
Abstract
Antibiotic resistance is one of the world's most pressing public health problems. Historically, most drug-resistant bacteria have emerged in hospital settings, yet the vast majority of antimicrobials used in humans in the United States are administered in outpatient settings. Strong collaboration between physicians and pharmacists in the development of antimicrobial stewardship programs in outpatient settings is thus a critical strategy for curtailing antibiotic resistance. Recently, pilot projects have been launched in 3 states that pair physicians and community pharmacists under a Collaborative Practice Agreement (CPA) to treat patients with influenza and group A Streptococcus (GAS) pharyngitis. Under this model, community pharmacists use rapid point-of-care tests to guide clinical decision making and initiate treatment as appropriate under a physician-led, evidence-based protocol. Experience with this research initiative has suggested this model can lead to more judicious use of antibiotics and antivirals, improve public health, and provide safe and convenient care for patients.
Historically, most drug-resistant bacteria have emerged in hospital settings, but the majority of antimicrobials used in humans in the US are administered in outpatient settings. Strong collaboration between physicians and pharmacists in the development of antimicrobial stewardship programs in outpatient settings is thus a critical strategy for curtailing antibiotic resistance. Pilot projects have been launched in 3 states that pair physicians and community pharmacists to treat patients with influenza and group A streptococci (GAS) pharyngitis. Experience with this research initiative has suggested this model can lead to more judicious use of antibiotics and antivirals, improve public health, and provide safe and convenient care for patients.
A
Historically, most drug-resistant bacteria have emerged in hospital settings. 4 As a result, it is in the inpatient setting that most efforts to control the spread of resistant bacteria have been focused. The vast majority of antimicrobials used in humans in the US, however, are administered in outpatient settings. According to 2 recent studies, antibiotics were prescribed during 21% of all pediatric and 10% of all adult ambulatory care visits in the United States.5,6 Unfortunately, both studies deemed at least 25% of this use to be unwarranted. Thus, it comes as no surprise that drug resistance among bacteria in the community is increasing. Pathogens such as methicillin-resistant Staphylococcus aureus and drug-resistant strains of Escherichia coli, Streptococcus pneumoniae, and Neisseria gonorrhea have all increased significantly in the ambulatory setting. 4
Preventing and reducing antibiotic resistance in the community is thus a critical public health imperative, but the large size and diversity of the outpatient sector pose significant challenges to achieving progress. Efforts to date have commonly focused on decreasing the need for antimicrobials by increasing vaccination rates, developing treatment guidelines, and educating healthcare professionals and the general public about the appropriate use of antimicrobials. 7 Still, little progress has been realized. An estimated one-third to one-half of all antibiotic prescriptions used in the United States are either unnecessary or inappropriately broad spectrum. 8 In one study, 80% of prescriptions for acute respiratory tract infections were not appropriate according to CDC guidelines. 9 In another series that spanned 2 decades, it was reported that 50% to 70% of antibiotics prescribed for pharyngitis were unnecessary and inappropriate.10,11
Thus, to increase the longevity of current antimicrobials, the US will need to develop new strategies to ensure existing antibiotics and antivirals are used appropriately. This will require study of innovative models that address the core reasons for antibiotic misuse. While the reasons that contribute to misuse of antimicrobials are multifaceted, 2 primary drivers are (1) failure to confirm that bacteria are causing the infection, and (2) the prescriber's willingness to satisfy a patient's expectation for an unneeded antibiotic prescription. 4 With respect to the latter, one study showed that doctors prescribe antibiotics 62% of the time if they perceive parents expect them, but only 7% of the time if such expectation is not perceived. 12
To improve antimicrobial use in outpatient settings, the Report to the President on Combating Antibiotic Resistance offered 2 explicit strategies. 2 First, the report calls on the Centers for Medicare and Medicaid Services to include measures that discourage inappropriate antibiotic use as part of its Physician Quality Rating System. Second, the report highlights the need to develop rapid point-of-care diagnostics that provide information to assist in making treatment decisions in a medically relevant timeframe.
We submit that the healthcare system should also consider ways to promote greater collaboration between physicians and pharmacists in the development of antimicrobial stewardship programs in outpatient settings. For infections such as influenza or group A Streptococcus (GAS) pharyngitis, physician-pharmacist collaboration is ideal because (1) many patients first seek symptomatic relief with over-the-counter (OTC) medications available at pharmacies; (2) most patients require only management of their symptoms and monitoring; (3) prompt identification of those with the actual pathogen and early treatment are key to optimizing patient health outcomes and reducing infectivity; (4) the choice of appropriate treatment for uncomplicated patients is relatively straightforward; and (5) rapid point-of-care tests can be used to better guide treatment decisions. 13 Recently, pilot projects have been launched in 3 states (Michigan, Minnesota, and Nebraska) that fostered strong collaborations between physicians and community pharmacists in the development of innovative disease management programs for patients with influenza and GAS pharyngitis. 13 Experience with this research initiative has suggested positive progress toward reducing the inappropriate use of antibiotics. This article outlines the innovative physician-pharmacist disease management programs that have emerged, summarizes published evidence from this early pilot initiative, and makes recommendations for the expansion of this program.
Physician-Pharmacist Collaboration
Nearly all outpatient prescriptions for an acute infectious condition are filled and dispensed at outpatient community pharmacies in the United States. In filling a prescription for an antibiotic or antiviral, a pharmacist will traditionally check to ensure the accuracy of the dose, screen for drug interactions or contraindications, and counsel the patient on the appropriate use of the medication, among other things. The evolution in the education and training of pharmacists, as well as the emergence of new technologies such as Clinical Laboratories Improvement Act (CLIA)–waived point-of-care tests, have created opportunities for pharmacists to take on an enhanced role in antimicrobial stewardship in close collaboration with physicians. Since the early 2000s, the doctor of pharmacy degree (PharmD) has become the sole entry-level credential to practice as a pharmacist in the US. 14 The PharmD emphasizes a diverse curriculum that provides extensive education on the safe and appropriate use of medications as well as direct patient care roles such as collection and interpretation of laboratory and physical assessment data.15,16 As one example of their changing role, pharmacists in all 50 states now have the ability to provide immunizations, and 20% of all influenza vaccinations are now provided in pharmacies. 17
Pharmacists do not, however, have direct prescriptive authority in most situations. In many states, a prescriber may enter into a formalized Collaborative Practice Agreement (CPA) with a pharmacist and delegate to him or her the authority to initiate, modify, or discontinue medications under tightly controlled conditions. 18 The CPA can set parameters around the specific patient care functions that pharmacists are authorized to perform, the patient populations the pharmacist can and cannot manage, the therapies that may be provided, and the procedures for reporting and follow up. In its best practices for CPAs, CDC has stated that physician-pharmacist CPAs “can reduce fragmentation of care and improve health outcomes if they are set up properly.” 18
Thus, a CPA serves as a strong foundation for a collaborative, interprofessional disease state management program for infectious diseases. An early example of a CPA for influenza emerged from a collaboration among the Seattle & King County Advanced Practice Center, the Northwest Center for Public Health Practice, the Washington State Pharmacy Association, and the Washington State Board of Pharmacy during the 2009 H1N1 influenza pandemic. 19 The partners created a CPA that is triggered during a public health emergency that requires mass prophylaxis with antivirals. For example, in the event of a pandemic, a medical director of a local health department could enter into CPAs that allow pharmacists, who are specifically covered under the agreement, the ability to provide a patient assessment that screens for high-risk criteria and symptoms of influenzalike illness (ILI). Based on the results of this assessment, the pharmacist has the delegated authority to initiate a prophylaxis or treatment dose of either oseltamivir or zanamivir. 20 The CPA would be active only during an emergency, however, and pharmacists would not have the authority to initiate antivirals for patients during seasonal influenza under this agreement.
Such a model has received support from the general public. In 2012, the Institute of Medicine's Forum on Medical and Public Health Preparedness for Catastrophic Events held a series of 3 workshops in California, Montana, and Tennessee to explore the public's perception of various models to enhance access to antiviral medications during an influenza pandemic.
21
One of the strategies that was put forth for public comment was a physician-pharmacist CPA model that would allow pharmacists to initiate antiviral medications under specific prescribing guidelines developed by flu experts. The IOM reported:
Many participants across the three workshops expressed a high level of regard for the pharmacist profession. They indicated they would have few reservations about relying on pharmacists to carry out the proposed antiviral prescribing role because they believe local pharmacists are trustworthy and knowledgeable about prescription drugs.
21
Although physician-pharmacy CPAs related to infectious diseases have been described, they have primarily been explored in the context of a public health emergency such as pandemic influenza. In these models, pharmacists dispense antimicrobials based on guidelines related to patient symptoms alone. 22 Extrapolating this model to nonemergency situations warrants consideration for 2 reasons. First, if the public health community intends to leverage a CPA model for mass prophylaxis in the context of an emergency situation, it makes sense to build the community infrastructure to support this preparedness goal during nonemergencies. It is widely accepted that emergency response works best when it builds off of everyday practice. Rubin and colleagues described the difficulty physicians and pharmacists had in trying to rewrite and implement CPAs in real-time in New York, pursuant to a gubernatorial executive order during Hurricane Sandy. 23 Second, CLIA-waived, point-of-care tests for influenza and GAS have been approved with the intent of providing guidance to clinicians in making appropriate treatment decisions. These tests can be incorporated in collaborative disease management programs to help optimize the appropriate use of antibiotics and antivirals. In nearly all states, pharmacists have the authority to use point-of-care tests that are CLIA-waived. The Food and Drug Administration (FDA) defines a CLIA-waived test as one that is “so simple and accurate as to render the likelihood of erroneous results negligible; or pose no reasonable risk of harm to the patient if the test is performed incorrectly.” 24
A recent meta-analysis of rapid point-of-care tests for GAS found that overall estimates for sensitivity and specificity were 0.86 and 0.96, respectively. 25 The authors concluded that these tests “… can be used for the accurate diagnosis of GAS pharyngitis to streamline management of sore throat in primary care … [and] may not require culture backup for negative tests in most low-incidence rheumatic fever settings.” 25 The performance of point-of-care tests for influenza has been scrutinized, and the FDA has set new targets for performance for sensitivity and specificity. 26 Some tests on the market currently meet these new performance guidelines and thus may provide useful information to assist clinical decision making, especially when steps are taken to identify appropriate patient populations and optimize the positive predictive value of the tests.
Thus, employment of a CPA using CLIA-waived point-of-care tests to guide clinical decision making serves as a model to foster a physician-pharmacist partnership for management of influenza and GAS in nonemergency situations. In so doing, a model built on this infrastructure holds promise to optimize use of antibiotics and antivirals in outpatient settings, since the circumstances under which a pharmacist can initiate these agents may be bound by an evidence-based protocol under the direction of the collaborating physician.
Physician-Pharmacist Seasonal Influenza Model
Studies have shown that a physician-pharmacist collaborative management model for influenza can not only shorten the time to receipt of antiviral, but also achieve this outcome safely and in a manner that reduces inappropriate use of antivirals. A sample flowchart for a physician-pharmacist collaborative influenza management program is shown in Figure 1.13,27
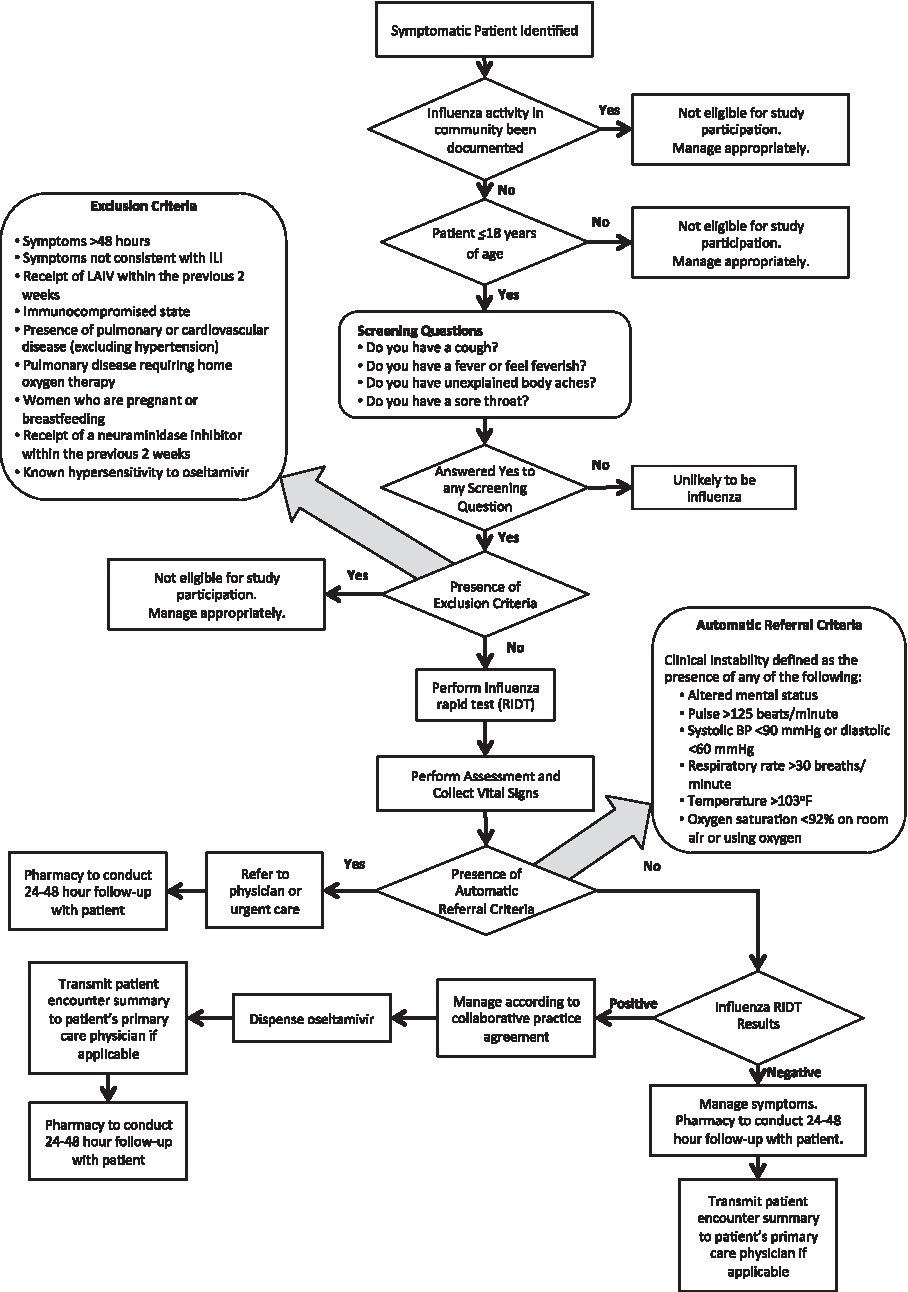
Community-Based Influenza Disease Management Program 13
According to this model, pharmacists would screen all individuals 18 years of age and older who complained of symptoms consistent with ILI. 13 A nasal swab specimen would be collected from individuals to use in a CLIA-waived rapid influenza diagnostic test (RIDT). To maximize the positive predictive value of the tests, patient screening and enrollment would be conducted only when local influenza activity has been documented by state or federal surveillance data. Additional data gathered via physical assessment and vital signs collection (eg, pulse, blood pressure, respiratory rate, temperature, and oxygen saturation) would be assessed and used to guide treatment decisions. 13 Accordingly, the collaborating physician can establish thresholds for each of the aforementioned parameters, based on evidence-based guidelines and their clinical practice, so that patients with a high risk of influenza-related complication and clinical instability can be referred to another healthcare setting as appropriate. For patients who are deemed to be clinically stable, meet criteria of ILI, and have a positive rapid influenza diagnostic test, the physician may authorize the pharmacist to dispense the appropriate antiviral therapy, such as oseltamivir. Essential to such a program is the provision of follow-up care to the patient and communication with the collaborating prescriber and the patient's primary care provider to ensure coordinated team-based care.
A program based on such a model was piloted between December 15, 2013, and April 5, 2014, at 55 pharmacies in 3 states (Michigan, Minnesota, and Nebraska). 13 A total of 121 patients were screened, with 75 meeting criteria for inclusion in the study. Of the patients presenting with ILI, only 8 (11%) had a positive rapid influenza diagnostic test result. Under the CPA, pharmacists were unable to dispense oseltamivir for patients who did not test positive with the rapid influenza diagnostic test, nor were they able to initiate an antibiotic. The study demonstrated that a collaborative physician-pharmacist disease management program can lead to judicious use of antivirals and safely avoid inappropriate antimicrobial use in this patient population. No adverse outcomes were reported by patients in the study. 13 By contrast, in a recent review of 5 ambulatory care sites using a traditional physician prescription model, only 15% of patients with polymerase chain reaction (PCR)–confirmed influenza received an antiviral medication, yet 30% inappropriately received 1 of 3 antibiotics.25,28
Thus, given the nature of the CPA, pharmacists must adhere to the evidence-based guidelines as established in the protocol. Although a common complaint in traditional models of care is that patients have an expectation of receiving an antibiotic, the pharmacy model achieved a patient satisfaction rate of greater than 90%, despite only 11% of the patients receiving oseltamivir. 13 One explanation for this may be that pharmacists were able to explain the results to the patients and work with them to select an appropriate OTC medication for symptomatic relief in the event the patient tested negative. Further, 39% of the patients presented to the pharmacy after normal physician office hours, and 35% of the patients reported that they did not have a primary care physician. These facts indicate that the alternative choices available to many of these patients included doing nothing or seeking treatment in an urgent care center or emergency department. Therefore, the model studied may not only improve access to care for patients without a medical home, it may also decrease inappropriate healthcare use. 13
Physician-Pharmacist Group A Streptococcus Model
A sample flowchart for a physician-pharmacist collaborative GAS program is shown in Figure 2. 29 According to this model, pharmacists would screen all individuals 18 years of age and older who complained of symptoms consistent with pharyngitis. 29 Patients are then evaluated for clinical instability (ie, conduct a physical assessment and collect vital signs) and factors that would place them at high risk for complications. A tool such as the Centor Score may be used to further increase the probability that the source of infection is bacterial. At this time, a point-of-care test for GAS may be employed to provide additional guidance. A reasonable population for management may be clinically stable adult patients who have a Centor Score ≥1 and a positive GAS point-of-care test. For such a patient, the collaborating physician may authorize the pharmacist to dispense appropriate therapy. Essential to such a program is the need to provide follow-up care to the patient and communicate with the collaborating prescriber and the patient's primary care provider to ensure coordinated team-based care.

Community-Based GAS Pharyngitis Disease Management Program 29
A program based on such a model was piloted between December 15, 2013, and September 1, 2014, at 55 pharmacies in 3 states (Michigan, Minnesota, and Nebraska). 29 A total of 316 patients were screened, and 273 were eligible for testing. Only 48 patients (17.5%) had a positive test result and received amoxicillin or azithromycin per the CPA. This represents a dramatic reduction in antimicrobial use compared to the rates of 60% to 80% reported for adult pharyngitis reported in the literature.10,11 A 17.5% rate of antibiotic use in an adult population with pharyngitis is closely aligned with data that suggest that 5% to 15% of cases of pharyngitis in this cohort are caused by bacteria. No adverse outcomes were reported by patients in the study. 29 This model again showed judicious use of antibiotics yet still achieved an 84% patient satisfaction rating. Similar to the influenza model, 43.9% of the tests were provided outside of traditional physician office hours, and 43.9% of the patients reported not having a primary care physician. 29
Discussion
A physician-pharmacist disease management program anchored by a CPA and point-of-care tests can thus promote the judicious use of antibiotics and antivirals while maintaining patient satisfaction with the care provided—even in the absence of receiving a prescription. If expanded, patient management models such as these could make a meaningful difference in reducing overuse and misuse of antibiotics in the community. This in turn could have a significant impact on not only rates of antimicrobial resistance in the community, but also on antibiotic use in the hospital setting, the latter often being influenced by a patient's history of prior antibiotic exposure.
The opportunity is significant: Community pharmacists are among the most accessible healthcare providers; 92% of all Americans live within 5 miles of a pharmacy. 17 In addition, pharmacies are open nights and weekends when many other healthcare provider offices are closed. By entering into a CPA, a physician-pharmacist collaboration for infectious diseases such as influenza and GAS pharyngitis may facilitate earlier identification and treatment in a manner that is consistent with the principles of team-based care such as the patient-centered medical home.30-32
While most CPAs today represent partnerships between outpatient physicians and community pharmacists, state and local health departments may additionally explore CPAs as a way to improve care. In a 2014 policy statement, the National Association of County and City Health Officials (NACCHO) urged its members: “Where feasible, local and state health departments and pharmacies are advised to forge Collaborative Practice Agreements, which authorize pharmacists to administer vaccines, provide medical countermeasures, or provide patient care services under established protocols for certain patients and populations.” 33 By entering into a CPA, the medical director of a state or local health department could set evidence-based parameters for treatment and disease reporting. For the latter, health departments may be able to use data on the number of patients seeking services at pharmacies as an additional real-time data set that could help with surveillance for influenza outbreaks. Additional exploration of this opportunity is warranted.
One challenge to the expansion of this model is state-level restrictions on CPAs. In a 2012 review of state laws, the CDC noted that 36 states allow CPAs in any pharmacy setting. 34 Still, these states vary as to the breadth and depth of the CPAs. For example, some states impose restrictions on the ability of physicians to enter into CPAs or set restrictions on the disease states that may be treated or the types of services that are permitted. One particular challenge to using a CPA for infectious diseases is that some states restrict CPAs to written agreements for individual patients. This would mean a pharmacist could only treat a patient for influenza if a pharmacist has a CPA signed in advance with the patient's primary care physician. Since research has noted that more than 1 in 3 patients seeking care for influenza or GAS pharyngitis at a pharmacy did not have a primary care physician in the first place, a patient-level CPA restriction would suggest these patients would need to be referred to an urgent care center or an emergency room for service. To remedy this, research could examine restrictions that are currently in place related to CPAs and study the impact of these restrictions on patient care outcomes.
Several potential limitations should be noted. First, as discussed previously, some point-of-care tests for influenza have been criticized for poor performance. 26 Some tests on the market currently meet guidance set by the FDA for future performance, however, and new CLIA-waived PCR influenza tests have emerged that may further minimize the potential for false-negatives. Still, because of the potential for false-negatives, it is important for collaborative disease management models to have a process to manage patients who initially test negative. In the studies presented, pharmacists follow up within 48 hours to assess symptom progression and make a referral to care as appropriate. Future research should include a verification of the point-of-care test performance characteristics under pharmacy use conditions.
Second, the antimicrobial usage for the innovative disease management models presented is compared to previous medical literature. It is possible that the patients presenting in this model have different characteristics than patients that present to other care settings. Future research should consider matching patients that present under the pharmacy-physician model to similar patients that present to other care settings.
Lastly, future research should further explore patients who test negative and their use of additional services, such as immunizations, as a result of the pharmacy visit.
Conclusion
As part of a comprehensive strategy to reduce antimicrobial resistance, innovative partnerships between physicians and pharmacists for the treatment of various infectious diseases including influenza and GAS pharyngitis should be expanded. These models can lead to the more judicious use of antibiotics and antivirals, improve public health, and provide safe and convenient care for patients.