
Abstract
We present an analysis of the diagnostic technologies that were used to identify historical outbreaks of Ebola virus disease and consider systematic surveillance strategies that may greatly reduce the peak size of future epidemics. We observe that clinical signs and symptoms alone are often insufficient to recognize index cases of diseases of global concern against the considerable background infectious disease burden that is present throughout the developing world. We propose a simple sampling strategy to enrich in especially dangerous pathogens with a low background for molecular diagnostics by targeting blood-borne pathogens in the healthiest age groups. With existing multiplexed diagnostic technologies, such a system could be combined with existing public health screening and reference laboratory systems for malaria, dengue, and common bacteremia or be used to develop such an infrastructure in less-developed locations. Because the needs for valid samples and accurate recording of patient attributes are aligned with needs for global biosurveillance, local public health needs, and improving patient care, co-development of these capabilities appears to be quite natural, flexible, and extensible as capabilities, technologies, and needs evolve over time. Moreover, implementation of multiplexed diagnostic technologies to enhance fundamental clinical lab capacity will increase public health monitoring and biosurveillance as a natural extension.
The authors present an analysis of the diagnostic technologies used to identify historical outbreaks of Ebola virus disease and consider systematic surveillance strategies that may greatly reduce the peak size of future epidemics. They propose a simple sampling strategy to enrich in especially dangerous pathogens with a low background for molecular diagnostics by targeting bloodborne pathogens in the healthiest age groups. With existing multiplexed diagnostic technologies, such a system could be combined with existing public health screening and reference laboratory systems for malaria, dengue, and common bacteremia or be used to develop such an infrastructure in less-developed locations.
T
Infectious disease surveillance—or, more broadly, biosurveillance—is accomplished by collecting information from diverse data sources that range from traditional syndromic surveillance data collected at hospitals and clinics to information processed from nontraditional data sources such as internet data streams (eg, Twitter, Wikipedia, Google Trends). Margevicius et al have grouped the diverse sources of disease surveillance data into 16 broad categories, one of which is laboratory records, which includes all forms of diagnostics applied to individual samples, whether used in a laboratory setting or at the point of care. 7 This particular data stream is often applied following the first detection of an infectious disease outbreak and therefore has traditionally been a means of confirming the first suspicions of an unfolding outbreak. This is a necessary and credible data stream that forms the cornerstone of any disease surveillance system. To be operationally effective, however, the processes of pathogen detection and diagnosis must be rapid and not require multiple rounds of confirmatory testing. Another key requirement is for the process to generate information that not only identifies the causative agent but also includes characterization (eg, antibiotic resistance). This information allows decision makers to rapidly choose a course of action, such as effective and specific therapeutic and prophylactic treatments. To enhance the use of laboratory records in routine disease surveillance, and perhaps make diagnostic devices the first indicators of a disease outbreak, real-time diagnostic data feeds to global surveillance systems would be a bonus.
Recent, but pre-Ebola, efforts by nongovernmental organizations to address the disease surveillance problem by Connecting Organizations for Regional Disease Surveillance (CORDS) are reviewed by Bond and colleagues. 8 An extensive statistical model of global morbidity, mortality, and associated risk factors has been compiled and made accessible through a variety of web-based visualization tools at the Institute for Health Metrics.9,10 Subsequent to the West African Ebola outbreak, an international commission was established to guide the development of a global architecture. Called the Global Health Risk Framework, its aim is to mitigate the threat of large outbreaks of infectious disease. This commission will examine the various elements needed to build a robust framework for effective response that includes surveillance, health information systems, and health systems infrastructure, among others, and to develop evidence-based guidance for world leaders to develop robust response systems. 6 The US government has published a national strategy for biosurveillance 11 and combating antibiotic resistance 12 and has called for linking diagnostic systems to digital health surveillance systems.
In this article, we examined the potential for integrating multiplex diagnostics into routine infectious disease surveillance through incorporation in clinical diagnostic workflows as a means of cost-effective, timely detection of emerging diseases and as a means of improving the effectiveness of surveillance systems. Multiplexing can be defined generally as the ability to ask more than one question about a sample at the same time (multiple markers per sample), or the ability to conduct more than one test on or test for multiple targets in a sample in the same reaction volume. In the context of infectious disease diagnostics, this means enabling an assay to screen samples for more than one pathogen, facilitating the “rule in” approach to diagnostics and supporting early detection of an outbreak. 13 An additional benefit to employing multiplexed diagnostics is enabling detection of multiple pathogens (co-infections) in an individual host or even host response biomarkers that inform about individual disease progression.
We performed 2 studies to inform our conclusions: The first one focused on detailed analysis of historic Ebola outbreaks to identify challenges associated with the diagnosis and declaration of EVD outbreaks, and to identify the opportunities for early detection using point-of-care, multiplexed diagnostics on both the individual and population scales. We then looked more broadly across 4 recent epidemics in different areas of the globe—Ebola in West Africa, dengue in Southeast Asia, chikungunya in Latin America, and MERS in the Middle East—to understand common themes in emerging disease surveillance. Second, we analyzed the economics and utility of a specific surveillance architecture using multiplexed diagnostics, considering the likelihood of it detecting emerging infectious disease against the background of infectious disease deaths in each region of the globe. For example, multiplex tests that include both EVD and other diseases with similar symptoms (eg, gastrointestinal) that are known to cause illness in a specific region would help to delineate individuals who actually had EVD from those who were being unnecessarily treated during an EVD outbreak, thereby conserving the limited stocks of therapeutics for EVD.
Methods and Results
Historic Outbreak Analysis for EVD
A total of 27 EVD outbreaks (including the recent West African outbreak) were analyzed to understand EVD progression, its differential diagnosis, durations from the time the index case(s) was discovered to the confirmation of the occurrence of EVD, and control measures implemented. The epidemiology of each outbreak was analyzed to understand the causes of reporting delays and even misreporting (eg, low index of suspicion, concomitant outbreaks of other diseases with similar early symptoms like cholera or typhoid, etc). Finally, detection techniques used for each outbreak were identified and the processes by which EVD outbreaks were declared were compared. Supplement 1 shows the details of the information collected for outbreak comparisons (see Supplement online at http://online.liebertpub.com/toc/hs/14/3).
Figure 1 shows the various stages of EVD progression and a representative timeline, which was built using specific case histories from the recent 2014 series of EVD cases treated in the United States.14-16 This analysis enabled us to understand disease progression at the individual level and the cause for misdiagnoses that were documented to have occurred during some of the historical EVD outbreaks discussed in Table 1. Because of the generic nature of symptoms of EVD in the initial stages, a primary challenge is distinguishing EVD from other diseases such as cholera or malaria. Table 1 lists 10 diseases that EVD was mistaken for in at least 1 of the 27 historic outbreaks, and while all of them require supportive care, EVD-specific treatment was almost always delayed in these cases, leading to continued spread in the population. The table also shows the various tests and sample types that are commonly employed for the diagnosis of these diseases.
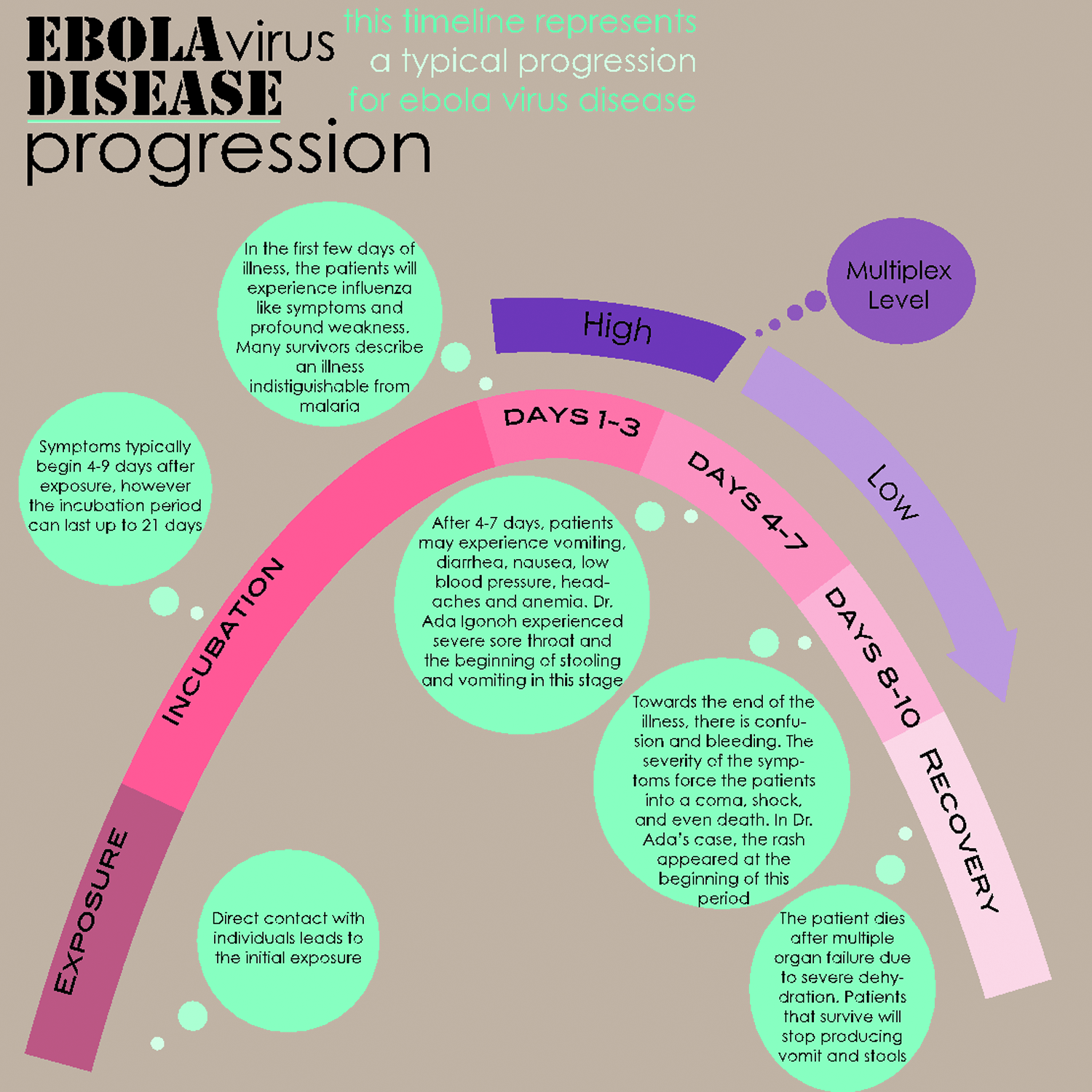
EVD Disease Progression
Diseases That EVD Was Mistakenly Diagnosed for in at Least 1 of the 27 Historic Outbreaks of EVD
BSL = Biosafety level
For individual diagnosis, it is possible to develop multiplex panels that could screen the appropriate sample type for an EVD and its commonly mistaken diagnoses. The level of multiplex could also be tailored based on specificity of symptoms as seen in the disease progression time line in Figure 1. For implementation in a regional routine surveillance program, such multiplex tests could also be designed to encompass prevalent diseases in the region, thereby allowing the characterization of emerging diseases. EVD has been diagnosed with a wide variety of techniques, ranging from clinical progression 1 to characterization by whole-genome sequencing. 27 As multiplex diagnostics could be implemented for both outbreak surveillance and characterization of emerging threats during routine surveillance, different types of assays could be used at point-of-care settings in combination with clinical observation (eg, lateral flow antigen/antibody detection) or in a laboratory setting that performs higher resolution characterizations (eg, multiplex PCR). Point-of-care settings offer a much earlier time point in outbreak detection, and therefore lateral flow multiplex assays that perform rapid screening could be considered for implementation. Moreover, when one considers other factors, such as the cost per sample, biosafety levels required for sample preparation, complexity of equipment, infrastructure needed, complexity of sample tracking, and level of training required to conduct tests, the types of multiplex assays that merit greater consideration are non–nucleic acid biomarker assays such as the standard antigen/antibody assays.
The time to diagnose EVD for historic outbreaks in which a mistaken disease identity occurred was compared to the outbreaks in which EVD was the only diagnosis. We collected the following pieces of data for each EVD outbreak from the publicly available literature (this list is not exhaustive):
• Mistaken for another disease: This included any outbreak where original reports, or literature regarding the outbreak, specifically mentioned mistaking the outbreak for a different disease. We also included outbreaks in which other diseases were suspected and treated for prior to testing for EVD. We did not include outbreaks whose initial cases were labeled as “general viral hemorrhagic fever.” We categorized this both as a descriptive free text variable as well as in a binary fashion, for outbreak comparisons noted below. • Time to diagnosis (days): The number of days from the first mention of illness onset (ie, index case's symptom onset date) until laboratory confirmation of EVD. • Time to control measures (days): The number of days from the first mention of illness onset (ie, index case's symptom onset date) until date of first control measure implemented, as described in the literature. We did not distinguish between types of control measures (eg, quarantine vs barrier nursing) but rather used the earliest date for this calculation. The objective was to measure the shortest block of time between outbreak onset and the time when actionable events were documented.
We then compared outbreaks with mistaken disease identity to those without mistaken disease identity by looking at the relative time to diagnosis in each group (Figure 2a). A statistically significant difference (p < 0.05) was seen in the time to diagnose EVD between the 2 categories of outbreaks based on the Student's t-test, indicating that mistaken disease identity contributed to the delayed detection and therefore delayed control measure implementation. To further explore the relationship between time to diagnosis and time to control measure implementation, we analyzed a simple linear regression model between the 2 variables (Figure 2b). We see a strong correlation between them (R2 = 0.89), further indicating the value of accurate and early diagnosis. Had multiplexed or even parallel reaction diagnostic platforms been in place, a whole panel of diseases could have been tested for whenever a routine infectious disease test was ordered, thereby allowing for emerging diseases to be detected earlier, assuming that diagnostic results were indeed provided to the proper surveillance systems.
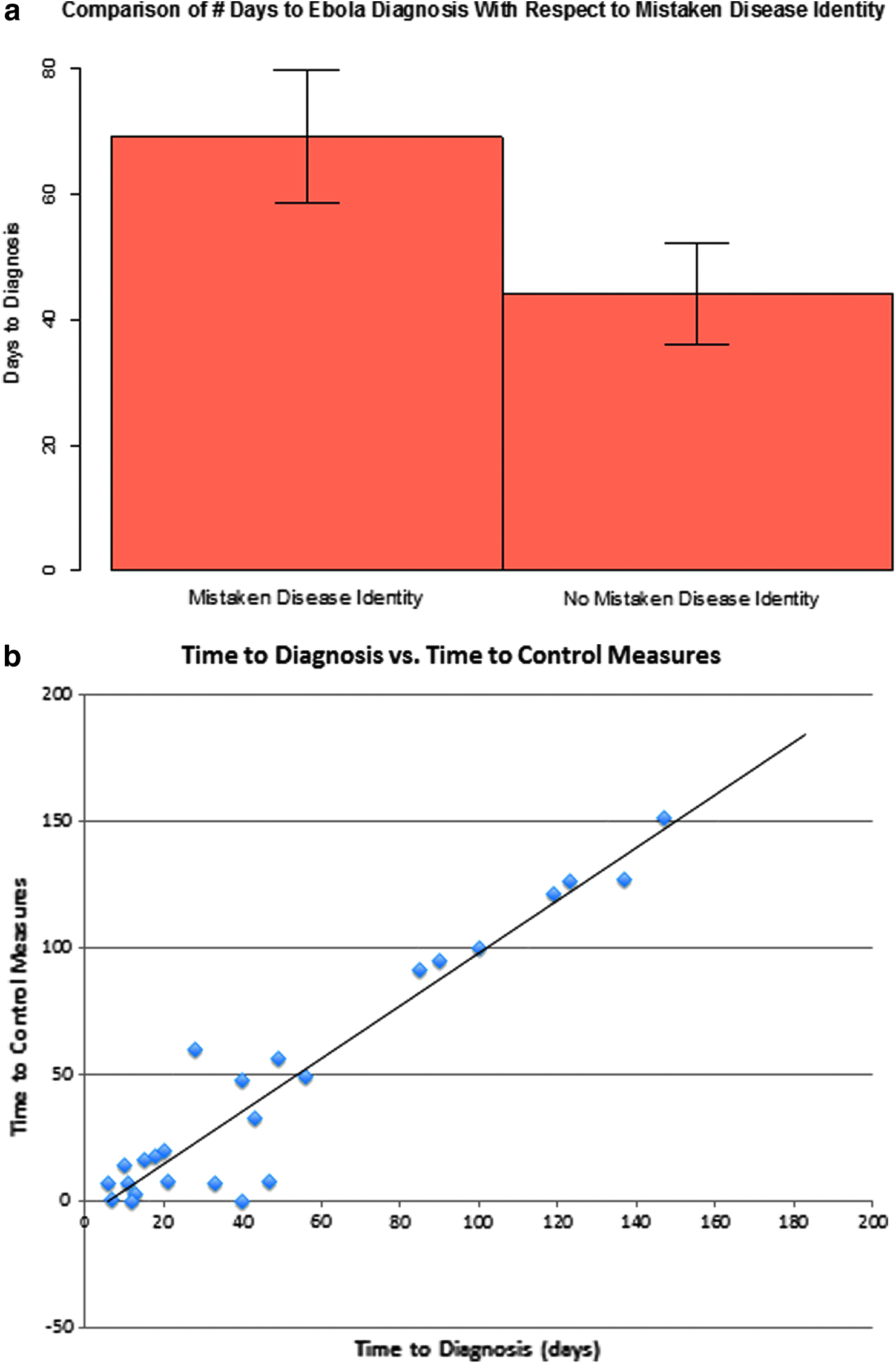
(a) Comparison of time to diagnose EVD in historic outbreaks with initial mistaken disease identity versus historic outbreaks with singular EVD diagnosis. Groups were compared using arithmetic means and Student's t-tests to determine if the average time to diagnosis was statistically different based on mistaken disease identity status. Bars show the arithmetic mean of the group and error bars represent 95% confidence intervals. (b) Correlation between time to implementation of control measures and time to diagnosis of EVD (R2 = 0.8911) examined using linear regression.
Generalization to Other Disease Outbreaks
While the EVD outbreak has focused the world's attention unlike any other recent outbreak, development of a surveillance system requires consideration of generality, which we explored by considering 3 other outbreaks that have recently caused significant morbidity and mortality and have been addressed with modern diagnostic tools. We researched these outbreaks to understand how they were detected, what the causes of delayed diagnosis were, and what diagnostic tools were used during the outbreak to first identify and then confirm cases of the disease. The goal was to determine if the conclusions arrived at through analysis of historical EVD outbreaks were generalizable across other infectious diseases and therefore could be used to make recommendations about the use of multiplex diagnostics in an infectious disease surveillance system.
Examination of single outbreaks for these diseases revealed very similar challenges in early detection to the analysis performed on multiple EVD outbreaks described in the earlier study. As further support for our conclusions, a recent article showed a background prevalence of a number of arthropod-borne and hemorrhagic fever viruses in samples submitted to the Lassa Diagnostic Laboratory in Sierra Leone during 2006-2008 when tested serologically. 32 Sierra Leone is hyperendemic for Lassa, and therefore most individuals are first tested for Lassa fever virus. However, this study demonstrated that other diseases can appear at a background level in a given outbreak. This underscores the value of implementing multiplex diagnostics for screening samples both during an outbreak of undiagnosed illness and in routine surveillance.
Both studies indicate a strong utility for multiplex diagnostics, especially blood-based, low-plex (3-5) assays that will enable detection of likely emerging pathogens as well as the most common local concerns. As mentioned before, when taking into account various operational considerations, simpler, low-plex assays might currently be more practical to use even though large multiplex panels may be available. Additionally, regional customization of multiplex panels should be considered, because one size or level to type of multiplex would not be practical for all testing. The local prevalence of diseases, population susceptibility, and environmental factors would all be needed to inform multiplex panel design.
Healthcare Spending and Disease Burden
Many of the countries where infectious diseases emerge are relatively poor, and one should ask how the expense of a disease surveillance program compares to incomes, healthcare spending, and other healthcare needs. In Table 2, we provide an overview of per capita healthcare metrics for representative countries in which the 4 outbreaks we considered were emerging. Unless we plan to create an infrastructure comparable in size to national healthcare delivery systems, it is evident that sampling of well-chosen subsets of the population will be essential. Insofar as a disease surveillance system represents a significant proportion of a healthcare budget, it should also be designed to provide substantial and enduring value to the population being surveyed—perhaps comparable to improving water, sanitation, or nutrition.
Overview of Healthcare Spending, Incomes, and Healthcare Needs for 8 Countries, from WHO Summary Sheets
To understand the magnitude of the burden of infectious disease, as well as the level to which it is currently classified through symptoms, we examine data from 2 regions, sub-Saharan West Africa and North Africa and the Middle East (Figures 3a and 3b). All-cause mortality with risk factors, age structure, and historical changes are available by country from the Institute for Health Metrics. 9 From this source, we see that infectious disease is still the primary cause of mortality in western sub-Saharan Africa, even for 15- to 49-year-olds.
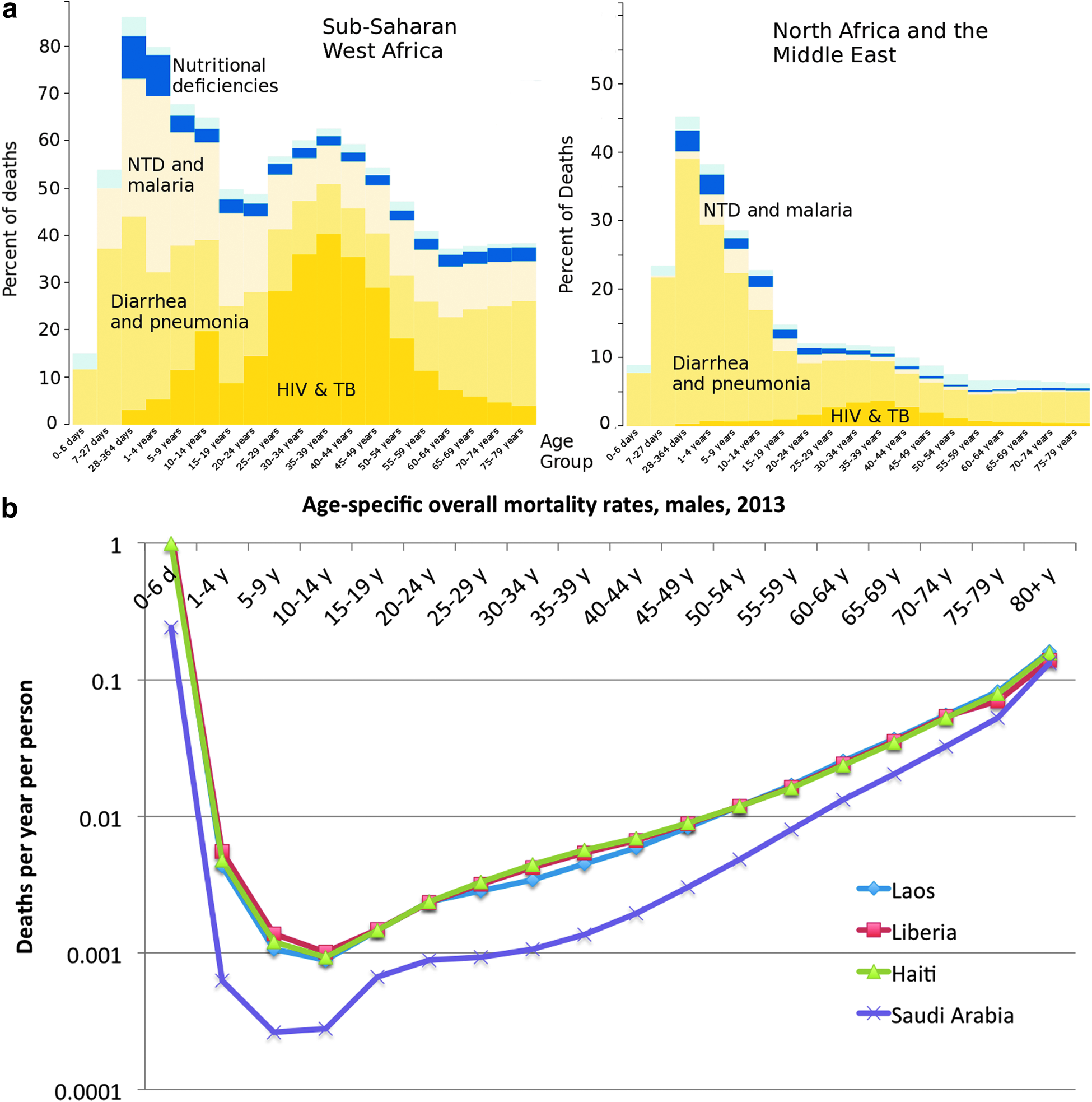
(a) Age dependency of infectious disease deaths in sub-Saharan West Africa and North Africa by cause, from reference 9. NTD = Neglected tropical diseases; TB = tuberculosis. (b) All-cause mortality rates, from reference 9, for Laos, Liberia, Haiti, and Saudi Arabia.
The data in Figure 3a show that infectious disease deaths can be classified into 3 main groups: HIV+tuberculosis, neglected tropical diseases and malaria, and diarrhea and pneumonia, reflecting the limitations of clinical diagnosis from which such global data must derive. From the types of misdiagnosis of EVD provided in Table 1, it appears likely that a diagnostic tool stream will need to include the categories “NTD [neglected tropical diseases] and malaria” and “diarrhea and pneumonia,” thus encompassing approximately half of all infectious deaths. A multiplex diagnostic could easily incorporate panels that cover these groups. In fact, several multiplex diagnostics exist today that could cover these groups, and some of these devices are already CLIA waived and approved for point-of-care use.
It is also evident, however, that there is a strong characteristic age-dependency of infectious disease deaths, which we show for West Africa, where HIV is highly prevalent, and North Africa and the Middle East, where much lower levels of HIV are reported. This suggests that an age-specific surveillance of infectious disease could create a sample stream that is substantially enriched in diseases of particular virulence.
Figure 3b shows infectious diseases as a percentage of deaths in each age category and the overall age-specific mortality rate for 4 countries of interest, so that one can quantify the magnitude of possible infectious disease surveillance systems. Not only do 15- to 24-year-olds show a minimum in the fraction of deaths resulting from infectious disease, but they also have much lower all-cause mortality rates than any other age group.
Surveillance Architecture
A significant cost of any disease system will include the infrastructure, training, and validation and the information management system and experience required to appropriately act on the data stream. An extensive consideration of political and economic realities is essential to the success of biosurveillance systems and was identified as a part of the Rockefeller Foundation initiative promoting regional surveillance networks.8,39 Descriptions, lessons learned, and suggestions of paths forward were provided by the Mekong Basin Disease Surveillance Network, 40 the East African Integrated Disease Surveillance Network, 41 the South-Eastern European Health Network, 42 the Middle East Consortium on Infectious Disease Surveillance, 43 the Asian Partnership on Emerging Infectious Diseases Research, 44 the Southern African Centre for Infectious Disease Surveillance, 45 and the REASAOLAB project involving clinical laboratories in West Africa. 46 One consistent issue with all of these efforts is how to sustain the long-term activity and continuity in training and interactions that is so crucial to the productivity and trust necessary for crisis response. Operationally, including the multiplex Dx platform in clinical settings to identify common diseases as well as potentially emerging diseases could be one contributing solution.
To understand this, we reviewed a variety of existing government-funded programs aimed at biosurveillance at the scale we envision: the Health and Demographic Surveillance System (HDSS) in Kisumu, Kenya; 47 the reporting system of the Pan American Health Organization (PAHO); and efforts of the US Department of Defense, such as Walter Reed, the GEIS program of the Armed Forces Health Surveillance Center (AFHSC) system, the NAMRU/USAMRU-K system, the sentinel laboratory system of the US CDC, and the infectious disease surveillance systems funded for the purposes of infectious disease research. Additionally, the WHO regularly produces standard of care documents for best practices of medicine in resource-limited regions of the globe.
As observed previously, 1 systematic surveillance of infectious diseases using multiplexed diagnostics could, if done properly, provide significant value in both characterizing the circulation of common pathogens for the benefit of patient care and rapidly identifying comparatively rare emerging outbreaks of concern. For inclusion of multiplex diagnostics into a surveillance system, it is important to consider both design of the multiplex panel and a sampling strategy. These 2 elements are what would make adoption of multiplex point-of-care diagnostics attractive in developing nations and regions that are sources for many emerging diseases. Many of these expenses are fixed costs and will need to leverage existing efforts in any sustainable system. This also effectively defines a minimum practical throughput of the system in terms of samples per day.
A diagnostic tool with everyday applicability, coupled with the ability to screen for emerging infectious diseases, could be more easily included in a surveillance system than a tool that was expressly designed to detect only emerging diseases and therefore would see use only upon suspicion of that disease occurring. Multiplex diagnostics enable this to happen. To make multiplex diagnostics even more adoptable, probe panels that represent the commonly occurring diseases in a specific region can be designed to allow the detection of multiple disease outbreaks if they are occurring at the same time. This was illustrated in many of the historical EVD outbreak case studies in which EVD occurred at the same time as a cholera or measles outbreak. Additionally, use of a properly randomized sampling architecture would enable statistically controlled assessment of the temporal and geographic trends in disease burden of the common pathogens, which could be of great value in assessing control measures. This becomes important if multiplex diagnostics were to be considered part of a routine surveillance program to gather information about the prevalence of region-specific infectious diseases to plan for prophylactic and therapeutic stockpiles. Such a use of multiplex diagnostics would further make them useful in a surveillance system.
Examination of Table 2, however, suggests that it is unrealistic to administer multiplexed diagnostics to a significant portion of bouts of infectious disease in a developing country, as one would naively need to do in order to identify a disease outbreak without prior specific suspicion. Without such an ability, the international community would have less incentive to fund the significant infrastructure to maintain such a system. A nonrandom sampling strategy, however, can greatly decrease the number of samples that need to be measured while only modestly decreasing the likelihood of identifying an unanticipated disease outbreak. Such a system would also provide significant benefit to the patients whose blood is assayed. We suggest that this outbreak identification ability would be cost-effective for the international community, simply by reducing the risk of another infectious disease outbreak of international concern. Once established, such a system could be expanded with local investments in whatever manner seems most cost-effective to local populations.
It is possible to estimate the necessary capacity of such an age-specific infectious disease surveillance system that would have a well-defined and significant chance of identifying outbreaks not already suspected by clinicians, yet reasonably be completed in a modest-sized laboratory. The annual rate of age-specific all-cause mortality reaches a minimum of ∼0.0018 per person-year in Liberia in the age range of 15 to 24. Starting with a population of 1 million, of whom 15% will be between 15 and 24 years of age, we see from Figure 3 that 40% of the deaths in this age group, or 108 deaths per year, will occur in West Africa. The corresponding value for Saudi Arabia, with its annual all-cause mortality rate among 15- to 24-year-olds of 0.0008, with 10% of these caused by infectious diseases, is 12 deaths per year.
Any surveillance system that is going to provide patient benefit (to improve sustainability) must diagnose sick patients as well as dead; we estimate that an age-specific emerging disease surveillance could be designed with a case definition that captures approximately 10 times as many samples as there are deaths, and reports back the results of multiplexed diagnostic tests soon enough to affect patient care.
The age-specific nature of such a system means that it will have at most only a 15% chance of identifying the index case within our surveillance age window for an unexpected pathogen in the multiplexed diagnostic panel. On the other hand, such a system would only need to process ∼4,000 samples per year in a country like Liberia, with 4 million people and a relatively high disease burden and mortality rate. Countries with an infectious disease mortality rate like Saudi Arabia would require a sampling rate that is 10 or 100 times lower and could consequently survey for a larger number of pathogens. The abovementioned rate of sampling is well within the reach of a program comparable to existing efforts in many developing nations, if assays can provide reasonable utility to the people being surveyed (multiplexed) and reagent costs can be reduced to a few dollars per assay.
Investors in multiplex point-of-care diagnostics development can easily define requirements for costs such that their use can become widely accepted. Following the EVD crisis, significant infrastructure has already been established in countries like Liberia for both disease surveillance and reporting,48,49 and implementation of a surveillance system using multiplex diagnostics that screen for EVD and region-specific diseases for ∼4,000 samples a year seems completely reasonable. Liberia already has mobile labs established by CDC, 50 and the US Army Medical Research Institute of Infectious Diseases (USAMRIID) has developed a new genomics laboratory at the Liberian Institute for Biomedical Research that will be “supporting surveillance projects across the country to investigate reservoir animals and insect vectors of disease to identify potential threats. In addition, the center will support ongoing assessment of samples from patients with severe diseases of unknown origin, providing a key public health asset to West Africa.” 51 A reasonable sampling plan and well-designed multiplex assays would further the investments that have already been made in infrastructure for robust disease surveillance in Liberia. A multiplex system inserted into the workflow of a clinical laboratory could provide the necessary sampling capacity while also providing clinical benefit.
While this is a very specific example, and we provide only the roughest sketch suggesting its cost-effectiveness and utility, the core idea of identifying virulent pathogens by preferentially sampling the healthiest people is broadly applicable and can be easily modified to a variety of background disease burdens or surveillance architectures that exist across the developing world.
Conclusion
To summarize, this article demonstrates the practicality and utility of using multiplex assays at point-of-care settings as part of routine surveillance for infectious diseases or during outbreak monitoring. For most effective use of this tool as part of an infectious disease surveillance system in developing nations, it will be important to consider both diagnostic panel design and sampling strategy. This will drive down the costs of implementing multiplex diagnostics use. While performance characteristics of multiplex diagnostics were not discussed here, they are equally important for selecting the most appropriate tool for use in a surveillance system. Technology has improved to the point where multiple stakeholders can contribute to and benefit from high-throughput characterization of infectious disease samples.
Footnotes
Acknowledgments
This work was supported by an Interagency Agreement with the Department of Homeland Security (HSHQPM-14-X-00069).