
Abstract
Super Bowl XLIX took place on February 1, 2015, in Glendale, Arizona. In preparation for this event and associated activities, the Maricopa County Department of Public Health (MCDPH) developed methods for enhanced surveillance, situational awareness, and early detection of public health emergencies. Surveillance strategies implemented from January 22 to February 6, 2015, included enhanced surveillance alerts; animal disease surveillance; review of NFL clinic visits; syndromic surveillance for emergency room visits, urgent care facilities, and hotels; real-time onsite syndromic surveillance; all-hazards mortality surveillance; emergency medical services surveillance, review of poison control center reports; media surveillance; and aberration detection algorithms for notifiable diseases. Surveillance results included increased influenzalike illness activity reported from urgent care centers and a few influenza cases reported in the NFL clinic. A cyanide single event exposure was investigated and determined not to be a public health threat. Real-time field syndromic surveillance documented minor injuries at all events and sporadic cases of gastrointestinal and neurological (mostly headaches) disease. Animal surveillance reports included a cat suspected of carrying plague and tularemia and an investigation of highly pathogenic avian influenza in a backyard chicken flock. Laboratory results in both instances were negative. Aberration detection and syndromic surveillance detected an increase in measles reports associated with a Disneyland exposure, and syndromic surveillance was used successfully during this investigation. Coordinated enhanced epidemiologic surveillance during Super Bowl XLIX increased the response capacity and preparedness of MCDPH to make informed decisions and take public health actions in a timely manner during these mass gathering events.
In preparation for Super Bowl XLIX in Glendale, Arizona, and associated activities, the Maricopa County Department of Public Health developed methods for enhanced surveillance, situational awareness, and early detection of public health emergencies. Surveillance strategies implemented included enhanced surveillance alerts; animal disease surveillance; review of NFL clinic visits; syndromic surveillance for emergency room visits, urgent care facilities, and hotels; real-time field syndromic surveillance; all-hazards mortality surveillance; emergency medical services surveillance; review of poison control center reports; media surveillance; and aberration detection algorithms for notifiable diseases.
A
Super Bowl XLIX took place on February 1, 2015, at the University of Phoenix stadium in Glendale, Arizona. In preparation for this large-scale public event and related activities in Maricopa County, the Maricopa County Department of Public Health (MCDPH), in close collaboration with other local, state, and federal agencies, developed and implemented methods for enhanced epidemiologic surveillance, situational awareness, and early detection of public health emergencies.
In this article, we describe the enhanced epidemiologic surveillance efforts in place during Super Bowl XLIX and related events, review epidemiologic surveillance results, discuss novel approaches for near real-time surveillance for situational awareness and early event detection, and examine lessons learned for surveillance strategies during mass gatherings.
Methods
From July 2014 to January 2015, a Public Health and Medical Resource Work Group (one of 24 resource work groups) and an Epidemiology Work Group met monthly to develop and coordinate epidemiologic surveillance strategies and other public health considerations with more than 60 local, state, and federal partners (Table 1). During this planning phase, meetings were coordinated with groups from New Jersey, Louisiana, North Carolina, and Las Vegas to gather surveillance methodology recommendations from state and local jurisdictions that had previous experience with epidemiologic surveillance for mass gatherings. The surveillance strategies outlined in Table 1 were developed to monitor levels of disease activity and provide situational awareness to partners in Maricopa County from January 22, 2015, to February 6, 2015, with focus on the following high-profile events: Pro Bowl (January 25, 2015, Glendale, AZ); NFL (National Football League) Experience (January 24, 2015, through February 1, 2015, Phoenix Convention Center, AZ) and Super Bowl Central (January 24, 2015, through February 1, 2015, Phoenix, AZ); the Waste Management Phoenix Open and other activities associated with the Super Bowl in Scottsdale, AZ; and Super Bowl XLIX. The Fiesta Bowl (December 31, 2014, Glendale, AZ) was selected to pilot test surveillance strategies.
Work Groups and Surveillance Strategies Employed During Super Bowl XLIX and Related Events
Event-Specific Strategies
NFL Clinic
The NFL maintained a local clinic that offered healthcare services to NFL staff and their family members. MCDPH reviewed a daily report of all visits to the NFL clinic. The report included information on chief complaints, testing, and diagnosis for patients visiting the clinic. The line list was maintained in Microsoft Excel and emailed to MCDPH surveillance staff by the clinic physician.
Super Bowl Enhanced Animal Disease Surveillance (SBEADS)
MCDPH established a team of representatives from municipal, local, state, and federal agencies that work with animals (wild or domestic) to facilitate the surveillance and laboratory testing (if warranted) of adverse events in Maricopa County involving animals. Agencies represented included Arizona Game & Fish (AGF), the Arizona Department of Agriculture (ADA), the Arizona Department of Health Services (ADHS), the Arizona Veterinary Medical Association, the Midwestern University Veterinary School, the University of Arizona Veterinary Diagnostic Laboratory, the US Department of Agriculture (USDA, Veterinary and Wildlife Services), municipal and county animal control programs, and others. The primary role of the animal health team was to implement active surveillance for animal disease morbidity and mortality events that (1) would be considered unusual; (2) might involve a possible bioterrorism agent, such as plague, tularemia, anthrax, or smallpox; or (3) might signal a significant increase over expected levels of disease. A list of 24/7 agency contacts was established, and enhanced surveillance activities and communications were conducted from December 31, 2014, to February 6, 2015. Partners reported any identified issues by direct telephone call to the responsible agency for investigation and then reported any findings to the larger team on regularly scheduled conference calls.
Hotels and Urgent Care Facilities
MCDPH identified hotels and urgent care facilities within a 5-mile radius of the event sites in Glendale, Phoenix, and Scottsdale. Facilities identified were invited to participate in enhanced syndromic surveillance. Syndromes of interest to MCDPH were gastrointestinal illness (GI), influenzalike illness (ILI), rash illness, and neurological illness. Urgent care directors, managers, and nursing supervisors were given a link to a survey that asked the number of ILI, GI, rash, and neurological illness visits. For each syndrome, the survey asked if the number of visits reported was considered above normal. Hotel managers were asked to fill out a survey that asked if in the past 24 hours they had seen an increase in guests reporting symptoms for ILI, GI, rash illness, or neurological illness. Both hotels and urgent care facilities entered their information daily in online surveys.
Disease Reporting Line
MCDPH maintains a 24/7 call center for healthcare providers to seek consultations on issues of public health importance and report infectious disease cases. This line is referred to as the Disease Reporting Line (DRL) and is managed by the Banner Poison and Drug Information Center (later referred to as PCC), the American Association of Poison Control Centers' location serving Maricopa County. During the period of enhanced surveillance, PCC staff were trained to solicit information about possible exposure or attendance at events of interest and add the key words “Super Bowl” in the system for relevant reports. MCDPH reviewed PCC data daily to identify any increases in the number of flagged reports and any cases or exposures of public health concern. The concept of including the PCC as part of the enhanced surveillance during this special event was based on the National Institute of Health's framework for integrating PCC into public health activities. 8
Mapping
Real-time mapping capabilities were developed for syndromic surveillance at the Super Bowl, the Pro Bowl, and the NFL Experience as well as for hotel and urgent care syndromic surveillance. ArcGIS 10.2 was used to create these maps. The University of Phoenix stadium section seating charts were obtained to create digital databases depicting the sections. The field surveillance survey recorded section seating information, and maps were produced to illustrate section seating locations of people reporting syndromes or injuries. For the NFL Experience, geographic information system (GIS) databases depicting the Phoenix Convention Center floor plans were created based on computer-aided design (CAD) drawings, and event room designations were added based on an NFL Experience brochure that was available on the event's website.
Enhanced Surveillance Strategies
Outbreak Reports
Confirmed or suspected outbreaks of notifiable diseases are required to be reported to MCDPH by schools, providers, and hospitals in Maricopa County. These outbreaks are investigated and reported by MCDPH staff to ADHS in an electronic reportable disease surveillance system. MCDPH's outbreak summary report is routinely produced monthly using Statistical Analysis Software (SAS) 9.3 and summarizes all newly identified and ongoing outbreak investigations using this electronic database. This process was enhanced to increase report frequency to daily, and the report format was edited for communication with lay audiences.
Syndromic Surveillance for Emergency Room Visits
The Centers for Disease Control and Prevention's (CDC) National Syndromic Surveillance Program BioSense 2.0 platform was used to conduct syndromic surveillance of emergency departments in Maricopa County (see reference for further description of BioSense, syndrome definitions, and statistical methods). 9 Daily reports were created that included time series graphs of the percentage of emergency department visits for GI and ILI. The BioSense 2.0 Cumulative Sum 2 (C2) method with default options was used to detect increases above expected baseline levels. Additionally, through partnership and coordination with ADHS and CDC, a customized analytical program in R was created to identify Super Bowl–related terms, patients from out of state (with focus on team states), and bioterrorism agents of interest. If a syndrome category was statistically flagged or a single record was identified through the R program, MCDPH followed up with the relevant facility to investigate and request medical records when needed.
Mortality Surveillance
Review of death certificates is completed daily to identify deaths potentially caused by one of the 87 reportable diseases in Arizona. During this time of enhanced surveillance, mortality surveillance was expanded beyond infectious diseases to include a wider all-hazards focus. In addition to the infectious diseases already under surveillance, a list of circumstances and conditions that were of public health significance was developed mainly focusing on those factors most likely to affect large numbers of people. The factors included weather conditions, chemical and biological agents, transportation accidents (public transportation and multiple vehicle accidents), and drugs and alcohol. A list of International Statistical Classification of Diseases and Related Health Problems, 10th revision (ICD-10), codes and keywords associated with the chosen categories was developed and included as part of a query. The development and testing of the methodology was conducted using 6 years of retrospective death certificate data to identify the best combinations of key words and ICD-10 codes. This approach provided the ability to quickly identify deaths associated with any of the previously mentioned factors and flag for review any death related to infectious disease or a potential bioterrorism event.
A collaborative effort was established between the Maricopa County Office of the Medical Examiner (OME) and MCDPH to receive a list of decedents who were transported to the OME's facility the previous day. The list contained a brief description of the circumstances of death and scene data and was reviewed by MCDPH staff to identify suspicious or unusual deaths that could be of public health concern. The list also served as a reminder to the OME scene investigators to be more aware and vigilant in identifying cases that could be of public health importance and verbally notifying MCDPH if necessary.
Real-Time Onsite Syndromic Surveillance
Methods used by MCDPH in collaboration with the University of Arizona for real-time onsite syndromic surveillance during mass gatherings have been previously described. 6 Onsite syndromic surveillance was conducted for the Pro Bowl, the NFL Experience, and the Super Bowl. For each event, MCDPH worked with local fire and emergency medical services (EMS) agencies to place staff or volunteers in the first aid stations. Volunteers consisted of a combination of public health staff from various public health departments around the state and public health graduate students from the University of Arizona College of Public Health's Student Aid for Field Epidemiology Response (SAFER) team.
The system was designed using an active surveillance model in which guests who sought care at the first aid stations were asked additional questions about the nature of their illness or injury, predominant location during their stay, knowledge of any other guests who might be ill, and basic demographics (age and gender). The 4 main syndromes of interest were gastrointestinal (vomiting, diarrhea, nausea), respiratory (cough, shortness of breath, breathing distress, asthma attack), skin (rash, edema, excessive perspiration), and neurological (headache, dizziness, vision, seizures). Individual symptoms for each syndrome were also collected. For guests who presented at the first aid station with an injury, questions were focused on the nature of the injury as well as the location and circumstances in which the person became injured. All data were collected on tablets using a secure online survey system. As data were being collected in the field, MCDPH conducted real-time analytics for patterns and symptoms of concern, followed up with local healthcare providers if necessary, and mapped the data by facility and site in real-time to determine if any clusters of illness were present.
As was previously mentioned, 2 other events were also taking place: Super Bowl Central took up several city blocks in downtown Phoenix, and the Waste Management Open was a large golf tournament over 10 miles away from the other main events. For both events, EMS crews were not in a centralized first aid station but were either walking through the crowds or on golf carts and Segways. It was not logistically possible to have MCDPH staff in the field with them as was possible for the other events because of this decentralized set-up. Instead, a staff member was placed in the dispatch room, which served as the call center for both Phoenix and Scottsdale fire and EMS services, to collect data from the dispatchers as it came in. This was possible because a single dispatcher was responsible for each event and could share information about the nature of the call and the location as it was actively being managed.
Arizona Prehospital Information and EMS Registry System (AZ-PIERS)
Data from Arizona's pre-hospital registry (AZ-PIERS) was used to identify individuals with gastrointestinal and respiratory symptoms. AZ-PIERS data contain field visit data voluntarily submitted by fire departments and emergency medical services. From the database, primary impression, secondary impression, and primary symptom fields are used to select cases with any symptoms consistent with GI (eg, abdominal pain, diarrhea, nausea/vomiting, GI problems) or ILI (eg, cough, sore throat, fever, upper respiratory infection, breathing problems). These lists are usually compiled once per week, but during Super Bowl events, the system was enhanced to obtain a daily list of de-identified individuals with GI or ILI symptoms. Algorithms to detect GI and ILI cases were created in SAS 9.3, and the program was run daily during events.
Previously Existing Surveillance Strategies
Enhanced Surveillance Alert
An enhanced surveillance alert was sent to healthcare providers in Maricopa County requesting that they voluntarily report increases in illness or injury as well as any unusual illness presentation associated with any of the events under surveillance. The alert was distributed by email through the county's established notification system and was in place from January 22, 2015, to February 6, 2015.
Influenzalike Illness
Sentinel ILI surveillance has been in place at MCDPH for several years in accordance with CDC guidelines for outpatient influenza illness surveillance. 10 The system routinely collects information from selected local emergency departments and outpatient clinics in Maricopa County. During this time enhanced ILI surveillance was in place, and a report compiling the number of outpatient ILI cases from the previous day was reviewed for detection of sudden increases in ILI activity.
Media Surveillance
MCDPH monitors several sources for media reports of public health relevance, including information related to disease spread and public health threats in our community, as well as emerging disease and public health threats in the United States and throughout the world. Media surveillance is done by scanning a list of relevant news websites, such as the Arizona Republic, and monitoring aggregated Twitter feeds. Also, MCDPH staff subscribe to several news websites, government websites, and breaking news alerts. These websites are routinely monitored to identify public health threats. A media surveillance report is usually distributed every Friday, but during the Super Bowl events, this report was done daily.
Aberration Detection Algorithms for Reportable Diseases
Morbidity data were retrieved using the Medical Electronic Disease Surveillance Intelligence System (MEDSIS), an Arizona statewide surveillance system for reportable infectious diseases. There are 87 diseases deemed reportable by the Arizona Administrative Code. Morbidities of interest during the surveillance period were selected by MCDPH based on the following: incidence of the disease, severity of illness, and person-to-person transmissibility. Human Remains Release Form (HRRF) data were collected from the Office of Vital Registration. Reported diagnoses were grouped into appropriate syndromic categories: respiratory, gastrointestinal, etc. Two advantages in using MEDSIS and HRRF data were that, first, both data sources were updated daily, and, second, both sources had at least 4 years of historical data.
There are several aberration detection methods that can be implemented in public health departments for detection of anomalies in surveillance data. 11 During Super Bowl 2015, MCDPH used 2 methods: Poisson regression and cumulative sums.
A series of algorithms measured current levels of syndromes or morbidities and quantified variations based on the historical averages as a baseline. The surveillance period was a 7-day moving average from the date of running the program. A total of 12 7-day intervals were used to estimate a baseline rate. The intervals used were as follows: for each of the 4 preceding years (2011-2014) a 7-day interval of the same surveillance period, a preceding 7-day interval, and a subsequent 7-day interval. Aberrations were flagged when levels of disease were greater than or less than 2 standard deviations away from the historical mean, using Poisson regression and the cumulative sums analysis. These statistical methods were used to adjust for confounders such as seasonality and past outbreaks. The aberration detection programs were written in SAS 9.3.
The program was run daily and a summary table of disease and syndrome levels was generated to outline which specific morbidities were flagged as having aberrations. These reports made it easy for MCDPH to share results with partners and make the results understandable to people from other organizations.
Laboratory
The Arizona State Public Health Laboratory (ASPHL) provides ongoing testing support to MCDPH and provided testing support during all events.
Results
A total of 67,813 people attended Super Bowl XLIX, 49,099 attended the Fiesta Bowl, and 63,225 attended the Pro Bowl. Total attendance for the NFL Experience was 165,403 (9-day average of 18,378), and 564,368 (7-day average of 80,624) attended the Waste Management Open. From January 23 to February 1, 2015, the MCDPH Incident Command Center (PH-ICC) was activated and the Intelligence Section, responsible for enhanced epidemiologic surveillance activities, produced daily intelligence section reports summarizing results from each of the surveillance methods and highlighting any findings of public health significance (Figure 1). The reports were distributed to the event Multi-Agency Coordination Center (MACC) and other partners and stakeholders. MCDPH representatives at the coordination center, together with the incident command center, conducted risk assessments, and the MCDPH public information officer managed risk communications.
First Page of the Daily Intelligence Section Report
NFL Clinic
From January 23 to January 31, the days the clinic was in operation, 51 individuals visited the NFL clinic. Visit complaints included ILI (n = 7), muscle strains or body pain (n = 7), allergies/allergic rhinitis (n = 6), bronchitis (n = 4), sinusitis (n = 2), and various other complaints (n = 25). Of the 7 ILI complaints, 6 were rapid influenza A test positive, and 1 individual rejected testing. A case complaining of pharyngitis was confirmed as streptococcal pharyngitis. No other cases had testing performed.
SBEADS
Several events in Maricopa County were reported through SBEADS. A sick cat in Cave Creek was tested for plague and tularemia. Specimens (node aspirate and swab) collected from the cat were tested at ASPHL. Results were negative, and plague and tularemia were ruled out. Also, ADA staff investigated suspected cases of highly pathogenic avian influenza (HPAI) in a backyard chicken flock in Phoenix. Several chickens had died after a local resident purchased chickens in Oregon and transported them to Phoenix. Laboratory results were negative. In addition, a local veterinarian diagnosed a suspected case of Rocky Mountain spotted fever in a dog in Sun City West. The diagnosis was based on clinical symptoms and a moderately high IgG antibody titer. Events reported from other counties in Arizona included: (1) an ADA investigation of cases of vesicular stomatitis virus in horses in Santa Cruz County; (2) an unexplained mortality event involving waterfowl and a few owls was reported in the Cibola Wildlife Refuge along the Arizona-California border, for which HPAI was considered to be low suspicion; (3) leptospirosis diagnosed in a dog in Mohave County, and suspected in another dog in the same household that had died a week or 2 earlier.
Hotels and Urgent Care Facilities
MCDPH identified 35 urgent care facilities within a 5-mile radius of the events (Figure 2) and was able to partner with 32 of these. We also partnered with 16 hotels. Some urgent care facilities reported that visits to their facilities were above the number expected; most reports were for ILI (Table 2). Hotel reports were minimal. At the time, we were unable to determine if this was because there was nothing relevant to report or if it was due to lack of buy-in from hotel partners.
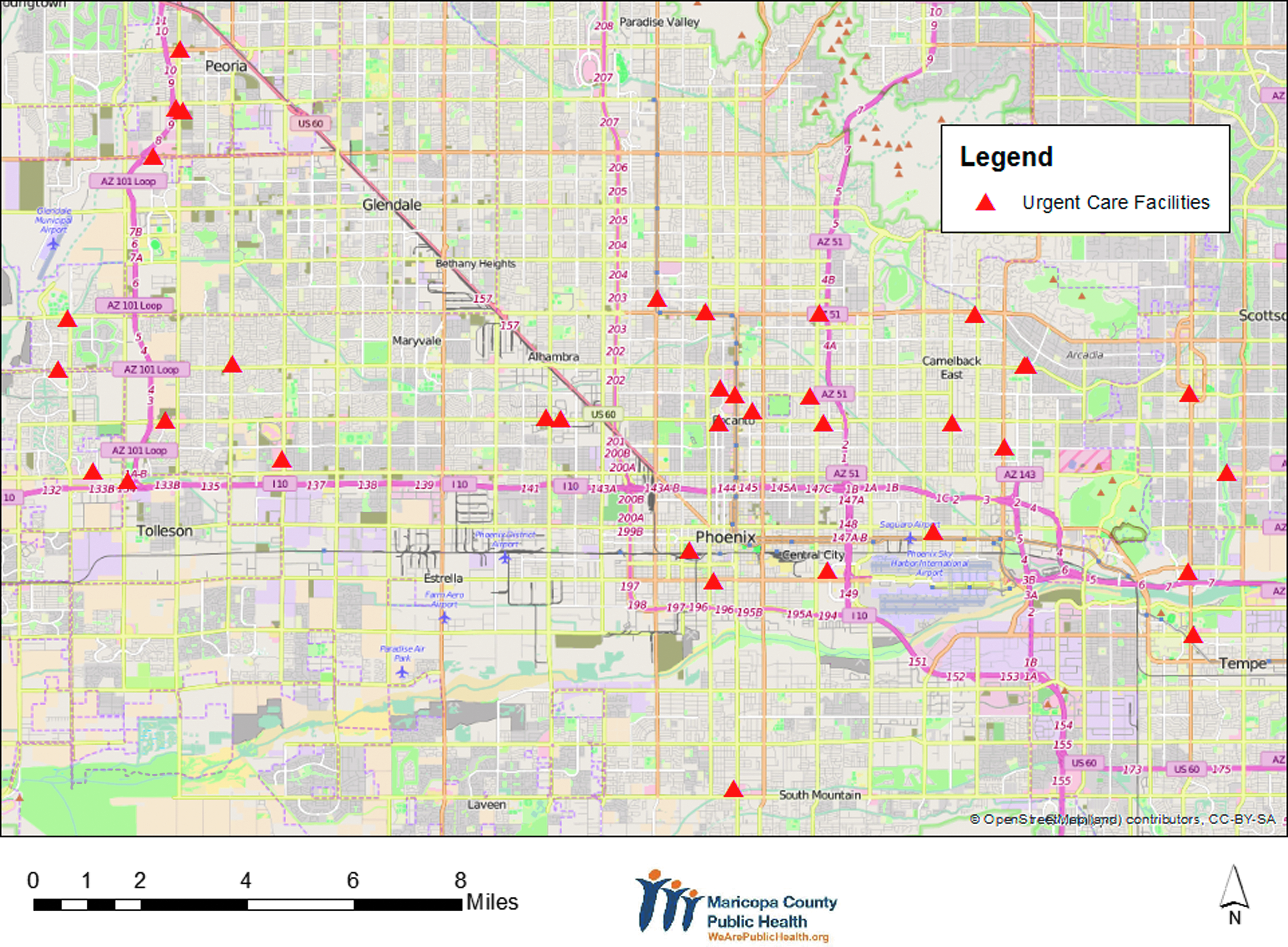
Urgent Care Facilities Identified for Surveillance During Super Bowl XLIX
Syndromic Surveillance at Urgent Care Facilities During Super Bowl XLIX and Related Events
Disease Reporting Line
A report regarding an individual attending a Super Bowl event in Scottsdale was flagged by the disease reporting line. The individual indicated the wine being served at the event had an unusual taste. The individual did not require healthcare attention, and the report was ruled out as not a significant public health concern. No other events were flagged by the disease reporting line.
Outbreak Reports
During the Super Bowl events, there were 9 open outbreak investigations (4 influenza investigations, 3 pertussis investigations, 1 respiratory, and 1 GI), all investigations unrelated to Super Bowl events. There were also ongoing measles investigations linked to an exposure at Disneyland around the same time as Super Bowl XLIX but unrelated to it. 12
Syndromic Surveillance for Emergency Room Visits
BioSense monitoring also indicated increases in rash and measles syndromes. In order to assist with the measles investigation, we decided to create daily rash and measles reports in BioSense, identify high suspects for measles (rash, fever, and a mention of measles in the chief complaint), and order medical records as needed. Although several suspect cases were investigated based on BioSense data, none of these resulted in identification of a confirmed measles case.
Mortality Surveillance
A cyanide single event exposure was reported by the OME and law enforcement partners. The cyanide event was investigated and determined not to be a public health threat. No other public health concerns were identified using mortality surveillance.
Real-Time Onsite Syndromic Surveillance
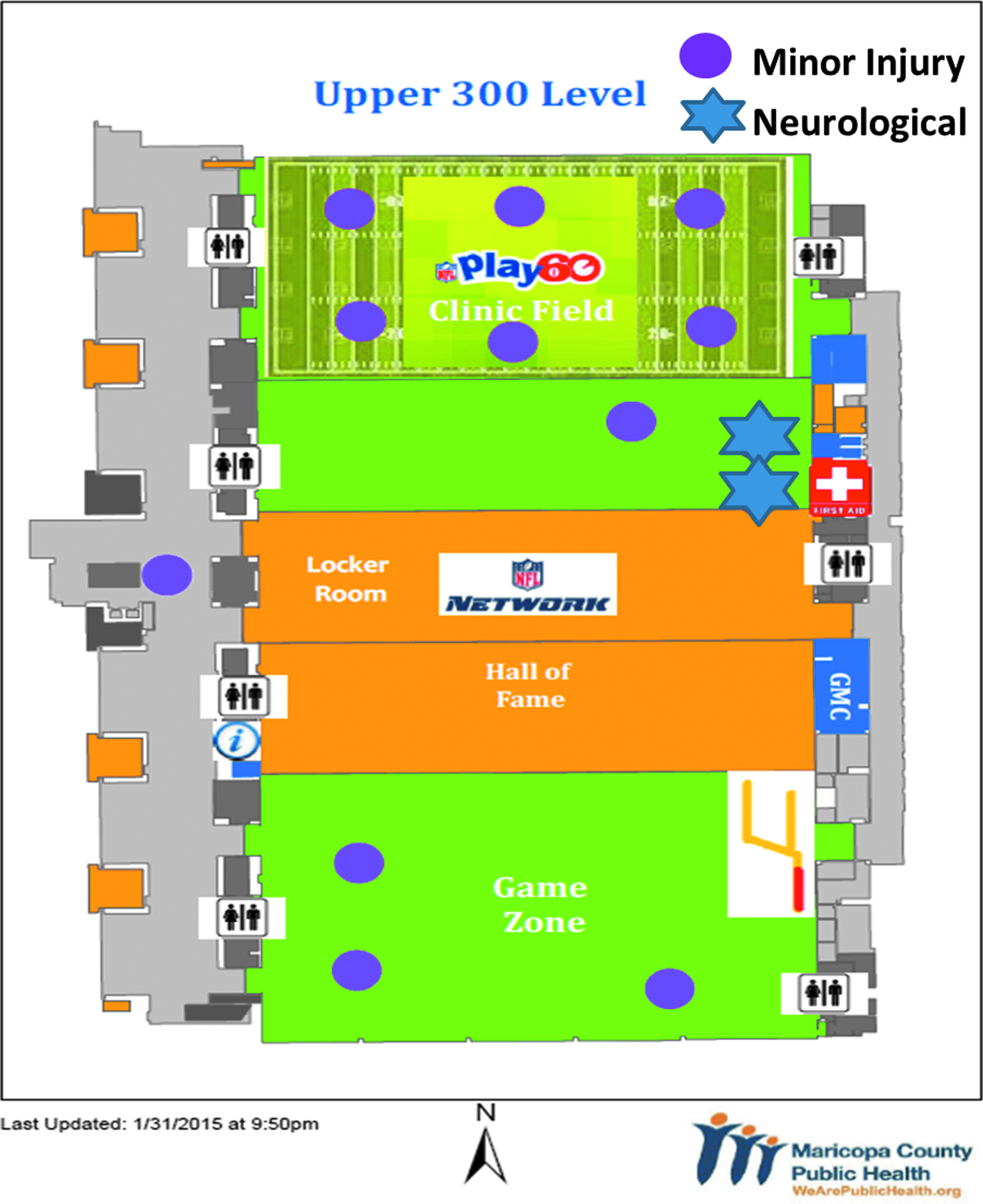
Overall, onsite syndromic surveillance efforts documented minor injuries more often than illnesses at all of these events (Table 3). For the 2 events inside the University of Phoenix stadium (Pro Bowl and Super Bowl), injuries (n = 15 and n = 20, respectively) were only slightly higher than illness (n = 15 and n = 17, respectively). For these events as well, neurological symptoms including headaches (n = 10 at each) were most commonly reported, followed by gastrointestinal (n = 4 and n = 5, respectively). Reported injuries were much higher for the NFL Experience (n = 145) compared to illnesses (n = 63), but surveillance took place over 9 separate days, with the highest numbers reported on weekend days when crowds were the largest. For this event, neurological symptoms were also the most commonly reported (n = 44), followed by respiratory (n = 10) and gastrointestinal (n = 7). The most commonly treated injuries among NFL Experience guests were cuts (n = 56), sprains (n = 27), and bruises (n = 20). Other types of injuries included getting hit in the head (football) or face, joint pain or injury, and burns.
Reported Syndromes by Major Event a
Symptoms and injuries are not mutually exclusive. For example, a person may report a gastrointestinal and respiratory symptom (each counted once), but only be counted as 1 illness complaint.
Also as a result of the measles investigation, the decision was made to add a question to the onsite syndromic surveillance survey about measles vaccine status. Field surveillance staff at a first aid station identified a girl with recent travel to Los Angeles complaining of rash and fever. Although her father indicated the girl had been vaccinated against measles, out of an abundance of caution, the girl was removed from the crowd and sent for further evaluation at a local clinic, where measles was ruled out.
Data collected from the emergency dispatching center for the Waste Management Phoenix Open and Super Bowl Central were small and ultimately not included in any analyses (data not shown).
Other Reports
We did not identify any public health concerns from AZ-PIERS reports, nor did we receive any reports from partners participating in Enhanced Surveillance Alert. Widespread influenza activity was reported by ADHS during the Super Bowl events. However, this level of activity was reached before Super Bowl events began. Public health media surveillance recorded concerns about measles and influenza in the population, and aberration detection algorithms reflected the corresponding increase in measles reports associated with the Disneyland exposure.
Seat-specific real-time mapping capabilities for onsite syndromic surveillance at Super Bowl XLIX, the Pro Bowl, real-time mapping at the NFL Experience, and mapping for hotels and urgent care facilities allowed MCDPH to closely monitor the distribution of syndromes and injuries reported (Figure 3).

Onsite Syndromic Surveillance, University of Phoenix Stadium
Discussion
Structured planning meetings with key partners and review of methods from other jurisdictions in advance of events were instrumental in the successful implementation of enhanced epidemiologic surveillance efforts. The flexibility of the different systems to adapt to challenges proved to be essential to effectively responding to public health concerns. Gastrointestinal and respiratory conditions were among the highest concerns during the planning phases, since Super Bowl XLIX took place during influenza season and events had a significant number of food vendors. However, monitoring for symptoms compatible with measles became a very high priority during the events, and we were able to adjust operations and systems to respond as needed.
Real-time onsite syndromic surveillance allowed public health professionals and students to be in the field and interact with first responders, and it allowed public health data to be collected quickly and in a format that was easy to analyze by health department staff. Use of data for daily updates also allowed other agencies to get a quick snapshot of the general health of the participants and be prepared to respond quickly if anything changed. One of the activities with the most potential for early impact was the mapping of cases as they were reported. Volunteers in the field were aware of what was going on only in their own first aid station. This could mean that 4 people who were all sitting near each other could become ill, but they could potentially each visit separate first aid stations. Mapping these data as they come in allows public health workers to determine if cases are sitting near each other and could potentially be related. If done quickly, this information can be passed back to the field volunteers, who can then be aware of a potential cluster of illnesses by location.
Onsite syndromic surveillance has been used by MCDPH since the 2008 Super Bowl, when it was first developed in collaboration with the University of Arizona. However, this was the first set of events that included questions about injuries. The injury questions were added because of observations from previous events where the majority of complaints seen in the first aid stations were related to injuries. The health department wanted to collect this data and provide information back to the organizers of the events. It is not surprising that the number of injuries was much higher for the NFL Experience, given the nature of the event compared to the games themselves. The NFL Experience is open to the general public, has high numbers of attendees, and includes various activities such as running, tackling, and throwing balls, in which people of all ages can participate. Injury information gathered about certain activities was shared with EMS crews, who pushed the information out to event organizers. This resulted in the implementation of additional signage and recommendations about the importance of stretching and warming up before participation.
We found that surveillance in the emergency dispatching center was not beneficial, since the amount of data relayed by the dispatcher to our public health volunteers was very limited. A better strategy would have been to have fire department data electronically available to the health department. However, electronic data sharing takes a considerable amount of planning and agreements between agencies. MCDPH is currently working on a system to gather data from the dispatch center.
The measles investigations associated with an exposure at Disneyland showcased the utility of surveillance strategies for early detection of illness (even before health care is sought), and the usefulness of maintaining close collaborations with EMS, law enforcement, and fire departments. For example, field surveillance staff at a first aid station identified a girl who had recently traveled to Los Angeles; she was immediately removed from the crowd and sent for further evaluation. Another example was an arrest made by law enforcement in which the individual in custody claimed to have been exposed to measles. Public health followed up on this claim, and measles exposure was ruled out. These collaborations with EMS and law enforcement allowed public health to easily conduct investigations while public safety was also maintained.
Onsite Syndromic Surveillance, NFL Experience, January 31, 2015
SBEADS was a novel approach for MCDPH, and partners demonstrated a high level of support for the system. Reports received during Super Bowl XLIX showcase the utility that a system like this can have to improve situational awareness and early detection of potential exposures to bioterrorism agents that affect both animal and human populations.
This event was also the first deployment of syndromic surveillance for mass gatherings using BioSense 2.0 in Maricopa County, and the system was useful in identifying potential cases of measles during our outbreak investigation and proved to be a great starting point in obtaining medical records.
Syndromic surveillance at hotels and urgent care facilities was also a new approach. Urgent care facilities actively reported into the system, and reports reflected increases in ILI as expected around this time period. In contrast, reports from hotels were limited. Urgent care facilities are clinical settings that may be more willing to collaborate with public health surveillance efforts than are nonclinical partners such as hotels. Perhaps more coordination and planning were needed to work with hotels on reporting. The utility of hotel surveillance in this jurisdiction and for these types of events remains to be determined.
Overall, the wide variety of surveillance strategies and partnerships in place during Super Bowl XLIX events showed the benefits of public health collaboration with traditional hospital partners but also with other partners, such as urgent care facilities, fire departments, EMS, and law enforcement for surveillance during mass gatherings. Public safety agencies might not have access to real-time information about circulating diseases and their spread and could benefit from partnering with public health to receive and interpret the information. Public health in turn benefits by increasing the timeliness, comprehensiveness, and quality of surveillance data so they can respond more quickly.
MCDPH plans to continue building syndromic surveillance systems, determining high priority syndromes to monitor during mass gatherings, and developing new external data streams to include 911/dispatch center data from fire departments. We would also like to develop a matrix to determine which special events require enhanced surveillance and the level of monitoring needed. Finally, report templates will be created to effectively communicate epidemiologic surveillance results to lay audiences in a timely manner.
Footnotes
Acknowledgments
The authors wish to thank Anne Vossbrink, Rogelio Martinez, David Leinenveber, PCC, SAFER, the NFL medical team, Scott Zusy and staff from MC Environmental Services, Joli Weiss and the ADHS Office of Infectious Disease Services, William Slanta and the ASPHL, Rebecca Sunenshine, Mitchell Lach, Tammy Sylvester, Ron Klein, Rasneet Kumar, the Maricopa County Super Bowl Surveillance Planning Group (Yixia Li, Katherine Aherns, Rechelle Kelly, William McConahey, Jigna Narang, Darcie Bentz, Keely Muertos, Siru Prasai, Melissa Kretschmer, James Matthews, Nicole LaMantia, Hovi Nguyen, and Jackie Ward), Melanie Sarino and David Balkcom for their work in the Dispatch Center, and all the staff from the MCDPH Office of Epidemiology and Office of Preparedness and Response.