
Abstract
The primary goal of biosafety education is to ensure safe practices among workers in biomedical laboratories. Despite several educational workshops by the Pakistan Biological Safety Association (PBSA), compliance with safe practices among laboratory workers remains low. To determine barriers to implementation of recommended biosafety practices among biomedical laboratory workers in Pakistan, we conducted a questionnaire-based survey of participants attending 2 workshops focusing on biosafety practices in Karachi and Lahore in February 2015. Questionnaires were developed by modifying the BARRIERS scale in which respondents are required to rate barriers on a 1-4 scale. Nineteen of the original 29 barriers were included and subcategorized into 4 groups: awareness, material quality, presentation, and workplace barriers. Workshops were attended by 64 participants. Among barriers that were rated as moderate to great barriers by at least 50% of respondents were: lack of time to read biosafety guidelines (workplace subscale), lack of staff authorization to change/improve practice (workplace subscale), no career or self-improvement advantages to the staff for implementing optimal practices (workplace subscale), and unclear practice implications (presentation subscale). A lack of recognition for employees' rights and benefits in the workplace was found to be a predominant reason for a lack of compliance. Based on perceived barriers, substantial improvement in work environment, worker facilitation, and enabling are needed for achieving improved or optimal biosafety practices in Pakistan.
To determine barriers to implementation of recommended biosafety practices among biomedical laboratory workers in Pakistan, the authors conducted a questionnaire-based survey in 2015. Among barriers that were rated highest were lack of time to read biosafety guidelines, lack of staff authorization to change or improve practice, no career or self-improvement advantages to the staff for implementing optimal practices, and unclear practice implications. A lack of recognition for employees’ rights and benefits in the workplace was found to be a predominant reason for a lack of compliance. Substantial improvement in the work environment is needed to improves biosafety practices in Pakistan.
B
In view of the lack of biosafety training among biomedical laboratory workers in Pakistan, the Pakistan Biological Safety Association (PBSA) 5 was established in 2008 with the aim to train workers and establish a national resource for biosafety education and training. To channel recommended guidelines into routine practice, a change in behaviors is required, and recognition of this issue resulted in several consecutive biosafety training sessions in the form of workshops and symposia. Several training workshops were conducted from 2008 to 2013. A summary of training activities carried out by PBSA since its inception is provided in Table 1.
Biosafety workshops and activities organized by the Pakistan Biological Safety Association (PBSA), 2008-2013
Recent publication of formative assessments at workshops conducted by PBSA and by other organizations has revealed that biosafety practices in national laboratories have failed to improve.6-8 Several recent studies published after these workshops have indicated that biosafety practices are suboptimal among laboratory workers, while also suggesting that knowledge and awareness of guidelines remain low even after attending training sessions. Sequential workshops have increased awareness since 2010, when 85% of laboratory workers reported a lack of training, to 2014, when only 40% of laboratory workers reported a lack of training in biosafety practices. Compliance rates as determined by these surveys in 2010 and 2014 are shown in Figure 1. A limitation of this comparison may be that nonstandardized techniques were used in the surveys, and, moreover, participants are likely to have been from different institutes, albeit with moderate overlap.

Compliance rates to optimal biosafety practices in various biomedical laboratories across Pakistan in 20106 and 20147,8 based on laboratory worker reports. The 2010 and 2014 surveys by Nasim et al and Khan et al were carried out in Karachi, while the 2014 survey by Ghanchi et al was carried out in Karachi and Lahore. X axis shows percent compliance.
Nevertheless, the variability in reported rates of compliance is alarming and suggests that education efforts have failed to translate into improvements in widespread practice. However, training and implementation of better practices may be hindered by barriers operant at the individual or the organizational level. In this study, we conducted an analysis of perceived and/or existing barriers that potentially hinder the implementation of improved or optimal biosafety practices, according to current guidelines, in the workplace.
Methods
A series of workshops was instituted, starting in 2015, to enhance training in biosafety and biosecurity in Pakistan. The workshops were supported by the US National Institutes of Health Fogarty International Center and conducted in collaboration with the PBSA.
The first series of workshops aimed to increase awareness of biosafety among laboratory workers and researchers in 2 different cities, Karachi and Lahore, in the respective provinces of Sindh and Punjab in Pakistan.
The administrators of 8 public and 8 private clinical laboratories in each city were contacted and asked to nominate at least 2 laboratory workers each from both clinical and research biomedical disciplines. Laboratories were selected from the PBSA database. After an initial assessment of the background (public versus private setting) and work experience (in years) of each institutional nominee, a total of 64 participants were invited and registered for a full-day workshop in Karachi or Lahore.
Workshop aims included education and training focused on the following topics: introduction to good laboratory practice; biological containment levels and biological hazard groups; laboratory standard operating procedures (SOPs); training on appropriate use of personal protective equipment (PPE); protocols for cleaning spills; and recognition of potential biological exposures and laboratory acquired infections (LAIs). The workshops also included a risk assessment exercise for individual laboratories, tailored to the scope of work in that laboratory.
Barriers to Practice
Questionnaires were administered to workshop participants at the end of each workshop to evaluate perceived barriers to biosafety practices in laboratories. The questionnaires were designed by modifying the BARRIERS scale (Funk et al, 1987), 9 in which evaluators are asked to rate each specific barrier based on the extent to which it is operant in their workplace.
Since Funk et al originally designed the BARRIERS scale questionnaire to evaluate research use in nursing practice, 9 2 organizers reviewed and removed for the biosafety questionnaire in this study any items in the scale that were deemed unsuitable or inapplicable to biosafety practices. Nineteen of the original 29 perceived barriers were included in the final questionnaire. In adapting the language of the BARRIERS framework from that of nursing research to biosafety implementation, we modified the remaining 19 elements. In addition, respondents were asked to rank the 3 greatest barriers to achieving optimal biosafety practices as they perceived them. The administered questionnaire is available online as Supplementary material (www.liebertonline.com/hs/). Since barriers may exist at multiple levels in the workplace, they were divided into 4 subcategories: skills and awareness subscale; biosafety material quality subscale (with the US Centers for Disease Control and Prevention [CDC] manual, Biosafety in Microbiological and Biomedical Laboratories [BMBL] 10 as the reference guideline); accessibility subscale; and the setting (workplace) subscale. In addition, respondents were asked to identify additional barriers that were not part of the modified BARRIERS scale.
Results were entered and analyzed in MS Excel. For analysis of the BARRIERS scale, the systematic review by Kajermo et al 11 was used as a guide. Barriers reported by 50% or more of the respondents as moderate or great (score of 3 and 4 on the BARRIERS scale) are presented. Barriers reported as nonexistent (score of 1 on the BARRIERS scale) by 50% or more of respondents are also presented and examined as possible facilitators for implementation.
Results
Two full-day workshops were conducted, 1 in Karachi and 1 in Lahore, in February 2015. Each workshop was attended by 32 participants and included senior-level laboratory technologists, laboratory physicians, and microbiologists (academic and research). Of the participants, 52.5% belonged to public sector laboratories, and 47.5% were employed in private sector or commercial medical laboratories; 64% (n = 41) of participants had more than 10 years of laboratory work experience.
Barriers identified by 50% or more of participants as operant to a great extent (barriers) and to no extent (facilitators) are shown in Table 2. No barriers were identified for the guideline quality subscale, while 1 barrier each was identified in the skills and awareness subscale (little benefit for self) and accessibility subscale (implications for practice unclear). Two barriers were identified as belonging to the workplace subscale (lack of time on the job to read/implement guidelines, and lack of authority to change practice). Laboratory consultants and administrators were identified as facilitators (workplace subscale), and respondents also positively rated the biosafety guideline (BMBL) quality.
Factors identified by workshop participants as barriers or facilitators to optimal biosafety practice
Participants suggested action items to improve implementation of optimal biosafety practices. These items included: dedicated time for education and implementation of biosafety practices, development and dissemination of SOPs, biosafety drills, and inspection by a government-designated regulatory body. The proportion of participants identifying these factors as barriers is shown in Figure 2.
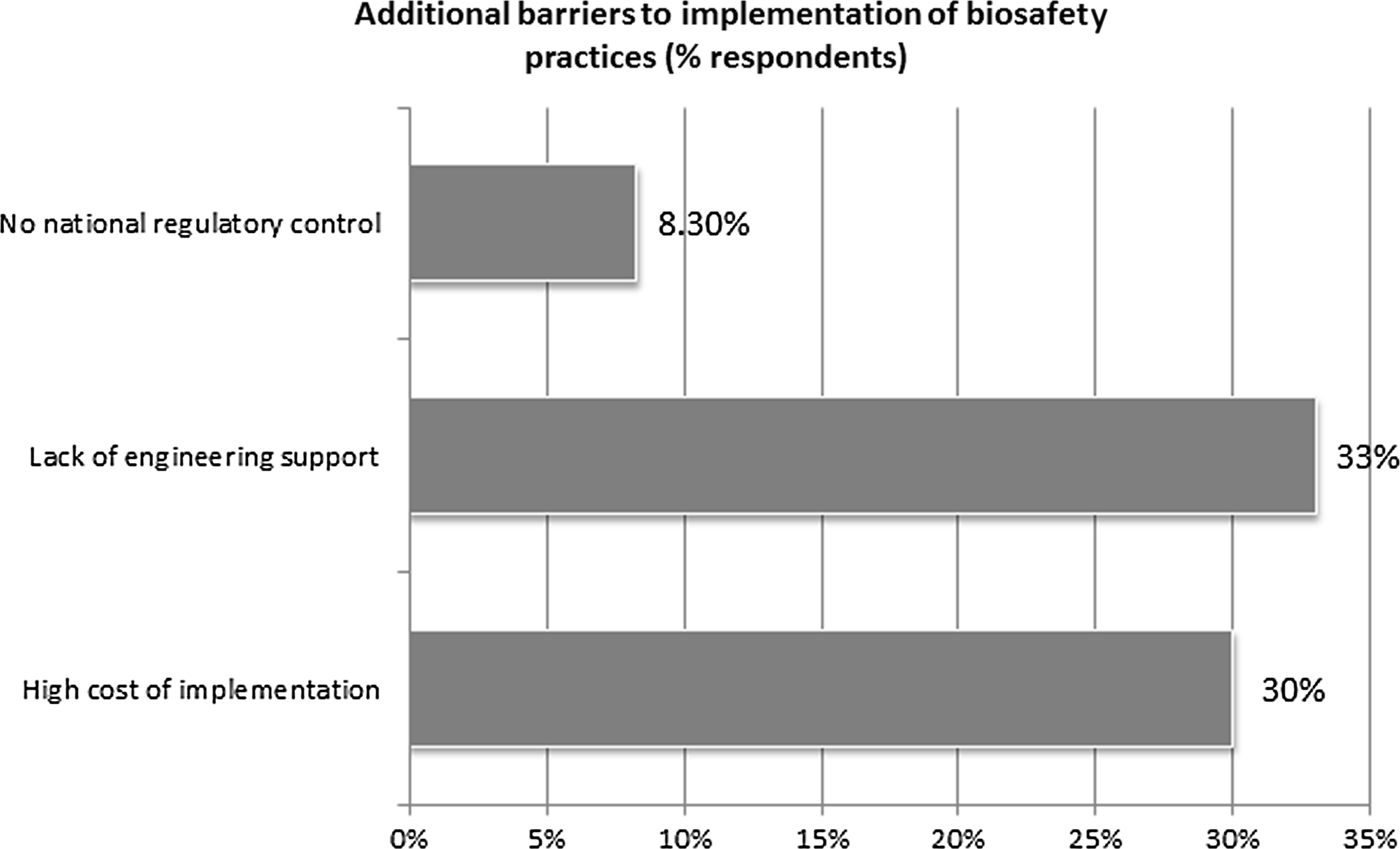
Additional barriers to implementation of biosafety practices as identified by participants in response to open-ended questions. Bars show percent of participants recognizing identified factors as barriers.
Discussion
Medical laboratory professionals play a critical role in health care through leading diagnostics. However, their safety and occupational health are sometimes sidelined in favor of concerns related to direct health care of patients, such as infection control and antimicrobial stewardship. Such oversight is especially pronounced in resource-limited countries.
Despite concerted training efforts, biosafety practices still remain far from satisfactory in Pakistan. The BARRIERS scale identified the following barriers to implementation of laboratory biosafety in Pakistan:
• There is perceived insufficient support in the workplace to the laboratory worker for introduction and improvement of practices, according to the survey. The key areas identified from the survey included: not enough time allowed for education, implementation of new practices, or SOP development; insufficient engineering support; insufficient provision of personal protective equipment; and lack of staff empowerment. • There is a perceived lack of regulatory oversight of biosafety practices, according to the survey. Establishment of a regulatory body to oversee safety and security in biomedical laboratories is required. • There appeared to be a perception among the attendees that the field of laboratory biosafety does not present any career opportunities for laboratory workers. • There is an ongoing lack of overall biosafety awareness, although the gap is closing.
Participants identified multiple barriers among the workplace subscale: no time on the job to read or receive additional education or training, no time available to implement a new practice, lack of authorization to change practice in line with recommendations, and little benefit to self (indicating a lack of lucrative career opportunities in the field). Perceived problems with administration and laboratory consultant cooperation affected implementation to a lesser extent than the aforementioned factors. Laboratory staff also indicated high rates of unawareness (on the awareness subscale) and felt that there was a lack of use of risk assessment and other biosafety skills.
Among additional barriers identified by participants, further factors identified also suggested workplace limitations. These factors included lack of engineering support in the laboratory (eg, to operate and troubleshoot biosafety cabinets, autoclaves, etc), lack of national or provincial regulatory control, and high cost of implementation of biosafety regulations.
Identification of workplace factors as one of the strongest influences on biosafety practice suggests that laboratory capacity building and engagement of laboratory administrators as stakeholders in improving practice are essential. As also suggested by some participants, government-initiated programs and regulatory bodies performing audits of biosafety practices are required.
This survey is a unique example of implementation science as applicable to laboratory biosafety in a developing country scenario. Barrier factors and facilitator factors identified here can serve as motivators for organizations looking to improve biosafety practices in their institutions. 12 We recommend a reevaluation of biosafety practices regularly to assess the impact of ongoing education and training activities.
Footnotes
Acknowledgments
This work was supported by Grant Number 3D43TW007585-07S1 from the United States National Institutes of Health Fogarty International Center. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. The authors have no conflicts of interest.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.