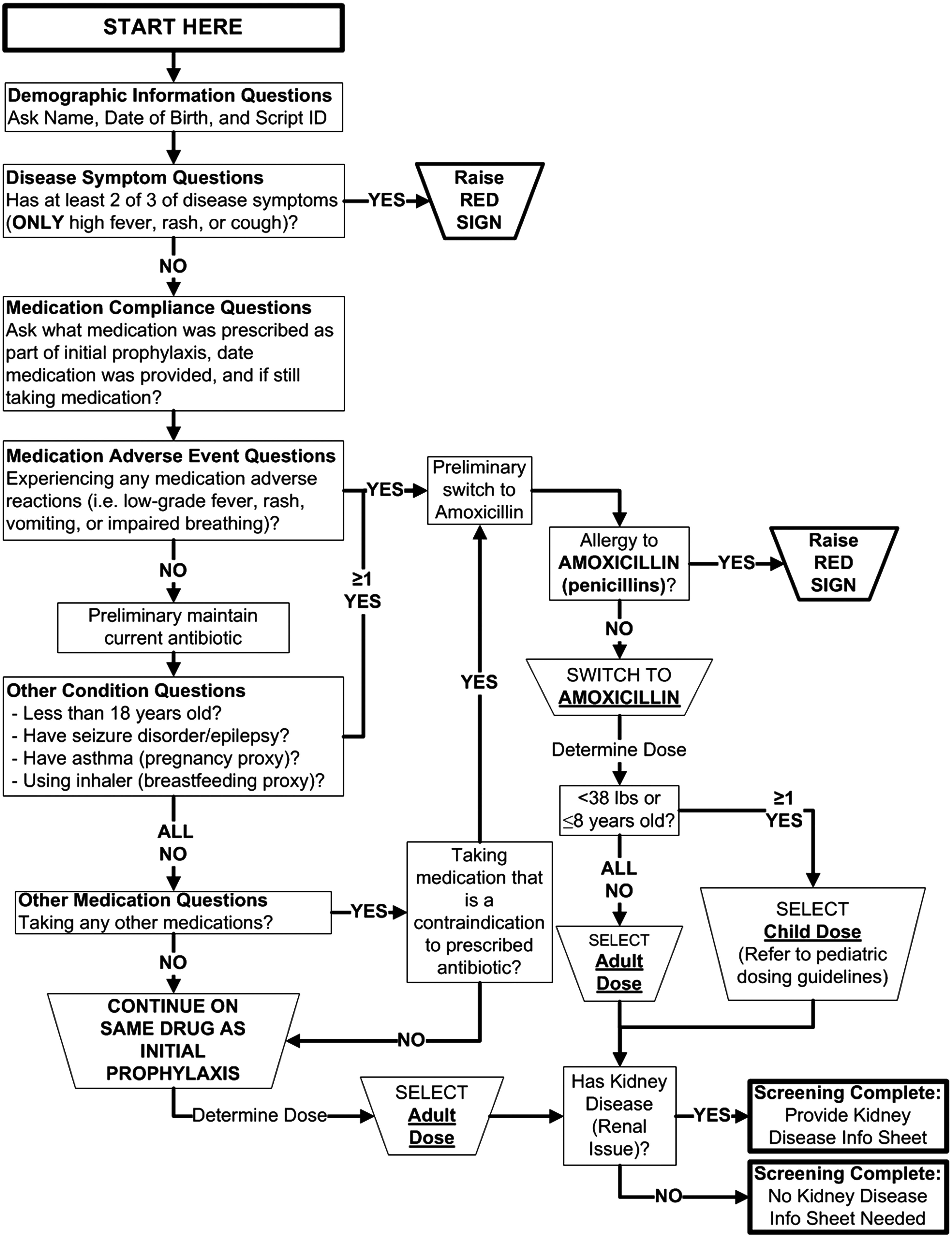
Expanded Screening Process Devised by PDPH: (1) gathering patient information; (2) screening for symptoms of disease; (3) assessing medication regimen; (4) ensuring correct dosage for pediatric patients; (5) identifying patients with renal impairment.
Vaccination
Seasonal influenza vaccine administered in the clinic was Afluria® injectable vaccine in multidose vials, which required staff to draw 10 doses into syringes per vial. A separate electronic database was used to capture vaccine administration records for students who received influenza vaccine; the database was populated with real identification, screening, and product information.
Staffing Model
Each antibiotic screening station consisted of 1 staff member who asked all of the screening questions, determined the appropriate antibiotic for the 50-day regimen, populated the electronic database accordingly, and handed medication to the patient. A single vaccination station consisted of 2 screeners, 1 vaccinator, and 1 vaccine drawer. Vaccine screeners captured real identification and demographic information, interviewed patients for vaccine contraindications, and collected vaccine information (product, expiration, site of vaccination, and vaccinator) in the vaccination database. Planners assumed that the antibiotic screening process would take longer per patient and therefore decided to implement a dual-step process, with patients first being processed at a screening station and receiving their antibiotic assignments and then progressing to a vaccination station to receive their injection. In total, the clinic was comprised of 4 antibiotic screening stations and 2 vaccination stations, with a total staff complement of 15 people, including 2 line staff and 1 clinic medical director.
Data Collection and Analysis
Throughput was assessed by counting the number of screening forms captured over the course of clinic operations. To get a more accurate measure of maximum throughput, only the forms that were collected when the clinic was fully saturated (ie, only when there was a queue of people waiting to enter the clinic) were included to estimate maximum throughput. Processing times for the antibiotic screening and dispensing step and processing times for the vaccine screening and administration step were reconstructed for each patient using database records. Overall patient processing times were reconstructed by matching records between the 2 databases using the patient's name and date of birth and adding together medication screening processing times and vaccination processing times. Antibiotic assignment accuracy was assessed for both the type of medication and dose dispensed by comparing the medication assignments made in the antibiotic screening database to the script key. Data were analyzed using Microsoft Access, Microsoft Excel, and SAS software, Version 9.3 (SAS Institute, Inc, Cary, NC).
Results
Throughput and Processing Times
The clinic observed a throughput rate of 92.5 people processed per hour, and the estimated maximum throughput (controlled for saturation) was 94.6 people processed per hour. This saturated throughput extrapolated over 4 antibiotic screening/dispensing stations and 2 vaccination stations equated to 23.7 persons per station per hour and 47.3 persons per station per hour, respectively. Records for 185 patients were created in the databases over the course of the 120 minutes of clinic operations. Only processing times collected during saturated clinic operations were used to better estimate the maximum model processing time (n=169). Records captured when the clinic was not fully saturated were excluded from the processing time analysis (n=16). The mean processing times for the 2 steps of this clinic were 2.57 minutes per person for the antibiotic screening step and 2.58 minutes per person for the vaccination step. The mean total processing time was 5.15 minutes per person, which did not account for any wait time between the antibiotic and vaccine stations (Table 1). The total processing time improved from 5.66 minutes per person during the first half-hour interval to 5.20 minutes per person (p=0.01) during the second half-hour interval and 4.80 minutes per person (p<0.001) during the third half-hour interval.
Summary of Dual-Model Mass Prophylaxis Patient Processing Times During Fully Saturated Clinic Operations (minutes)
An additional pediatric dosing step is needed.
Total Processing Time excludes gap time between stations.
Medication Assignment Accuracy
Of the 185 patients screened using the antibiotic database, 184 (99.5%) received the correct medication type assignment, 183 (98.9%) received the correct medication dose assignment, and 182 (98.4%) received both the correct medication type and dose assignment.
Discussion
PDPH successfully exercised a more medically responsible expanded screening process for the provision of follow-up medications and vaccine in response to a widespread bioagent release. This was the first time (to our knowledge) that a model for a second-visit POD was tested under exercise conditions and for which throughput and accuracy data have been collected. The baseline data collected from this exercise provide a reference point to determine public health capacity to serve large populations during responses where expanded screening or multiple interventions are indicated. Table 2 provides estimates of population sizes served and resources needed, which can be used by other local health agencies to inform the development of their own multi-visit and/or multi-intervention mass prophylaxis models, as well as to provide a framework for exploring the optimal division of labor between public health agencies and the healthcare provider community. Given existing staff and supplies, PDPH estimates that it could operate this expanded screening model to serve approximately 22.3% of its entire 1,526,000 population over a 6-day period (assuming dispensing operations occurred for 12 hours each day). Further application of this data presents several noteworthy implications for long-term mass prophylaxis planning.
Extended Screening Dual-Model Throughput Extrapolation Estimates for Larger Mass Medication Responses a
Assuming a 6-day timeframe is available for long-term mass medication dispensing operations.
Given the 2014 local health department (LHD) clinic model, 1 dual-step processing unit above is equivalent to 2 antibiotic screening/dispensing stations, 2 vaccine screening stations, a 1-vaccinator station, and a 1–vaccine drawer station.
Assuming a fully saturated model. Throughputs extrapolated from 2014 LHD clinic data.
Staff estimates based on the number of staff used in the 2014 LHD clinic model at stations (antibiotic screeners/dispensers, vaccine screeners, vaccine drawers, and vaccinators). This is the minimum number of staff needed, assuming each person used to staff the clinic will work on a rotating 12-hour on, 12-off basis.
Staff estimates based on ratio of staff at stations to other staff in POD (leadership staff and line staff) used in the 2014 LHD clinic model. The number of staff at stations was multiplied by a factor of 1.5 to get the total staffing estimate. This is the minimum number of staff needed, assuming each person used to staff the clinic will work on a rotating 12-hour on, 12-off basis.
To reduce the challenges associated with sustaining operations for a presumed jurisdiction-wide exposure, epidemiologic investigations and environmental assessments should attempt a more precise determination of exposed people to limit the number indicated for full-course postexposure prophylaxis. However, assuming that all of the residents of a densely populated jurisdiction are recommended to receive full postexposure prophylaxis, it is likely, based on the numbers presented above, that additional options would need to be implemented to ensure provision of the additional 50-day supply by the tenth day of the response.
First, health departments could defer first dose vaccine administration to a later time, thus allowing the use of the head-of-household model for continued antibiotic medication dispensing. One of the advantages of this strategy is that it allows established closed PODs that dispense only oral medications to assist in this phase of the response, which could be of substantial benefit to jurisdictions with robust closed POD plans. To ensure operational readiness, health departments should provide long-term mass prophylaxis training to established closed PODs in order to acclimate staff to the expanded antibiotic screening process.
Second, dispensing operations could potentially occur for up to 24 hours per day. In theory, this strategy could double the population served, but staff fatigue and responder exhaustion would increase and likely interfere with dispensing accuracy.
Third, health departments could limit the number of additional screening questions to expedite patient processing, but this strategy may sacrifice patient adherence, safety, and optimal health outcomes while imposing additional demands for health services on clinical providers if adverse events result.
Finally, modifying patient intake to a paper-based system could expedite patient processing as screeners would not have to capture identification or demographic information. This option presents several disadvantages, however, including inhibiting use of an electronic database, which could be very useful for tracking adverse events, discontinuing medications, and arranging future appointments.
The use of electronic data capture to collect patient information increases the capacity of a health department to monitor medication-related adverse events over the course of the response when compared to a strictly paper-based system. The information collected in the databases could be used to follow up directly with patients who experience complications or miss appointments, and the database records could also be analyzed to detect trends of misuse, noncompliance, and/or adverse events. This information could lead to altered prophylaxis recommendations over the course of the response. Though the electronic screening database offers advantages with respect to patient tracking and monitoring, on-site electronic data capture capabilities during a large-scale response may be limited by the quantity of available laptop computers with the appropriate software installed (Table 2). In situations where the technological needs exceed the available resources, health departments may need to consider alternative approaches, such as prioritizing laptops at certain response sites and/or using paper forms.
Planners did not have previous experience with either the expanded screening process or the use of a single staff member at each antibiotic station to simultaneously conduct screening, data entry, and dispensing functions. Therefore, determining a clinic model with an appropriate ratio of antibiotic dispensing stations to vaccination stations was challenging. The mean medication screening processing time of 2.57 minutes was nearly identical to the mean vaccine administration time of 2.58 minutes. These measures represent the amount of time that a patient was present at each particular station. During the clinic, stations remained saturated for the majority of operations, and there was very little lag time observed between the antibiotic screening stations and vaccination stations. These results validate the dual medication and vaccination staffing model used in this clinic. Using twice the number of antibiotic screening stations as vaccination stations proved optimal for the staff roles, screening processes, and functions performed during this clinic.
Correct medication assignments correspond to safer, more tolerable courses of long-term prophylactic medications for patients. The high rate of screening accuracy observed in this clinic (98.4% accurate for both dose and type of medication) suggests that antibiotic screeners/dispensers were able to effectively process patients with a variety of adverse event reactions and conditions of interest and to make correct medication assignments with respect to both type and dose. The antibiotic screening/dispensing process was conducted by health department staff with some familiarity with the initial antibiotic screening process, and these staff received training on the database prior to the clinic. In addition, the detailed screening algorithm and the corresponding formatting of the antibiotic screening database likely played a role in this high rate of accuracy. Screening questions were divided into distinct sections in the database, red guidance text provided warnings, and some programming logic was included to guide screeners based on patient answers. The tools field tested in this clinic demonstrated promise in supporting patient safety during a long-term mass prophylaxis operation.
An estimated 1.7% of the adult population (aged 18 and older) suffers from kidney diseases. 25 While several scripts that included renal disease were incorporated in the exercise to reflect this prevalence, the data collected were insufficient to draw any conclusions about correct processing of renal patients. However, renal patients on extended courses of antibiotics will require close monitoring and possible dose adjustments to ensure safe and effective administration. Renal care networks should understand the impact that such a bioterror event could have on their practices and should work with health departments to assess capacity for patient surge. Given a smaller population to be screened, a longer dispensing timeframe to provide medications, and availability of resources for lab testing and patient follow-up, dose adjustments for renal patients could potentially be managed by some health departments. For moderate to large events, management of dose adjustments by a health department would likely not be possible and would need to be handled by renal care providers.
This expanded screening, multi-intervention model that enables health departments to provide more thorough patient management and ensure patient safety could be adapted for use in a variety of other scenarios. For example, this model would be appropriate for situations where the population to be screened is relatively small and/or the timeframe for providing medications is longer, such as an isolated exposure at a facility, including a response to a white powder event at a mail processing facility due to a positive biohazard detection system (BDS) assay. Additionally, during follow-up visits, when additional courses of vaccine would be provided, a similar model could be used to monitor for signs of disease and adverse events. This model could also be used for other diseases, in addition to anthrax, where the urgent medical clinic would consist of disease screening, provision of antibiotics, and a dose of vaccine (eg, outbreak response to nonserogroup B meningococcal meningitis at a university). Elements of both the dual-model POD set-up and the expanded screening and electronic data capture process can be incorporated into future mass medication responses depending on the urgency, size of population to be screened, prophylaxis needed, and resources available.
Limitations
Some limitations were noted as part of this exercise. First, the population that was assessed was a scripted patient population in a nonemergency setting with a limited number of medical conditions listed on the scripts. The scripts did not simulate those with limited English proficiency or those with physical, mental, or behavioral impairments, all of which would likely decrease throughput in this model. The screening algorithm did not encompass all possible medication contraindications, and only a subset of medical conditions and concomitant prescription medications was selected for the algorithm. The scripts also did not contain any extraneous medical conditions that were not part of the screening process but that would likely exist in reality. Patients concerned about these conditions when taking long-term medication regimens may ask additional questions of screeners, thereby increasing individual processing times and reducing throughput. Another limitation observed with the screening process is the similarity between drug-related adverse event symptoms and actual symptoms of disease. Given that gastrointestinal symptoms and fever may occur as a result of anthrax disease or from a medication adverse event, there could be possible confusion between the 2.5,6,8-10,28
Conclusions
This field test provided PDPH with initial timing and resource estimates for a more medically responsible emergency medication operation involving both disease screening and a 2-step medication dispensing and vaccination process. The window of time between initial postexposure dispensing and the second visit to obtain additional antibiotics and receive vaccine provides health departments with the opportunity to implement methods that enhance medical responsibility by increasing adherence and patient safety and decreasing the burden on traditional healthcare providers who will be overwhelmed in a large-scale public health emergency. Determining and effectively planning for the division of labor between public health agencies and healthcare providers during large-scale, long-term antibiotic administration is crucial to responsible patient management. Despite the fundamental importance of clearly defining and training for agreed upon roles, gaps continue to persist at the local level that will impair response capabilities and ultimately compromise patient safety. Additional work is needed to forge further ahead into this still largely unexplored frontier in order to better understand the likelihood of adverse events and nonadherence during a large-scale, long-term mass prophylaxis response and to optimally balance the breadth and length of an expanded secondary screening process with the safe and timely provision of the necessary interventions.