
Abstract
Local health departments play a critical role in short-, intermediate-, and long-term recovery activities after a public health emergency. However, research has not explored attitudinal determinants of health department workers' participation in the recovery phase following a disaster. Accordingly, this qualitative investigation aims to understand perceived facilitators and barriers to performing recovery-related activities following Hurricane Sandy among local health department workers. In January 2014, 2 focus groups were conducted in geographically representative clusters of local health departments affected by Hurricane Sandy (1 cluster in Maryland and 1 cluster in New Jersey). Focus groups were recorded, transcribed verbatim, and analyzed to qualitatively assess attitudes toward Hurricane Sandy recovery activities. This analysis identified 5 major thematic categories as facilitators and barriers to participation in recovery activities: training, safety, family preparedness, policies and planning, and efficacy. Systems that support engagement of health department personnel in recovery activities may endeavor to develop and communicate intra- and interjurisdictional policies that minimize barriers in these areas. Development and implementation of evidence-informed curricular interventions that explain recovery roles may also increase local health department worker motivation to participate in recovery activities.
Local health departments play a critical role in recovery activities after an emergency, but research has not explored health department workers' attitudes toward participation in the recovery phase. This qualitative investigation aimed to understand perceived facilitators and barriers to performing recovery-related activities following Hurricane Sandy. Focus groups were conducted in Maryland and New Jersey, and 5 categories were identified as facilitators and barriers to participation in recovery activities: training, safety, family preparedness, policies and planning, and efficacy. Systems that support engagement of health department personnel in recovery activities may strive to develop and communicate policies that minimize barriers in these areas.
L
While research regarding attitudinal determinants of local health department worker participation in disaster recovery activities is unprecedented, a growing body of literature suggests that workers' willingness and ability to engage in disaster response activities is directly related to their attitudes, beliefs, and perceptions, and especially their beliefs related to efficacy.2-8 “Efficacy” is composed of self-efficacy, or an individual's perception of his or her ability to execute a particular task, and response efficacy, or the perception of the performance of the task that yields the desired outcome. 9 Prior research has highlighted the impact of self-efficacy on performance, finding that increased self-efficacy, in particular, is associated with increased willingness to respond to work during a disaster response.2,3,5,7,10 This research has been guided largely by the Extended Parallel Process model, which incorporates dimensions of threat and efficacy to understand behavior change. 9
Understanding the attitudinal determinants, including efficacy, of local health department worker recovery activities is important to ensuring a national capability for communities to bounce back from disaster. The 2014 Forces of Change Survey administered by the National Association of County and City Health Officials (NACCHO) found that 47% of local health departments reported expanding services in at least 1 programmatic area in 2014 compared to 2013. 11 Despite overall service growth, the number of full-time equivalent (FTE) health department personnel decreased by an estimated 12% (from 166,000 to 146,000) between 2008 and 2013. 12 As local health departments are already doing more with less, it is important to understand what drives and facilitates health department workers' participation in disaster recovery activities and to endeavor to develop a system that supports this engagement.
Guided by the findings from the aforementioned similar investigations into the impact of efficacy and attitudinal perceptions on the public health emergency workforce's willingness to respond,2-6 this research sought to identify attitudinal determinants of local health department workers' participation during the recovery phase of Hurricane Sandy. Barriers and facilitators to health department workers' participation in recovery activities and pertinent efficacy considerations in the disaster recovery context were also explored.
Methods
Local health departments in Maryland and New Jersey were targeted for inclusion in the study via purposive and subsequent snowball sampling techniques 13 from among the counties and jurisdictions affected by Hurricane Sandy. In January 2014, 2 state-specific focus groups were held. A primary point of contact was identified in each local health department to facilitate the recruitment of health department workforce participants from a variety of professional strata.
Both focus groups were between 1 and 2 hours in duration. The facilitator used a focus group guide designed to elicit discussion in the following domains: (1) potential barriers to communicating and receiving needed information in recovery activities; (2) impediments to recovery surveillance efforts and how these impediments might differ by types of surveillance activities; and (3) hurdles to effective integration and coordination of recovery efforts between public health departments and other organizations across the “public health preparedness system.” 14 An additional member of the research team was present for note-taking and participated in post–focus group peer debriefing.
Each focus group session was audiorecorded and transcribed. A code book was deductively developed and iteratively modified throughout the coding process to guide the thematic organization of transcribed text. 15 Two members of the research team systematically applied codes to all data using NVivo 10 software (Burlington, MA). Analytic memos were developed to summarize major themes that emerged.
This study was reviewed and approved by the Johns Hopkins Bloomberg School of Public Health Institutional Review Board (IRB) and the Uniformed Services University of the Health Sciences IRB, which determined that this study did not meet the criteria defining human subjects research. The Maryland Department of Health and Mental Hygiene IRB also reviewed and approved this study and determined it to be exempt research.
Results
The final sample was composed of 8 local health departments, 5 from Maryland and 3 from New Jersey. A total of 27 health department employees participated in the focus groups: 15 in the Maryland focus group and 12 in the New Jersey focus group. Focus group participants had a diverse set of professional roles and local health department recovery-phase responsibilities, including clerical and support staff, administrative leadership, emergency preparedness personnel, and clinical workers.
Facilitators and Barriers
Participants described 5 major themes as barriers to and facilitators of local health department workers' performance of recovery activities during the aftermath of Hurricane Sandy: training, safety, family preparedness, policies and planning, and efficacy (Figure 1). These barriers to and facilitators of recovery role performance are described below. Focus group participants' suggestions for enhancement of health department workers' self-efficacy and response efficacy are summarized in Figure 2.
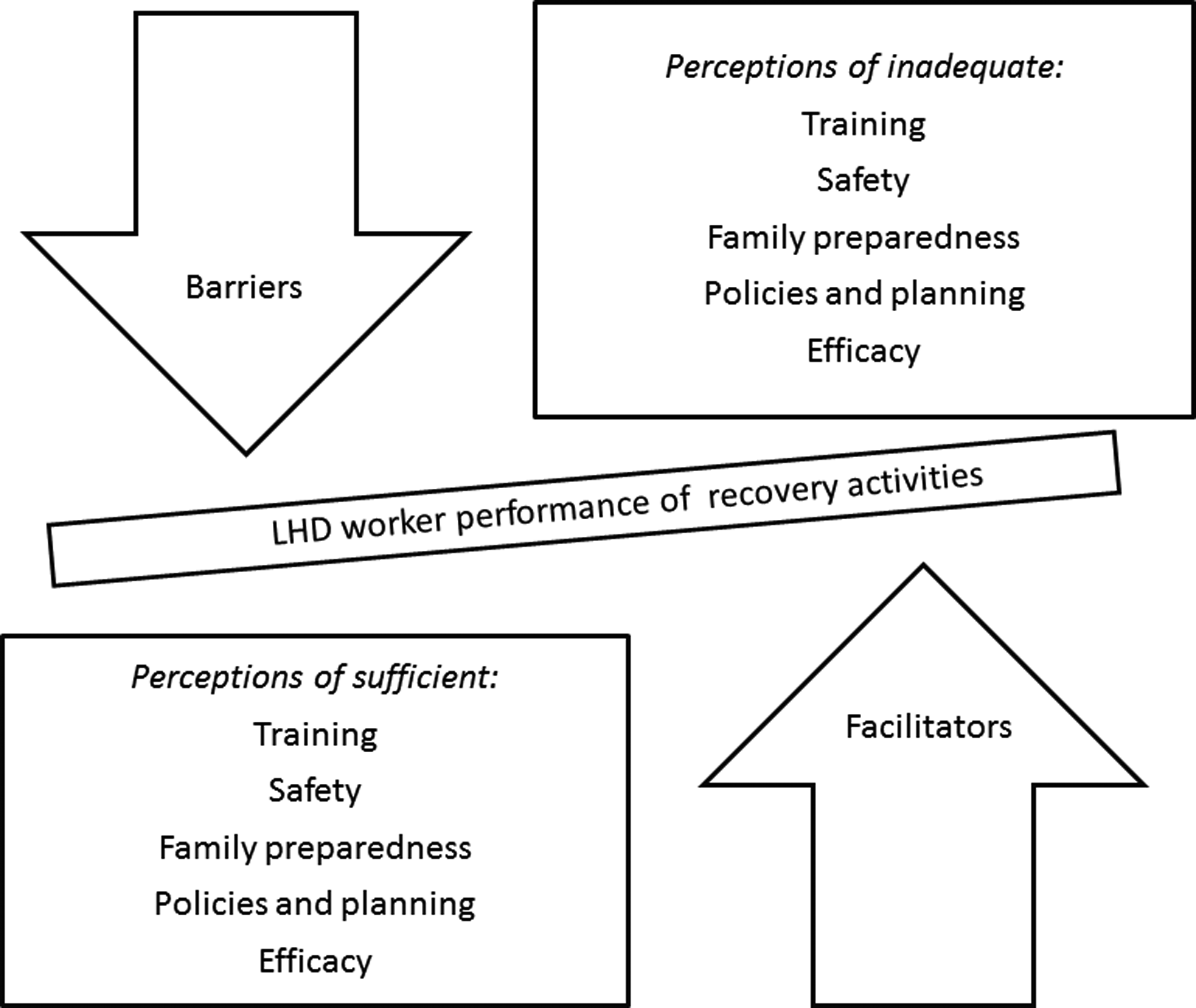
Major Thematic Categories Found to Be Facilitators and Barriers to Participation in Recovery Activities
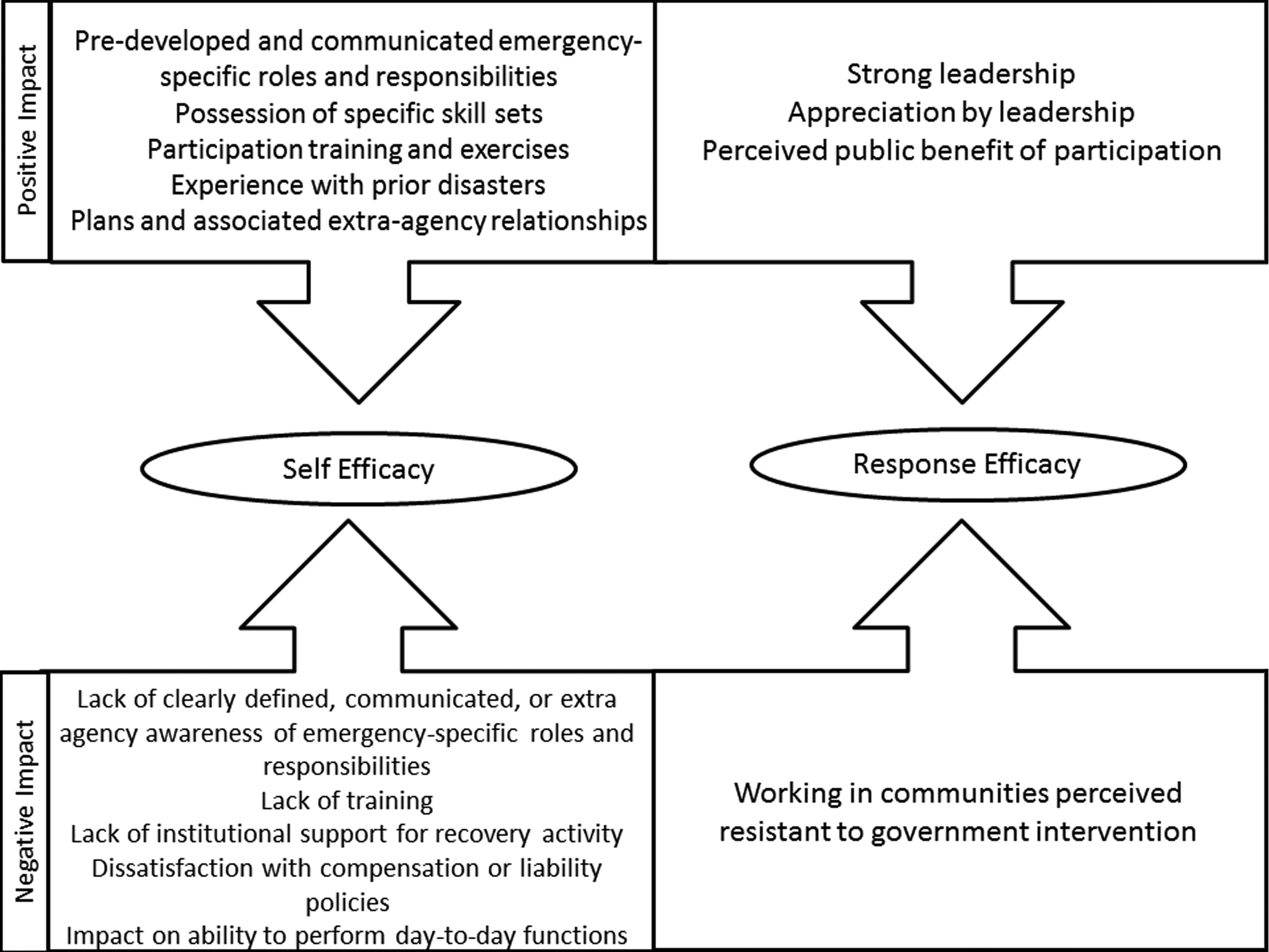
Positive and Negative Determinants of Local Health Department Worker Efficacy in Recovery
Training
Participants reported that emergency preparedness training, including role-specific training, incident command system (ICS) training, and psychological first-aid training, either improved or could have improved recovery activity performance. Participants suggested that additional interjurisdictional training and emergency exercises, particularly between state and local agencies, could facilitate recovery activities. Training administered at the start of employment (“onboarding” education) and assignment of new health department staff to specific emergency responsibilities at the time they were hired was described as having encouraged a culture of preparedness and facilitated understanding of roles and responsibilities in recovery activities. The inclusion of all staff in emergency preparedness training and exercises, including ancillary/support staff and others not traditionally involved, was encouraged.
Likewise, insufficient training of both regular and supplementary personnel was described as a barrier to effective participation in disaster recovery activities. Specifically, local health department personnel with particular skill-based roles or who operate under defined scopes of practice (eg, public health nurses) described feeling underprepared for the altered responsibilities that were assigned to them following Hurricane Sandy.
Safety
Local health department worker perceptions of personal safety influenced their ability to perform recovery roles during the short-term, acute disaster recovery period. Participants believed that higher perceived levels of safety both at work and while traveling to and from work would enhance health department worker participation in recovery activities.
However, participants articulated concerns regarding the level of perceived safety in the workplace, particularly for local health department workers who staffed emergency facilities that were geographically distant, run by external agencies, or located in areas that were perceived as unsafe. The inability to travel to and from work safely following a disaster was also perceived as an impediment to recovery activity performance. In addition, a perception of compromised personal safety appeared to be related to negative perceptions of the disaster recovery experience and decreased trust in organizational leadership and procedure.
Family Preparedness
Higher levels of family preparedness were perceived to positively facilitate local health department workers' participation in recovery activities. However, participants reported general willingness to participate in recovery activities with few exceptions among health department workers with varying levels of family preparedness.
Participants noted that, in general, all expected employees reported to work except in cases where they had been directly affected by the storm. Participants recognized the need to be flexible in the event that a staff member was personally affected by the emergency event. However, participants stated that there were a few health department workers who consistently used family preparedness as an excuse for nonparticipation in recovery activities.
Policies and Planning
Local health department emergency policies and plans widely influenced workers' perceptions of willingness to participate in recovery activities. For instance, positive interagency and intergovernmental partnerships developed through ongoing preparedness processes (eg, planning and training) were perceived to have facilitated recovery activities. In one focus group, a postevent inter- and intrajurisdictional recovery committee was described as having opened lines of communication and improved planning for future events. Participants reported that expanding services to accommodate the needs of other jurisdictions and providing staffing support increased some communities' ability to continue with long-term recovery activities. Several participants felt the faith-based community and nongovernmental partners contributed significantly to recovery activities.
Inadequate policies and planning were described as being a barrier. Participants consistently cited challenges with the vertical intergovernmental integration of recovery plans as a hindrance to the recovery process. They found that state and federal recovery priorities and timelines were, at times, not aligned with local recovery plans and community-based needs. Moreover, existing resource and communication channels from local to higher levels of government (eg, the state and federal levels) were not perceived as having the capacity to consistently fulfill recovery resource requests. Informal relationships were described as having been more efficient than official channels for resource coordination and collection. In addition, participants noted that some local health department staff funded by federal grants could not be used in the recovery process because of strict and narrowly defined scopes of responsibility in the grant language and an absence of planned reassignment for emergencies. They also expressed frustrations with state agencies' lack of understanding of health department staff roles.
Inconsistent compensation policies and their application were also perceived to negatively affect local health department staff's willingness to participate in recovery activities. As an example, leave time accrued from disaster-specific roles could result in personnel taking time off during nondisaster times, impeding the performance of everyday functions in the long term. In addition to compensation policies, participants reported perceptions of insufficient liability and workers' compensation provisions for local health department staff (eg, because it was unclear whether they were acting as volunteers or as employees and whether they would be compensated for their time). Participants discussed the need for such policies to be developed and communicated in advance of another disaster. Concerns regarding certifications, credentialing, and liability among medical volunteers were also raised, and medical volunteer credentialing practices were perceived to be insufficient.
Self-Efficacy and Response Efficacy
Self-Efficacy
Clear job descriptions and an awareness of personal responsibilities during disaster response and recovery activities were described as having increased health department staff's ability and willingness to perform recovery activities. Participants described emergency preparedness training and exercising to be associated with improved staff efficacy. They also found that training provided at the beginning of employment and indoctrination into emergency response, combined with the knowledge of prior recovery experiences of more seasoned employees, facilitated feelings of efficacy. Several participants believed that experience with previous weather-related emergencies, natural disasters, and public health crises (eg, Hurricane Irene and H1N1 novel influenza) helped prepare local health department staff to perform effectively and feel confident and comfortable in carrying out their duties following Hurricane Sandy.
Workers with particular knowledge or specific skill sets (eg, environmental health, food system surveillance, behavioral health service provision, nursing) related to recovery activities expressed high feelings of self-efficacy. While clerical and nonessential employees were perceived as being willing to assist with the recovery activities, their participation was hindered because their responsibilities during emergencies were not well defined and they were used to receiving task-specific directions.
Several local health department staff members expressed either personal feelings or perceived feelings of others that they were not always fully prepared for the altered responsibilities of an emergency. Lack of familiarity with or confidence in performing one's recovery role was described as an impediment to recovery activity willingness. This was exacerbated by a perceived lack of training, lack of clearly defined emergency roles and responsibilities assigned to some workers not traditionally involved in emergency preparedness activities, being asked to perform tasks outside of their normal scope of practice (eg, asking a public health nurse to perform donations management or manage acute medical needs), or being asked to perform a duty without sufficient institutional support (eg, sending only 1 employee to a shelter).
Response Efficacy
Generally, participants appreciated the importance of their professional role to the overall emergency response. Several participants expressed the importance of strong leadership in influencing this sentiment. One participant felt that acknowledgment and appreciation from leaders, both internally and from the state level, improved the staff's feelings of efficacy. The perceived public benefit of local health department recovery activities was also described to be associated with an increased willingness to participate in recovery activities and feelings of response efficacy.
Perceptions of low response efficacy negatively affected health department workers' desire to participate in recovery activities. For instance, the impact of local health department efforts was perceived to be limited in communities that were resistant to government disaster intervention (eg, those that were perceived to not follow evacuation orders). Also, a lack of experience with a storm of this magnitude affected the willingness of community members to act as advised, and this was reported as discouraging a health department worker's willingness to perform recovery roles.
Discussion
Prior research on the impact of attitudinal determinants of willingness to participate in emergency efforts has primarily focused on the preparedness and response periods. To our knowledge, this is the first inquiry of its kind to investigate the impact of attitudinal determinants on local health department workers' participation during the recovery period. Our results suggest that health department workers conceptualize many of the challenges experienced during recovery in 5 major thematic categories: training, safety, family preparedness, policies and planning, and efficacy.
Our results suggest that role-specific professional disaster recovery training is beneficial to increase levels of self-efficacy and willingness to perform disaster recovery activities among local health department personnel. Health department leaders can support recovery participation by ensuring that all personnel, including staff members not dedicated to emergency management, have recovery-time reassignments, are aware of the nature of the responsibilities they will be expected to fulfill, and are provided with relevant initial and ongoing training opportunities. Based on the perceived importance of feeling necessary and useful to recovery efforts, a process that better defines and provides training for each role could increase overall feelings of self-efficacy and response efficacy.
The representative professional diversity of the focus groups in this study maps onto a variety of recovery-phase activities in local health departments. Such activities include, for example, surveillance, local health department–based communication efforts to area residents, and coordination of shelter operations that can be of significant duration postevent. Future research can seek to translate health department workers' perspectives toward disaster recovery into new, evidence-informed training for enhancing efficacy in the postdisaster context.
Focus group participants associated willingness to perform recovery activities with perceived levels of personal safety. These findings are consistent with research on acute disaster response scenarios, where agencies' clear communication of safety-related policies and procedures was identified as a positive influence on health department employees' willingness to fulfill their professional role expectations. 7 Local health department leaders can endeavor to improve employee perceptions of personal safety by articulating safety policies in advance of a disaster and by providing institutional resources to promote employee safety (eg, providing transportation in hazardous conditions and/or security at facilities where workers provide disaster recovery services).
While focus group participants did not perceive that recovery activities were significantly affected by family preparedness, they did describe the need to accommodate health department personnel personally affected by a disaster. Contingency planning for recovery activities, including the use of volunteer or surge workforces, can be incorporated as part of local health department recovery programs. Plans and associated expectations should be communicated to health department personnel through training programs.
Focus group participants described a number of challenges that either were or could have been ameliorated with adjustments to organizational and government policies and improved predisaster planning. For instance, participants were dissatisfied with perceived inconsistencies in the application of workers' compensation and liability protections, a lack of clarity regarding pay, unclear professional credentialing standards, and perceived indifference to personnel safety. Workers' compensation is generally available only to paid employees when they are injured in the course of their regular work. 16 During the recovery period, when health department employees regularly take on atypical responsibilities, volunteer their time, work nontraditional or extended hours, or operate under supervision outside of their normal chain of command, it becomes less clear whether workers' compensation benefits could or should apply to them in the event of an injury. Several states have initiated an enhancement process to workers' compensation coverage to safeguard volunteer responders, but this has been applied only during periods of government-declared emergencies. 17 Given this variation, local health departments should ensure that all health department emergency-time employees, including supplementary personnel, understand the scope and extent of their workers' compensation benefits during the disaster recovery period.
Participants also cited difficulties with emergency-time credentialing processes and liability protections for volunteers and supplemental paid personnel during disaster recovery. During emergency response and recovery, credentialing processes are often tied to liability protections. A patchwork of emergency laws permits healthcare professionals to provide care in jurisdictions where they are not currently licensed as part of disaster response. 18 For example, the Emergency Management Assistance Compact allows licensed healthcare providers employed by state or local governments to temporarily provide care in affected states during a declared emergency. 19 Many states additionally have their own credentialing and licensure portability laws, which allow out-of-state providers, including volunteers, to practice in a state facing an emergency. 20 These state and local policies generally provide for liability protections for individuals participating in a response and recovery effort under their auspices. However, as with workers' compensation policies, application can be confusing and is often perceived as inconsistent, particularly for personnel who are unclear about whether they are participating as volunteers or employees. The policies also often lack a well-defined disaster recovery timeframe, which should clearly demarcate when liability protections begin and end for volunteers and supplemental personnel.
Finally, self-efficacy and response efficacy were perceived to have a distinct impact on local health department workers' participation in recovery activities. In order to improve levels of self-efficacy, health departments can endeavor to clearly define and communicate emergency-specific roles and responsibilities in advance of a disaster. Response efficacy can be enhanced by communicating to employees the public's benefit from recovery participation and by the assurance of supportive leadership throughout recovery activities. Further research is necessary to quantify the relationship between attitudinal determinants (eg, efficacy) and performance of recovery-related activities, as well as to compare these associations with those made in other phases of the disaster cycle.
Limitations
While the research team endeavored to minimize limitations through study design, generalizability and the introduction of researcher bias are concerns for research that is reliant on the qualitative analysis of data gathered from a relatively small pool of participants. In an effort to increase and test the applicability of the findings, the researchers engaged participants representing a diversity of disaster recovery roles, from a number of different local health departments in geographically and politically distinct jurisdictions. Findings may not be generalizable, as focus groups were limited to 2 geographic clusters. However, the authors believe that the best way to enhance our preparedness for future disasters is to learn from real experiences through the collection and analysis of real data. To mitigate the introduction and influence of researcher bias, the coding procedure was developed iteratively based on emerging themes of significance. In future research of this kind, these limitations could be further addressed through the recruitment of a larger cohort of participant health departments, with even more varied all-hazards recovery experience.
Conclusion
As both the frequency of all-hazards events and the need for recovery services grow, local health departments will find it necessary to cultivate novel, resource-moderate approaches to meet constituent needs and expectations during disaster recovery. Training, safety, family preparedness, policies and planning, and efficacy were all identified as having varying levels of influence on health department workers' perceptions of their willingness and ability to perform recovery activities. By minimizing these as barriers to health department worker participation in the disaster recovery process, local health departments can enable public health providers to better serve their communities in the weeks, months, and years following a disaster.
Footnotes
Acknowledgments
This work was supported by Centers for Disease Control and Prevention Cooperative Agreement 1U01TP000576-01. The funders had no role in decision to publish or manuscript preparation.