
Abstract
Rapid development and advancement of bioresearch at a university's laboratories can have both positive and negative implications for public health and the environment. Many research activities in which biological materials have been created, modified, stored, and manipulated require safety procedures to keep the negative effects on humans and the environment as low as possible. The Occupational Health, Safety and Environmental (OHS&E) Department of the University of Indonesia (UI) is trying to increase the awareness and responsibility of its university members and laboratory staffs who work with biohazard materials by creating a biorisk checklist. The checklist was developed based on WHO guidelines and the National University of Singapore (NUS) Laboratory Manual, which contains 311 questions about the management, administration, and handling of various hazards, recombinant experiments, and animal and plant experiments. A gap analysis was run against the checklist in 14 laboratories at the University of Indonesia Salemba campus, which daily works with highly infectious pathogens and high-risk agents. Overall result showed that none of these laboratories had met all of the checklist items, and there were only 2 laboratories that had implemented more than half of the items. This checklist was proven to be a simple tool for assessing laboratories that handle and store biohazard materials, and it could be used as a monitoring tool for biorisk programs as well. It also could be further developed as a laboratory software application to increase its effectiveness and its accuracy.
Universitas Indonesia is trying to increase awareness and responsibility of its university members and laboratory staffs who work with biohazard materials by creating a biorisk checklist, based on WHO guidelines. A gap analysis was run against the checklist in 14 laboratories at one campus that works with highly infectious pathogens and highrisk agents. Overall results showed that none of these laboratories had met all of the checklist items, and there were only 2 laboratories that had implemented more than half of the items.
B
Research has showed that only a small number of incidences of infection associated with microbiology teaching laboratories have been reported. 4 However, a significant case was revealed by the Centers for Disease Control and Prevention (CDC) that showed that 109 individuals had been infected by a strain used in clinical and teaching laboratories, which led to 12 hospitalizations and 1 death. 5 This might indicate that exposure to bio-infections were more common than had been reported. The underreporting of laboratory-acquired infections has been widely acknowledged and has been ascribed to the negative consequences that would result for reporting companies or authorities. 6 In addition, several reports of laboratory-acquired infections related to traditional laboratories that have been published in recent years bear this out.7,8 A study of laboratory-associated infections in Indonesia conducted by the National Institute of Health Research and Development in 2011 indicated a similar condition. 9 It was reported that 13.5% of needlestick accidents and 10.5% of infectious spills occurred in 770 healthcare laboratories operated by the ministry of health, but no laboratory-acquired infections were reported. 9 As a response to this potential biohazard, a lab management program was introduced by the UI Occupational Health & Safety Department in 2011 as part of a multiyear program of biorisk management.
One of the important elements of this program was to prepare a manual of good laboratory practices and standard operating procedures (SOPs) for biorisk management. This manual has been developed using the WHO Laboratory Biosafety Manual and the National University of Singapore (NUS) Biorisk Management Manual.1,10 Although this information had been made available to university personnel, it had been only partially implemented because of its recent introduction. The NUS Biorisk Management Manual describes in detail biorisk assessment and management of various bioagents such as plants, toxins, genetically modified organisms, and recombinant experiments, as well as training and an occupational health program. As in the WHO manual, NUS's manual also describes biosafety levels, lab animal safety, guidelines for lab commissioning and certification, biological safety cabinets and other engineering controls, and biosecurity.1,10 A series of questions were developed based on the WHO and NUS manuals to help in assessing laboratory biosafety at the UI Salemba campus.
Material and Methods
There are 50 laboratories belonging to the Medical Science and Dental Faculties at the Salemba campus, some of which are connected to major hospitals in the Jakarta region. Of these, 38 laboratories were taken as a base from which to select the samples because they work daily with biological materials. Of the 38 laboratories, 14 were selected for this article because of their frequent interactions with highly infectious pathogens and their readiness to be assessed; BSL-2 and BSL-3 laboratories were specifically selected. These laboratories were then examined using 311 questions that were developed to respond to 15 elements of the biorisk checklist (see Table 1). The responses to the questions were limited to yes, no, and N/A and were assigned values of 1, –1, and 0, respectively. Implementation scores and gap analysis were calculated based on the following formula:
Biorisk Checklist
The highest implementation score is 100%. Gap analysis equals the number of absences of implementation over 311 questions stated in the checklist.
Results
Overall results showed that only 2 laboratories obtained an implementation score greater than 50%. This may be because these laboratories were BSL-2+ and BSL-3 labs and thus there was a higher awareness among the staffs working at those facilities compared to other lower-level facilities; in addition, biosafety training had been conducted when these laboratories were established. As noted by Higgins et al, personnel awareness relies on the implementation of biorisk programs in the laboratory. 11 Biomaterials must be handled safely and securely in all settings where they are contained and kept separated from a noncontainment environment (biocontainment). Biosafety levels in high-resource laboratory settings are classified into 4 levels, 1 to 4, in order to ensure the safety of laboratory personnel and the environment, 12 so it makes sense that facilities having a higher level of biosafety would obtain a better score in this study.
Table 2 and Figure 1 show the score of effectiveness in the implementation of biorisk management, and Table 3 shows the gap in biorisk implementation in each laboratory. The widest gap found in this study is related to a lack of good microbiological techniques and recommended work practices, followed by lack of emergency response on exposure to potential infectious materials. Better microbiological techniques and work practices could be achieved by establishing a good lab practice manual, followed by continuous training to increase discipline and safety awareness among lab workers. Emergency response is more difficult to be implemented, as it may need support from other parties such as university security services, hospital workers, firefighters, police, and the like.
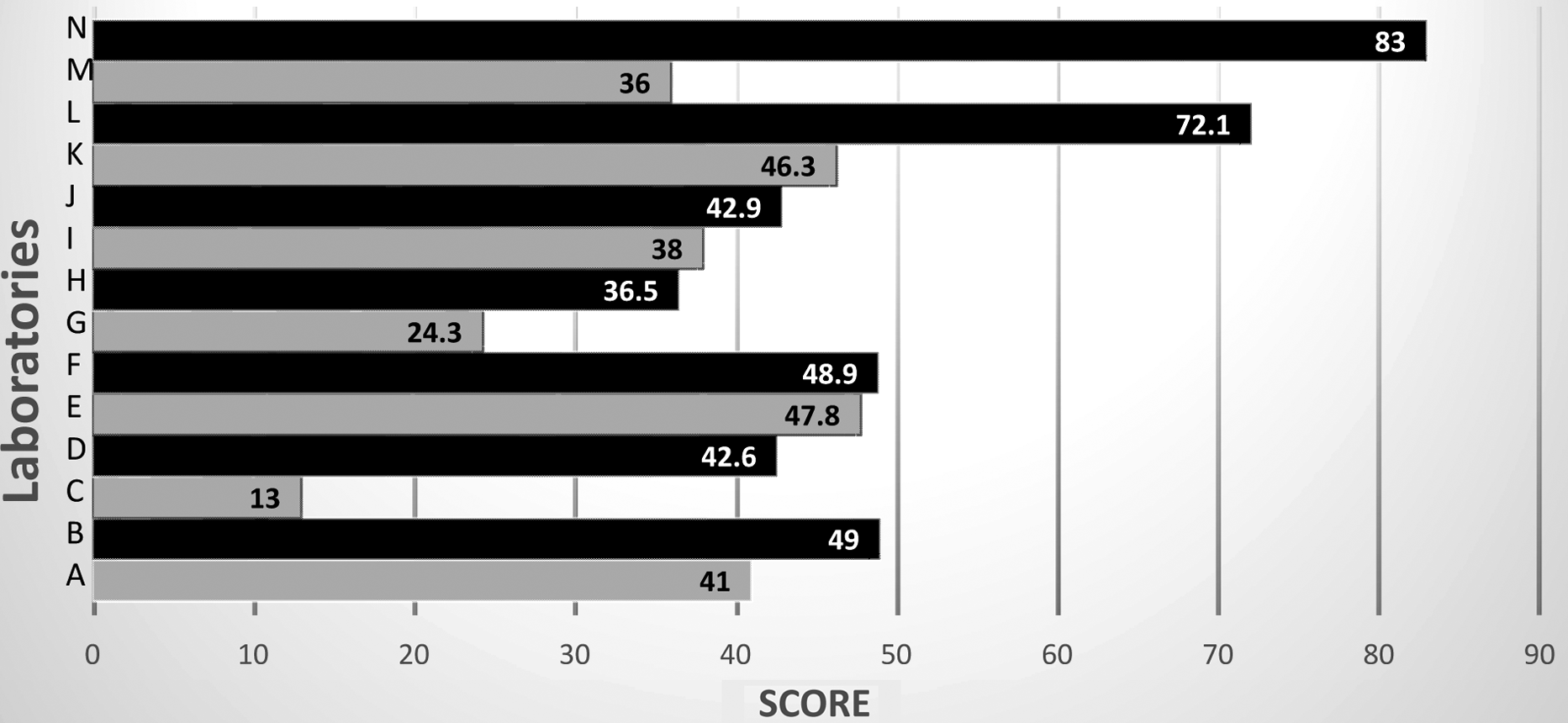
Score of Biorisk Management Implementation
Score of Biorisk Management Implementation in Laboratories in Health Science Area
Gap Analysis of Each Laboratory
Note. Gray area = the 3 maximum gap analysis in each laboratory.
The top 3 implementation scores in this inspection were laboratory animal and plant facilities, biosafety and recombinant DNA technology, and personal protective equipment. But we should be careful in the interpretation of the categories of biosafety and recombinant DNA technology and laboratory animal and plant facilities, because the scores may reflect the absence of this facility and technology in the lab inspected. Only the use of personal protective equipment may be considered but should be analyzed further concerning its suitability and sufficiency (see Table 3).
In addition, it was noted during the analysis of results that there were 2 laboratories that belong to the dentistry faculty that had low scores because biological agents were not found. During the preliminary sample selection process, these 2 laboratories were thought to work with biological materials, but it was found that they work only with nonbio material, such as dental implant materials. Thus, they were irrelevant to this study. This finding could be used as an exclusion criterion when developing this checklist further.
Discussion
Working with biological specimens, such as human tissues, bones, and fluids, and with various microorganisms such as parasites and viruses are routine activities in health sciences and educational fields. The potential risk of being infected while working in a laboratory exists and may be inevitable. There is the possibility for students, lecturers, and laboratory workers to be exposed to various biological threats, because it is estimated that a human body, on average, contains 10 times as many bacterial cells as human cells13,14 and at least 10 times as many viral genomes as bacterial genomes.15,16 Were those agents to be released from the laboratories, they would be a major threat to public health and safety.
Furthermore, current biotechnology used in developing new vaccines, diagnostic tools, and therapeutic agents, and microorganism manipulation using genetic engineering techniques, could also pose new concerns of risk in the biological field. 17 Biotechnology laboratories need good biosafety measures designed to protect their staffs, the surrounding population, and the environment from hazardous organisms and materials. Continuous training and education are essential, not only to acquire a good understanding about the direct handling of biohazardous agents but also to gain knowledge of the epidemiology, pathogenicity, and human susceptibility of the biological materials used in research.
Biological risk can be reduced and controlled by correct application of internationally recognized procedures, such as proper microbiological techniques, proper containment apparatus, adequate facilities, protective barriers, and training and education of laboratory workers. The standardized microbiological techniques and the use of containment devices, facilities, and protective barriers are necessary.17-19
The current common practice of the “western standard” for ensuring the safe and secure handling of pathogenic agents is mainly focused on installing complex and costly containment units in emergency outbreak areas or areas with a continuing high rate of disease. This practice has not always been effective or sustainable, as it required large amount of investment, adequate and continuous access to resources, and educated personnel.20-22 This is an important point to be emphasized at universities in developing countries, where the government may not make biorisk management issues their top investment priority. For the same reason, the UI Occupational Health & Safety department had tried and been successful in 2015 in obtaining a commitment from the university's board, titled the Implementation of Occupational Safety Health and Environment Program at Universitas Indonesia. Despite all efforts since 2011, this program has not been very successful among faculty members and laboratory staffs. Some of them did not even know of the program's existence. Thus, the department is now developing compulsory online training for all staff and students to participate in prior to working in a laboratory.
Indonesia has also recently established a National Standard for Biorisk Management based on CWA 15793, which could be improved by implementing a Plan-Do-Check-Act (PDCA) cycle 23 as well as further development of the biorisk checklist. This program could be developed further over a larger area, such as all Southeast Asian countries, to harmonize laboratory standards in this area.
In addition, support from university members and the Indonesian government is needed to ensure biomaterials are being handled properly. These include infrastructure upgrades, continuous personnel training, and good laboratory policy and practices, which could be further enforced by Indonesian laws.
This checklist can be developed further as a software application, which has started to provide a practical and efficient tool to assess and monitor the implementation of biorisk management in the laboratory, and checklist analysis could be done faster and more accurately.
Conclusion
Using this checklist, the gap analysis showed that the major points of weakness are good microbiological techniques, recommended work practices, and emergency response to exposure to potentially infectious materials; these are very important in the implementation of biorisk management and are not difficult to implement because they are not costly but do require continuous training, manuals, and an increased awareness among lab workers.
This checklist has been proven to be a simple tool to assess laboratories that handle and store biohazard materials, and it can be used as a monitoring tools of biorisk programs. Further development as a laboratory software application could increase its effectiveness and its accuracy.
Footnotes
This publication is based on work supported by a grant from the US Department of State's Biosecurity Engagement Program (BEP). The opinions, findings, conclusions, or recommendations expressed in this material are those of the authors and do not reflect the views of BEP. We would like to thank the National University of Singapore Occupational Safety Health and Environment team who fully supported us in developing Biorisk Management System. We would like to thank Hendri Bundrawan for manuscript preparation, English correction, and editing.