
Abstract
We analyzed the mass influenza vaccination clinic process at the United States Naval Academy to identify gaps and implement changes for improvement. The Lean Six Sigma methodology was employed. Total number of staff members working the clinic and total hours worked were measured at baseline in August 2013 and after implementation in August 2014 to determine improvement. The clinic was moved from a hallway to an auditorium, and a linear patient flow was established. Staff members wore vests for easy identification, and the supply box was reorganized. Training was standardized and given to all staff members before working in the clinic. These changes decreased the number of staff members required to work in the clinic from 62 to 40 (–35.5%) and decreased the total number of hours worked from 558 to 360 (–35.5%). The changes successfully improved the mass vaccination clinic by decreasing staffing and hours required. These changes can be adopted in other settings to increase community capacity and readiness.
The authors analyzed the mass influenza vaccination clinic process at the United States Naval Academy to identify gaps and implement changes for improvement. Total number of staff members working the clinic and total hours worked were measured at baseline in August 2013 and again in August 2014 to determine improvement. The changes successfully improved the mass vaccination clinic by decreasing staffing and hours required.
M
The US government created the Strategic National Stockpile (SNS) in 1998 to address the need for quick distribution of medical supplies to support a public health emergency. State and local authorities are responsible for subsequently dispensing medicines and supplies to the population. 9 The Centers for Disease Control and Prevention (CDC) created the Cities Readiness Initiative (CRI) in 2004 to assist communities in developing mechanisms to efficiently dispense medical countermeasures within 48 hours from the time the federal decision is made to dispense SNS supplies. The CRI focused on developing and funding thousands of open points-of-dispensing (PODs) in 72 metropolitan statistical areas 10 and dramatically increased public emergency preparedness over the next several years. 11 Public health departments experienced great success in implementing POD plans, coordinating training exercises,12-14 and using training data in computer models to determine methods to improve traffic flow and throughput.15,16
Closed PODs are an alternative dispensing modality that would target a specific population. The Institute of Medicine encouraged development of closed PODs, such as for corporations and private businesses, to alleviate the burden on open PODs during emergency situations. 9 This is ideal for health institutions where employees would be expected to remain functional during a public health emergency. A recent nationwide survey found a gap in closed POD preparedness, but it did show that jurisdictions that had at least 1 closed POD had higher levels of staff member confidence in the ability to provide effective medical countermeasures within 48 hours of an emergency situation. 17
Background
The armed forces of the United States are a unique population because of its members' increased risk of exposure to bioterrorism, 18 infectious disease through crowded living quarters, and endemic illnesses on deployment.19,20 Mass immunization programs have long been a routine component of medical readiness since their first implementation in 1777 to immunize Continental Army trainees against smallpox. 21 The United States Naval Academy (USNA) provides the influenza vaccine annually to 4,500 midshipmen in 6 hours over 3 days via a mass vaccination clinic staffed by Naval Health Clinic Annapolis (NHCA). The set-up of the clinic is analogous to a closed POD. Previous clinics revealed midshipmen's dissatisfaction with long lines, disruption because of the POD's proximity to the dormitory areas, and confusion on patient flow through the clinic. Staff members expressed equal frustration with patient flow, lack of confidence from inadequate training, and the disruption of their concurrent daily responsibilities. The annual occurrence of the clinic offered a unique opportunity to implement a quality improvement project. This article outlines the identification and improvement of gaps in the mass vaccination process.
Methods
Selecting the Methodology
The quality improvement project used the Lean Six Sigma (LSS) methodology to plan and implement changes to the mass vaccination clinic. Six Sigma allows users to improve product quality by determining the relationship between output and errors in process inputs. The name comes from a statistical model of manufacturing in which sigma refers to standard deviation of product variability. The Lean principle revolves around waste elimination and process velocity optimization. Where Lean lacks statistical control and organizational infrastructure, Six Sigma is a complex method that does not emphasize process efficiency. Combining the 2 principles into the LSS methodology created a business improvement framework that addresses both quality and speed.22,23
The Bureau of Medicine and Surgery (BUMED) of the US Navy began training healthcare leaders and staff in LSS methodology by implementing certification training programs known as green belts and the more advanced black belts in 2006. By 2009, BUMED recognized LSS to be a successful quality improvement methodology and supported the process as the primary approach for performance improvement. 24 In November 2013, NHCA trained its first green belt to support its mission to optimize the health and readiness of the brigade of midshipmen. Numerous studies have been published on the LSS tools and methodology, and its application to this study will be briefly explained in this section.
Commissioning the Team
An LSS team was commissioned, which included a green belt, a master black belt, and an LSS champion. The team first created the project charter to outline the problem statement, expected mission benefits, expected financial benefits, and improvement goals using specified metrics. A communication plan was devised going forward.
Determining the Metrics
The team decided to measure process efficiency by the total number of staff members working the clinic and the total number of hours worked. The team set improvement goals for each metric by which they would consider the implementation to be successful. Team members obtained baseline data from the mass influenza vaccinations clinic in August 2013.
Planning the Process
During subsequent meetings, the team developed a rough sketch of the vaccinations process using a SIPOC (suppliers-inputs-process-outputs-customers) diagram to visualize the entire process to ensure team members had the same understanding of all steps involved. The steps were further detailed through a process map (Figure 1), which was defined to start when a midshipman checked in at the clinic and to end when the staff member collected the patient's record at checkout. The LSS team used value stream analysis to identify the non-value-added steps and decreased process complexity through standardization. The team used a fishbone diagram and root cause analysis to identify areas of clutter where Lean tools could be used to reduce waste, and they informally surveyed staff members and midshipmen to determine the “voice of the customer.” An implementation plan was created and implemented during the mass influenza vaccinations clinic in August 2014.

Post-implementation Process Map. The process starts when the midshipman checks in at the clinic and ends when the staff member collects the patient's record at checkout.
Results
At baseline, 62 staff members worked the mass vaccinations clinic for a total of 558 hours. The LSS team set improvement goals at 10% reduction in both metrics, equivalent to 56 staff members and 502 hours. The post-implementation clinic greatly exceeded the goals and decreased the number of staff members to 40 (–35.5%) and total hours worked to 360 (–35.5%). The changes led to a decreased need for traffic control, staff members administering the vaccines, and staff members running the checkout station. The team recorded and archived all process documents and results. New standard operating procedures (SOPs) were created and documented for future clinics. The team presented project success to the command's executive steering committee. Major issues addressed are discussed below.
Station Layout
The clinic was originally set up in the hallway outside the midshipmen's dormitory (Figure 2). The midshipmen were directed to receive either the live attenuated influenza vaccine (LAIV, FluMist) or the inactivated influenza vaccine (IIV, flu shot) according to their medical history as determined by a nurse or healthcare provider. The enclosed space did not allow much flexibility for clinic set-up. The patient flow was nonlinear, and midshipmen were confused about where to go next. The enclosed space forced LAIV and IIV stations to be close to one another. In addition, midshipmen who had received their vaccination had to walk through the other vaccination stations in order to exit, leading to a mixing of vaccinated and unvaccinated midshipmen. If midshipmen were not paying attention, they could inadvertently stand in another line before a staff member recognized the error and redirected them. Staff members working the clinic for the first time were not familiar with the layout and were unsure of where to direct the midshipmen. Stations at the end of the hallway did not always have patients because midshipmen and staff members did not realize there was an open station. The potential for disorder required more staff members for traffic control. The clinic's proximity to the dormitories caused disruption of other events occurring at the same time.
Layout of the Baseline Clinic in 2013. LAIV = live attenuated influenza vaccine (FluMist); IIV = inactivated influenza vaccine (flu shot). Numbered circles depict staff member roles: 1 = traffic control, 2 = check-in, 3 = LAIV vaccinator, 4 = IIV vaccinator, 5 = checkout. Black circles depict a nurse or healthcare provider.
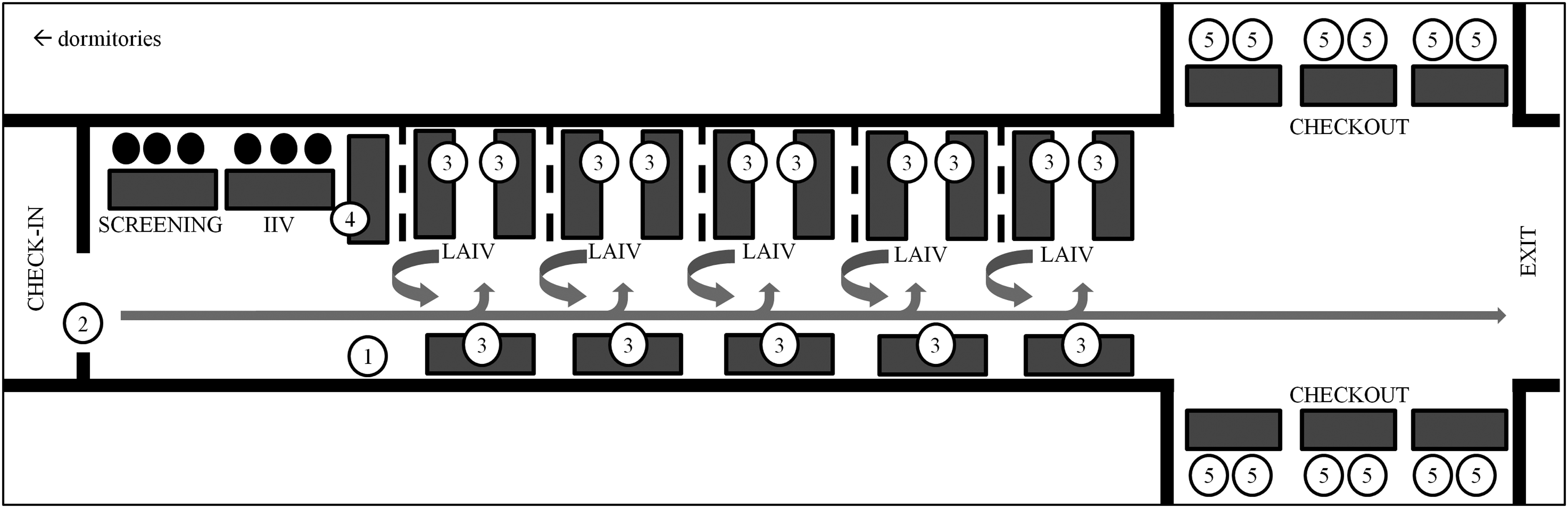
Post-Implementation: The location of the clinic was moved to an auditorium (Figure 3). The open space allowed staff members to create a linear patient flow using visual tape and other physical barriers to guide midshipmen down specific paths. The rows of seating in the auditorium naturally created line separation for each vaccination station. Traffic control was necessary only at a divergence of 2 pathways. For the entire process, IIV patients remained separated from LAIV patients, and vaccinated patients remained separated from unvaccinated patients. The decreased number of traffic control needs reduced the overall number of staff members.

Layout of the Post-implementation Clinic in 2014. LAIV = live attenuated influenza vaccine (FluMist); IIV = inactivated influenza vaccine (flu shot). Numbered circles depict staff member roles: 1 = traffic control, 2 = check-in, 3 = LAIV vaccinator, 4 = IIV vaccinator, 5 = checkout. Black circles depict a nurse or healthcare provider.
Staff Member Identification
Because midshipmen wear distinctive uniforms, it was easy to distinguish between staff members and patients. However, midshipmen would often direct questions to the incorrect staff member. Inquiries concerning the traffic flow or directions on how to complete the paperwork should be directed to staff members assigned to the check-in station or to traffic control.
Post-Implementation: Designated team leaders in each area wore colored vests that further identified them to the midshipmen and helped direct questions appropriately to them. Providers and nurses were not approached for simple questions, leaving more time to focus on medical decisions associated with vaccine contraindications.
Supplies Organization
In the original clinic, staff members were confused on where supplies were kept. The nonlinear pathway created confusion about the deficient or surplus status of each vaccination station. Varying distances between stations also led to an unnecessary transport of vaccines, sharps, and equipment.
Post-Implementation: The LSS team placed all the supplies in a standardized blue box and made a checklist with pictures of each box. Trained staff members knew exactly how the supplies were stored and could easily locate them during the clinic. The new layout placed the stations closer together, and the proximity to the supply box allowed easy access and decreased transport distance.
Staff Member Training
Previously, most staff members did not receive adequate training before arriving at the clinic. A lack of standard instructions led to variation and subsequent confusion among staff member about how each station was operated. New staff members felt especially frustrated and confused if they had not previously participated in the mass influenza vaccinations clinic. Corpsmen reported feeling inadequately trained on the influenza vaccine, leading to a lack of confidence on how to administer the vaccine.
Post-Implementation: The training process was standardized and documented as SOPs to ensure each staff member received the same training every year. Corpsmen received additional video training on how to administer the vaccinations.
Discussion
The LSS team in this case study used the lessons learned from previous mass vaccination clinics at the USNA to implement changes and increase process efficiency. The team relocated the mass vaccinations clinic to the auditorium and reorganized the layout to create a linear patient flow. The new layout decreased the need for traffic control and created clear separation between vaccinated and unvaccinated midshipmen. Staff members were identified more easily, and supplies were organized in a predetermined manner. The team documented the procedures and trained the staff members before arriving at the clinic. The implemented changes standardized the process and reduced much of the confusion, leading to a decrease in the number of staff members required to work in the clinic and a decrease in the number of hours needed to vaccinate the same number of midshipmen. The decreased number of hours worked offers the potential for increasing the number of vaccination lines in future clinics.
Documentation of changes not only ensures that the same process is carried out year to year, but contributes to a community's private-public partnership by providing a written plan that other institutions can reproduce. The open location of the USNA auditorium creates a layout that is easily replicable in response to most public health emergencies, such as mass vaccinations or mass distribution of prophylaxis. The team's process map and clinic layout documents were shared with the local county hospital to increase the capacity and resilience of our community. The annual occurrence of our clinic allowed the LSS team to address gaps and implement changes that other clinics can simulate with annual training exercises. Several studies have similarly shown decreased total time to vaccinate the targeted population by conducting annual exercises, providing pre-event training, and documenting a written plan.11,16,17 We consider the study to be successful because it greatly exceeded initial expectations to decrease the number of staff members and number of hours worked by 10%.
Limitations
There are several limitations in our study. We could not evaluate the true effectiveness of our clinic without measuring throughput. Although this was the most commonly used measurement in previous studies, the LSS team felt that this measure did not adequately reflect their intent. The team wanted to improve the vaccination process so that fewer staff members would be diverted from their routine responsibilities and the fewer number of hours required would minimize disruptions to the normal NHCA clinic schedule.
Additional limitations relate to the military nature of the USNA. Staff members are expected to perform their duties when ordered, so we do not anticipate having a shortage of volunteers to run the clinic in an emergency. Our patients are midshipmen, who are expected to remain disciplined at all times and follow the instructions of their superiors. Most significantly, emergency preparedness is an essential component of military installations. Staff members are expected to devote additional time and resources beyond their primary responsibilities to develop standard protocols for responding to various emergency situations, including public health scenarios. The Department of Defense requires all military institutions to run annual drills. Nonmilitary institutions may find it more difficult to garner staff support and buy-in for a time-intensive undertaking.
Future Studies
Several issues identified in the “voice of the customer” were not addressed in this study, including the midshipmen's frustration with long lines. A post-implementation survey should be conducted after the clinic to reevaluate the midshipmen's and staff members' levels of satisfaction. Because we made several changes simultaneously across the entire process, it is difficult to ascertain which change had the greatest effect on our outcomes. Approximately 50% of the staff members in the 2014 post-implementation clinic held the same role as in the 2013 baseline clinic, and our improvement may be partially attributable to increased experience. Future clinics could consider having multiple clinics with different changes implemented. The increased training also required additional time outside of the measured number of hours, and it would be prudent to include that time in future studies.
Conclusion
Our study supports the feasibility of planning and training for a closed POD and contributes to best practices. Closed PODs are becoming increasingly familiar as more communities consider their utility in emergency preparedness plans. We encourage all communities to incorporate closed PODs in their plans to maximize coverage of their populations.