
Abstract
Potential terror events such as “dirty bombs” could have significant public health effects, but little is known about how low-literacy populations perceive dirty bombs, their trust in public health or government officials to provide credible information, and their willingness to comply with recommended actions. We surveyed 50 low-literacy adults from a large urban center; they were mostly members of ethnic minority groups. We used unique social marketing methods—perceptual mapping and vector message modeling—to create 3-dimensional models that reflected respondents' knowledge of what a dirty bomb is, their intended behaviors should one occur, and their concerns about complying with “shelter in place” recommendations. To further understand individual variations in this at-risk group, a k-means cluster analysis was used to identify 3 distinct segments, differing on trust of local authorities and their emergency response, willingness to comply with emergency directives, and trust of information sources. Message strategies targeting each segment were developed to focus on concepts important to moving the groups toward a “shelter in place” behavior, revealing key differences in how best to communicate with risk communication. We discuss how these methods helped elucidate specific differences in each segment's understanding of and likely response during the event of a “dirty bomb” and how these techniques can be used to create more effective message strategies targeted to these groups.
Potential terror events such as “dirty bombs” could have significant public health effects, but little is known about how low-literacy populations perceive dirty bombs, their trust in public health or government officials to provide credible information, and their willingness to comply with recommended actions. The authors surveyed 50 low-literacy adults from a large urban center, most of whom were members of ethnic minority groups. They discuss how the techniques they used can help to create more effective message strategies targeted to these groups.
E
Barriers may also be magnified for vulnerable populations, particularly individuals with low literacy. A review of 50 websites containing information on disaster or emergency preparedness found that the average reading level of the sites was a US grade of 10.74 (considered upper-level secondary school in other countries, ages 15 to 16), despite most criteria indicating materials should be written at a 6th-grade reading level or lower (considered junior level, ages 10-11). 18 The sites also had an average score of 48% on the Suitability Assessment of Materials instrument, which evaluates graphics, layout, and cultural appropriateness of materials, implying below average suitability. Most notably, sites on pandemics and bioterrorism were the most difficult to read and least suitable for people with low literacy skills. 18 In a study conducted by Wray et al, 15 participants of any literacy level preferred messaging that provided clear and accurate information and concrete action steps that were simple and consistently presented; people were often confused by terms and messages used in current government communication efforts (eg, “shelter in place”). 15
Our study aimed to investigate how low-literacy adults living in a large Northeastern city in the United States, many of whom are ethnic minorities, perceive “dirty bombs,” using unique social marketing methods: perceptual mapping and vector message modeling. These techniques produce 3-dimensional perceptual models that reflect respondents' knowledge of what a dirty bomb is, their intended behaviors should one occur, and their concerns about complying with “shelter in place” recommendations. To further understand individual variations within this at-risk group, a k-means cluster analysis was used to identify segments in this population. Given these segments, message strategies targeting each segment were developed, based on their trust of information and its sources, including both local and national authorities. We discuss how these methods helped elucidate specific differences in each segment's understanding of and likely response in the event of a “dirty bomb” explosion and how these techniques can be used to create more effective message strategies targeted to these groups.
Background
The widespread availability of radioactive material in nuclear, industrial, and medical facilities, and the lapses in programs regulating these materials, has made the acquisition of radioactive materials for making “dirty bombs” possible. 19 The Occupational Safety and Health Administration has acknowledged that many sources of radioactive material around the world are not securely housed or are not accounted for, thereby providing opportunity for terrorist groups to obtain the materials for building dirty bombs. 20 The National Nuclear Security Administration (NNSA), in the US Department of Energy, has acknowledged that current safeguards are becoming outdated and insufficient. NNSA therefore strives to improve accounting measures for radiologic materials and put improved physical protections in place to diminish the vulnerability of radiologic materials. 21 However, more than 100 incidents of theft or other unauthorized activities involving nuclear and radioactive material are reported to the International Atomic Energy Agency (IAEA) every year. 22 Recently, speculation that radioactive material has disappeared in Iraq has brought this concern to the forefront of the fight against terror. 5 Clearly, the threat posed by radiological terror events is real.
Public trust and confidence in the authorities charged with public safety—national and local governments, police and fire personnel, public health workers—is critical to improving the effectiveness of the response during a terror threat. 23 Risk communication is important for improving decision making among individuals and groups.24,25 While it is unknown how the public would actually respond in the event of a radiological terror event, evidence from non-terror radiation events, such as the 2011 Fukushima nuclear accident, indicates that credible and trusted information is needed to address the significant social and psychological impacts that would occur. 26 Because of the fear of an unseen and unknown threat such as radiation, the public may be confused and have uncertainty which, without clear communication that is acceptable to all groups, may result in the public's being unable to act in ways that are protective of themselves and their families. 27 In addition, the public in general has low knowledge of radiological terror events and “dirty bombs,” which can make communicating either before or during an event critical.28,29 However, individuals with low literacy are at higher risk of not understanding the information presented to them and of making a decision that could negatively affect their health. When combined with the lack of trust of authorities that has been seen in urban minorities (eg, Hurricane Katrina),16,30 risk communication is particularly challenging with high-risk, high-outrage radiological terror situations. In such situations, information processing and memory abilities are often reduced, which instigates fear and fatalism in the public.9,31
The importance of examining low-literacy populations' perceptions of and responses to radiological terror events is evident. The 2003 National Assessment of Adult Literacy, the most recent national-level assessment of literacy, revealed that 14% of adults in the United States have below basic literacy, 22% have basic literacy, and 53% have intermediate literacy, while only 12% are proficient. 32 Overall, the United States ranks 17th of 24 developed nations in literacy. 33 The National Center for Education Statistics (NCES) found that having only basic literacy was greater in urban areas (16.3%) compared to nonurban areas (13.1%). 34 In addition, low literacy is more prevalent in minority groups in the United States; while 28% of whites have below basic or basic literacy, 56% of blacks and 65% of Hispanics do, making minorities an important target group. 35 In Philadelphia, PA, the location of this study, almost half of adults have low literacy—an estimated 550,000 people; 36 within this group, 22% are estimated to have below basic literacy. Philadelphia is also quite diverse, with 55% of residents indicating they belong to an ethnic minority. African Americans and Hispanics, the largest minority groups in the city, also have the highest rates of not graduating from high school (secondary school, ages 17-18); over 16% of African Americans and 39% of Hispanics indicate they do not have a diploma. 37
While it is difficult to separate these demographic correlates to low literacy, it is clear that urban minorities are at special risk of having low literacy in the United States, and this prevalence has significant implications for communicating about emergency preparedness. Few studies, however, have focused on the unique challenges of low-literacy groups specifically to assess risk and act on emergency directives. Most assess ethnicity with education level and do not assess literacy per se.
A 1995 study 38 examined the risk perceptions of Mexican immigrant farmworkers concerning agricultural pesticides and found that those workers in the most inadequate socioeconomic positions were the least likely to take action to protect themselves, even when risk information was provided. These individuals, living in poverty with very little formal education and limited English skills, were more likely to have greater levels of pessimism about future health effects and were less confident that precautionary behaviors would be successful.
Emergency preparedness materials also may not be culturally targeted to their unique needs, including limited comprehension, language barriers, and lack of access to information, resources, shelter, and transportation.39-45 Racial and ethnic minorities are, in fact, more vulnerable to disasters because of socioeconomic differences, language barriers, minority preference for information sources, and distrust of government authorities.46,47 A survey of New York residents 1 year after the September 11 attack found African Americans and Hispanics and those with less education and income had high fear of subsequent attacks and were most likely to say they would flee the area, even if police or health officials advised them not to. 48 While literacy was not assessed or used in the analysis, because of the connection of literacy with race and education levels, similar results may be found in those with low literacy.
Four studies on perceptions of radiological terror events have been published, only one of which assessed perceptions of those with low literacy. The Centers for Disease Control and Prevention (CDC) published research on public perceptions of radiological terror events and risk communication messages in the United States, which involved numerous qualitative focus groups conducted with geographically and demographically diverse populations. 49 While the findings did recognize that many radiological and nuclear terror emergency information sheets and terms can be confusing and unclear, the study did not specifically examine the perceptions of low-literacy individuals. Additionally, Rogers et al 50 and Pearce et al 51 examined the perceptions of individuals in the United Kingdom and Germany concerning radiological materials and attacks in order to then create and test informational leaflets and videos. Results indicated that targeted communication geared toward complying with recommended behaviors could be improved with pretested messages, but again literacy was not assessed. Only 1 qualitative study has examined knowledge of and intended actions in a radiological terror event with low-literacy adults, 28 so little is known about the differences this group may exhibit in regard to risk perception and trust of authority, representing a significant gap in the literature. This study aimed to address this gap.
Methods
Study Design
This study included a multiphase protocol. In Phase I, focus groups were conducted with limited literacy individuals (N = 30 with ≤6th-grade reading level) to inform the design of a survey instrument to assess perceptions of a dirty bomb terrorist event. 28 The survey instrument was developed in Phase II and administered to 71 individuals at risk for low literacy. Results of this phase were then used to develop a low-literacy risk communication decision aid about dirty bomb radiological terror events and tested in a pilot randomized controlled trial. This review discusses the results of Phase II and how these outcomes were used to develop messages for use in the Phase III decision aid.
Phase II was a cross-sectional intercept survey, with recruitment occurring in a variety of community-based sites in north Philadelphia, including the General Internal Medicine Clinic at Temple University Hospital, neighborhood youth and senior community centers, and supermarkets. Potential participants were approached by study research assistants to assess interest in participating in the study. If the potential participant was willing, the research staff reviewed the informed consent, provided a brief tutorial on what a dirty bomb is, screened for literacy, and then administered the survey. Surveys were read aloud by the research assistant, who asked the participant to respond by pointing to a graphic scale that rated how much they agreed or disagreed with each of the statements on a scale of 0 to 10 (strongly disagree to strongly agree). The graphic scale is used widely in clinical settings to assess pain, particularly in populations with limited literacy.52,53 It consists of “faces” at the major scale points, ranging from strongly frowning (0) to strongly smiling. 53 This scale was printed on an 8 ½” × 11” sheet and positioned so that the participant could point to the “face” that best represented his or her response. If a participant needed clarification, the research assistant was trained to clarify without leading or potentially biasing the participant's responses. Surveys took approximately 15 minutes to complete, and participants received a $10 gift card to a local store and 2 public transit tokens as an incentive. All materials and procedures were approved by the Temple University Institutional Review Board.
Study Participants
Criteria for inclusion included being age 18 or over and having the ability to read, understand, and sign the consent to participate in English. The consent was written at a 6th-grade reading level, and, to ensure participants' understanding, research assistants read the document out loud. All participants were screened for literacy using the standardized REALM-R. 54 This instrument, a shortened version of the REALM, is highly correlated with other standardized reading tests (Peabody Individual Achievement Test-Revised, r = 0.97; Slosson Oral Reading Test-Revised, r = 0.96; Wide-range Achievement Test-Revised, r = 0.88). 54 It measures a participant's ability to read 11 common medical words, 8 of which are scored. Based on the validated scoring scheme of the instrument, participants unable to pronounce the first 3 words have very low literacy skills, and those unable to pronounce more than 6 words are at risk of having inadequate literacy. 55 A score of 6 corresponds to a 6th-grade reading level; 55 thus, for the purposes of this study, respondents had to score a 6 or below on the REALM-R to be considered at risk for low literacy. Survey data were collected from 71 individuals, 50 of whom met the criteria for low literacy. The analysis includes only those 50 low-literacy participants.
Instrumentation
The perceptual mapping survey tool was developed to reflect the 4 major themes presented in the focus groups in Phase I:
1. General knowledge of and assessment of dirty bombs; 2. Planning for emergencies and how planning might affect or mitigate a dirty bomb; 3. Response to information sources during a dirty bomb and preferred information providers; and 4. Trust of information sources, beliefs about how government would respond, and types of information wanted if a dirty bomb occurred.
28
Based on results, survey items included perceived barriers and facilitators to complying with radiological terror event recommendations and were placed in 4 groupings of conceptually related statements:
• Group 1: Statements (n = 17) centered on knowledge of a dirty bomb, trust of information sources if a dirty bomb occurred, and need for information about who was responsible for the event. • Group 2: Statements (n = 10) focused on action intentions (staying home vs leaving; getting children or family), belief in general preparedness, and preparedness activities, such as having an emergency plan, food, and water. • Group 3: Statements (n = 10) focused on what respondents would be worried about in the event of a dirty bomb, such as safety of food and water, risk of illness, breathing radiation, and its effects on and risks to children and pets. • Group 4: Statements (n = 12) that assessed participants' perspectives of how likely a dirty bomb is to occur; the likelihood of this event occurring compared to other threats (eg, violence, flooding, or a car accident); beliefs about the trustworthiness of local, state, and federal authorities; and whether their neighborhood would be treated fairly in response efforts.
In addition to the above, basic demographic questions were included in the survey to capture sociodemographic characteristics. These included age, sex, race, and education level. Literacy level was also captured, as described above. The instrument followed a format consistent with that used in other studies we have conducted with low-literacy populations.56,57
Data Reduction and Cluster Analysis
A k-means cluster analysis was conducted, producing 3 distinct clusters or segments. After the participant subgroups were named and defined, descriptive statistics were computed for all survey items. An analysis of variance was performed in order to compare perceived barriers to compliance with shelter in place recommendations across the 3 subgroups. To reduce the data for processing in the perceptual maps, a factor analysis of the 49 items from the survey was conducted. Varimax rotation with Kaiser normalization was used, and survey items with eigenvalues >1 were extracted. 58 Based on this, and a review of relevant concepts to include in the perceptual maps, survey items were analyzed for consistency. Variables were recoded to combine statements that loaded at a 0.5 level or above or were decided to be important to understanding the analysis. This analysis resulted in 10 perception variables and 2 action-related variables. The perception variables were named: (1) trust authority information, (2) trust authority response, (3) confidence in knowledge of “dirty bomb,” (4) need to know who is responsible, (5) distrust in authority, (6) family and pet concerns, (7) radiation concerns, (8) anti-compliant behavior, (9) believe I am prepared, and (10) know what to do. The 2 action variables were: (1) I would stay inside and (2) I have an emergency plan. All analyses were done using SPSS version 23.0.
Perceptual Mapping and Vector Message Modeling
Once data were reduced and segments established, perceptual mapping techniques were used to model how participants conceptualized the relationship among the 10 key perception variables and 2 action variables. Vector message modeling was then used to identify appropriate risk communication messages for each sample segment.
Perceptual mapping uses multidimensional scaling analysis to produce a graphic display of how participants perceive the relationships among the set of elements by modeling the similarities and dissimilarities as distances between points in a multidimensional space. The resulting maps display the risk/benefit elements relative to each other and to “self,” which can be an individual or group average. Perceptual mapping thus provides a graphic representation of how respondents conceptualize the decision or situation being evaluated. These methods are used extensively in marketing and advertising and have been used to evaluate a number of public health decisions by the authors. (For further in-depth information on these methods, see: https://sites.temple.edu/turiskcommlab/).57,59-61
To construct the perceptual maps we used Cogniplot, a software program the authors developed based on the multidimensional scaling program Galileo. 62 Survey data were rendered in distance matrix form for input into Cogniplot. The program produces the maps or models as n-dimensional rigid structures. To produce a coordinate frame around the structure for referencing purposes, the program uses a simple component factor analysis. Thus, the model can be seen to exist in an X-Y-Z coordinate space, making it easy to refer to the location of any given point (concept), including the “self.” The factoring process also produces eigen values for each factor, which provide a “variance explained” index. Thus, the total variance explained by a particular 2- or 3-dimensional model can be determined. The survey data were then entered into SPSS version 23 to generate inter-item correlation coefficients. The correlations, based on the total sample, were then converted to a 0-10 scale for processing through the perceptual mapping software. The resulting 3-dimensional maps for each segment are presented in Figures 2 through 4.
Vector message modeling was then used to identify optimum message concept combinations for changing the positioning of elements in the mapping display (ie, changing the perceptions/attitudes of the target segment). In order to move an individual or concept/attribute in the perceptual space to a more desired position, decision, or behavior, communication messages that emphasize the optimum associations must be created. After the perceptual map was produced to display the relationships among concepts and between the concepts and “self,” vector modeling was used to determine which element or elements would have to be emphasized in a message or intervention design to “move” the group toward the desired behavior—in this case, to shelter in place in the event of a dirty bomb. This behavior is the target vector. By identifying the target vector message and the number of elements to be included in the message, the software created all possible vector resolutions, rank ordered according to best fit to the target vector. The “best fit” solution was evaluated by the research team for conceptual consistency and practicality and then applied to the development of the literacy appropriate decision aid.
Results
Participant Characteristics
Participants self-identified as 80% African American, 14% white, 2% Hispanic, and 4% mixed race (Table 1). Our respondents were composed of more women (n = 29) than men (n = 21), with a mean age of 43.2 years. In terms of education, 34% (n = 17) had completed less than high school, 46% (n = 23) had graduated from high school or earned a GED, and 20% (n = 10) had vocational training or some college. Two respondents (4%) indicated they had a “graduate degree” but scored as “low-literacy” on the REALM-R. Table 2 shows overall means and standard deviations for the 10 combined items used in the analysis. The group indicated moderate distrust of authority (mean 5.92 out of 10) and their response (mean 6.19 out of 10). Notably, most believed they knew what to do if a dirty bomb exploded (mean 7.90 out of 10) but had moderate agreement with anti-compliant items, such as leaving the house and going to get family or friends (mean 4.65 out of 10).
Demographic Characteristics: Total and by Segment
Overall Means for Cluster Analysis
0-10 scale.
Cluster Analysis
Three distinct segments emerged from the cluster analysis, labeled (1) trust information, not response; (2) distrust information and response; and (3) trust local, not “global.” As Table 2 illustrates, the “trust local, not global” segment is the largest, containing half of the sample (25 respondents). The “trust information, not response” segment is next largest with 32% (16 respondents), and the “distrust information and response” segment comprises 18% (9 respondents).
For the “trust local, not global” segment, the majority of individuals are between 18 and 50 years old, most (88%) are African American, most (60%) are female, and 44% are high school graduates. The “trust information, not response” segment shows a different age profile, with individuals divided between the youngest and oldest categories: 43% are young, between the ages of 18 and 35, while 25% are 65 years and older. Over two-thirds are female (68%) and have a high school diploma (43%), while almost 19% are white. In the “distrust information and response” segment, the distribution among age categories is fairly even, with 22% being 65 years and over, and 33% between 50 and 65 years of age. The majority is African American (78%) and male (66%); 44% are high school graduates (Table 1).
ANOVA analyses were done by comparing the 3 segments on the 10 perception factors and the 2 actions/behaviors of interest (staying inside and having an emergency plan). Means and significance levels are displayed in Table 3. As noted, significant differences are seen among clusters in a number of different variables, including trust of authority's information and responses, confidence in knowledge of dirty bombs, and distrust of authority. Based on these differences, means were plotted graphically to better understand the key areas of differentiation across segments (Figure 1).
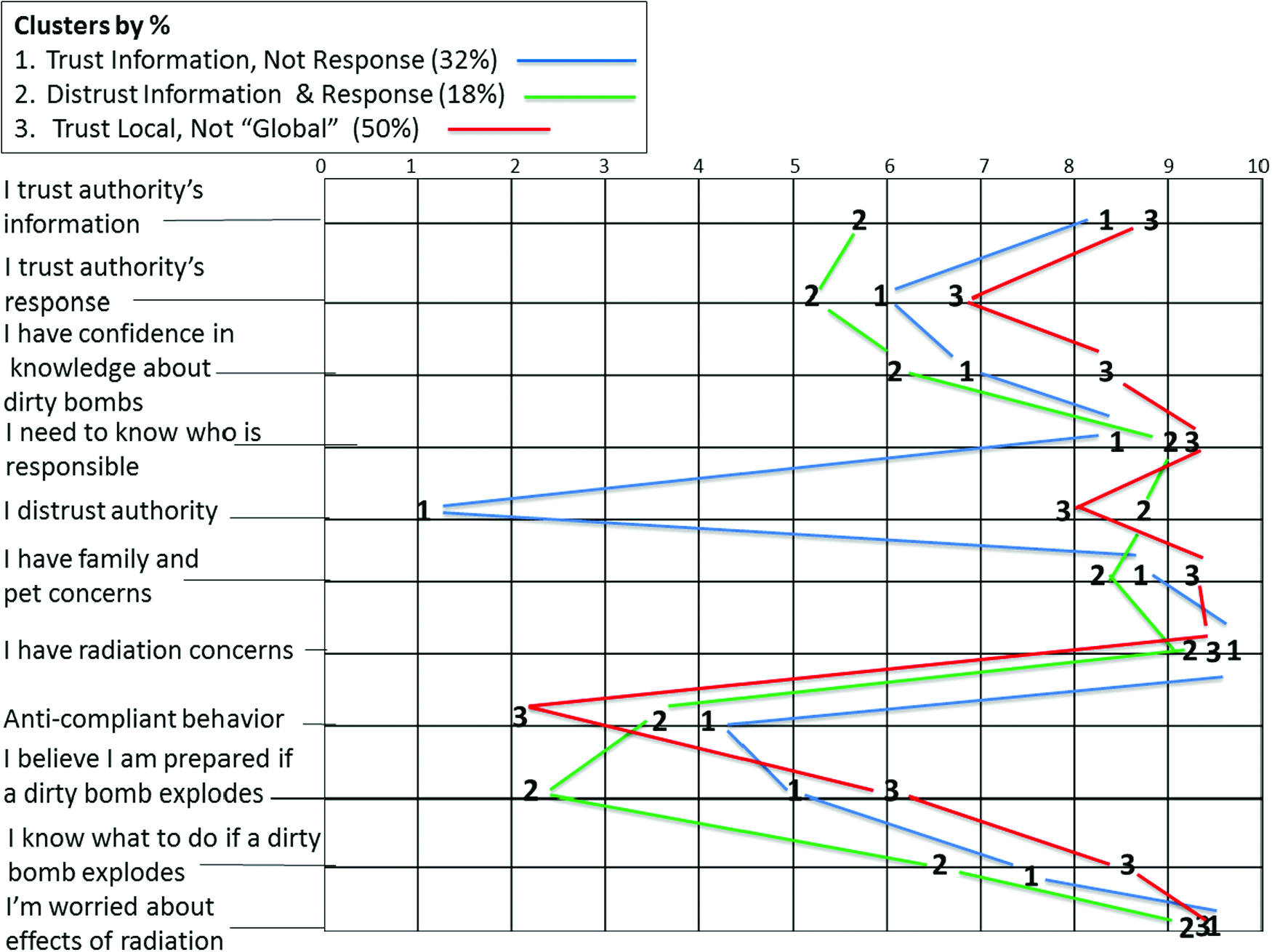
Mean Plot by Segment Group. Color graphics available at www.liebertonline.com/hs
ANOVA Analysis by Segment Group
≤.05; **≤.000
Perceptual Mapping
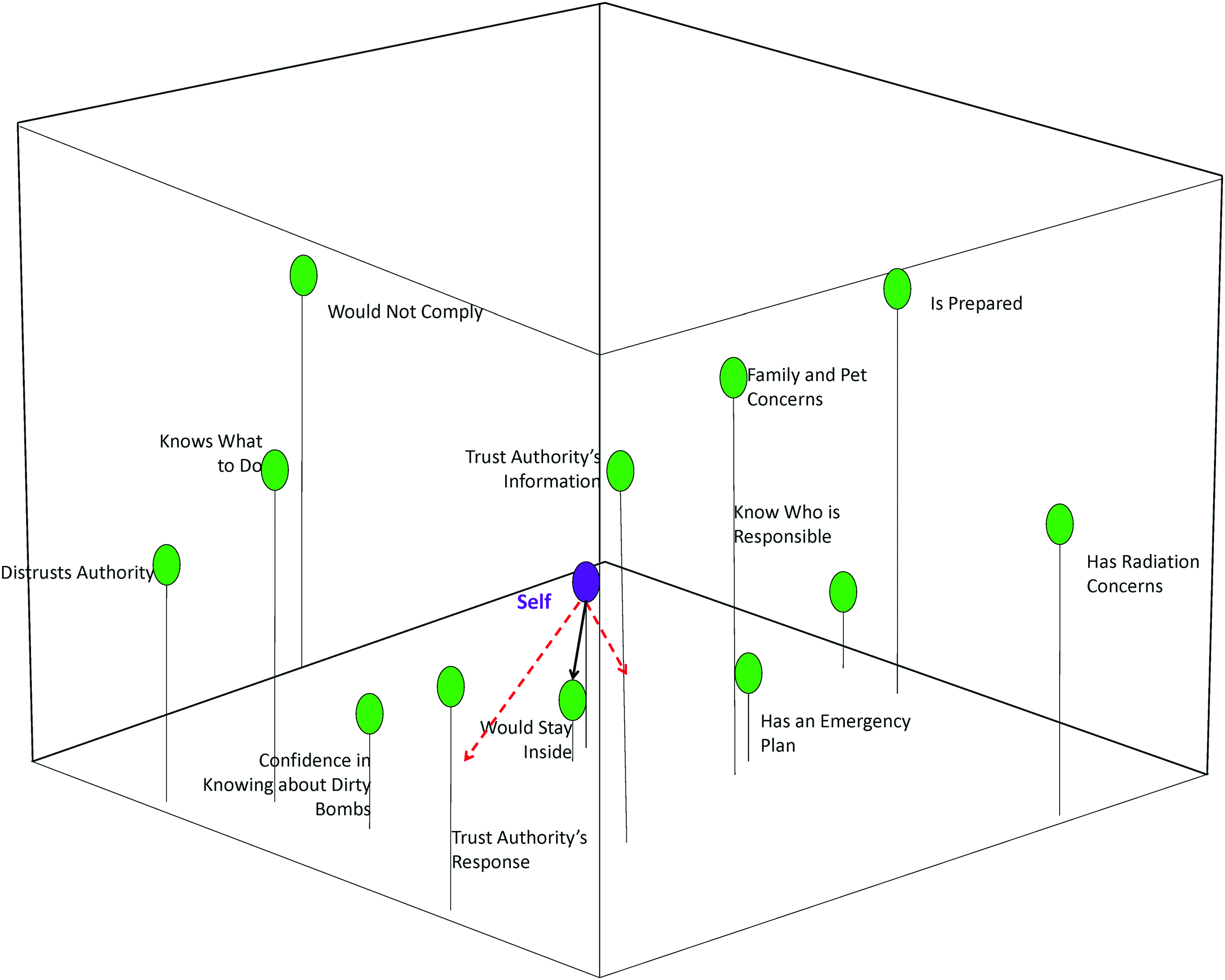
The perceptual mapping software produced 3-dimensional maps displaying the composite variables in relation to self, the group mean of each segment. Figure 2 displays the relationship of factors for the “trust information, not response” segment. This group conceptualizes “knows what to do” and “confidence knowing about dirty bombs” together, but few variables are close to “self.” The action variable of “stay inside” is far away from the group, meaning this directive has little resonance for them. Figure 3 displays the factors for the “distrust information and response” segment. This group is most likely to comply with shelter in place directives, as noted by the close distance of the variable to self. They do not see any of the other variables as close to them and seem to be the least likely to be concerned about radiation concerns or distrusting of authority. Figure 4 displays the factors for the “trust local, not global” segment. This group is also relatively far away from the “stay inside” variable and is most likely to have family and pet concerns. Few of the variables group together, meaning this group is not conceptualizing them as similar in nature.

Perceptual Map with Message Vectors to “Stay Inside,” Segment 1 (32%): Trust Information, Not Response. Color graphics available at www.liebertonline.com/hs
Perceptual Map with Message Vectors to “Stay Inside,” Segment 2 (18%): Distrust Information and Response. Color graphics available at www.liebertonline.com/hs
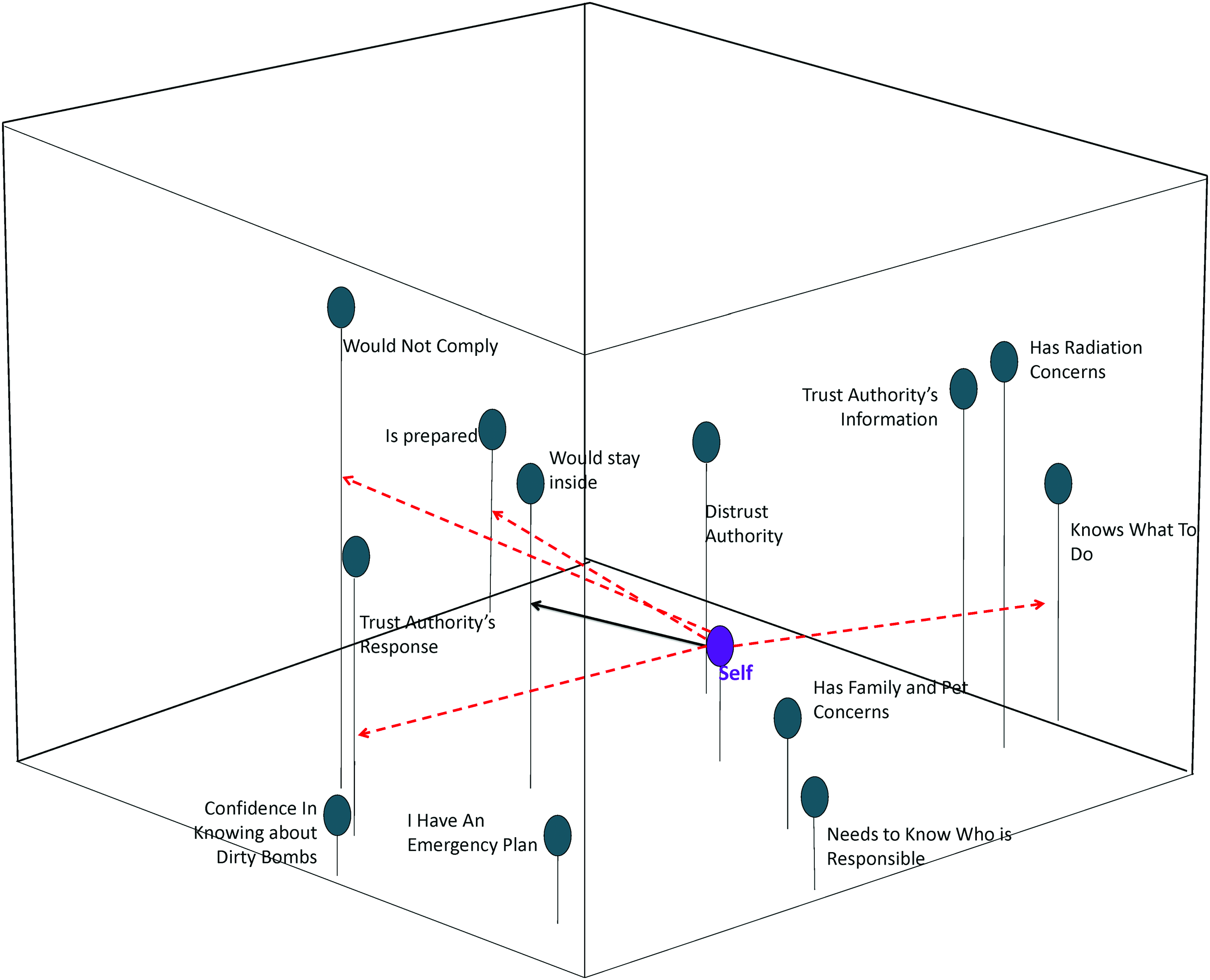
Perceptual Map with Message Vectors to “Stay Inside,” Segment 3 (50%): Trust Local, Not Global. Color graphics available at www.liebertonline.com/hs
Vector Message Design Analyses
The vector analysis is denoted by the solid and dotted arrows in Figures 2 through 4. Based on this analysis, specific message strategies emerged to move the “self,” or segment, in the desired direction in the perceptual space. While a number of the strategies would be the same, some differences in how messages might be emphasized remain and could be used in either pre- or postevent messaging. For example, in the “trust information, not response” segment, messages that emphasize trusting both the information and the authorities' response efforts would have to be provided to pull this group toward the target behavior of “stay inside.” It would also be important to stress why complying with emergency directives is in their and their families’ best interest. In addition, messages that modulate that they know what to do (meaning that they think they know more than they do) and feeling that they are totally prepared would need to be emphasized. In this case, providing messages that increase feelings of risk may be needed to counteract this segment's feelings of confidence about knowing how to respond. Because of their designated likely response to a dirty bomb explosion, it would be important to emphasize messages explaining why staying inside is the appropriate response and why trusting authority information will be critical.
The “distrust information and response” segment was the most distrustful, yet, as can be seen in Figure 3, they recognize the importance of “staying inside” by positioning it very close to “self.” In this case, it would take little to convince this group to comply with sheltering in place recommendations. As such, messages could emphasize trusting authority information and the authority's response and deemphasize needing to know who is responsible for the bombing.
Finally, the “trust local, not global” segment is similar to the “trust information, not response” segment in that “staying inside” is far from the “self.” In this group, it would be important to emphasize messages about being compliant to authority information, trusting the authority's response effort, and being prepared in an emergency. In order to move this group toward sheltering in place, messages would need to modify this group's belief that they know who is responsible for the attack and their perception that they know what to do in the event of a radiological terror event in order to adequately move them in the space toward sheltering in place.
Discussion
This analysis provides a look at how urban, mostly minority adults with low literacy conceive of a dirty bomb and how they might respond should an explosion occur. Importantly, we were also able to discern differences within this sample to examine unique perceptions about what they feel they know about a dirty bomb, what they would be most concerned about, and their intended actions. The unique segments identified show differences in levels of trust of information provided, trust of local authorities and the anticipated response of those authorities, and different levels of confidence in knowing what to do during a radiological terror event. These differences were then further elucidated by using perceptual mapping and vector message modeling to create specific, targeted message strategies for each segment. These methods can then help researchers understand how to “move” individuals within the perceptual space toward the desired decision or attitude. This can help develop message “parsimony,” by focusing only on those variables most important to the desired change, rather than employing the “kitchen sink” method of message/intervention development. If too many concepts are emphasized, the true motivators for change may get lost in a message or intervention that is too complicated. While the process of crafting the messages and interventions remains subjective, vector modeling methods provide an empirical basis on which to select message elements to include that are most likely to improve outcomes. In this study, the target vector was sheltering in place, indicating the need to “move” individuals in each of the segments toward being more accepting of emergency directives. Results can then be used to create highly targeted interventions.
The limitation that low literacy brings to the widespread distribution of emergency response directives is clearly a significant barrier. Literacy studies suggest that one-third to one-half of the US population has some difficulty using written materials, 38 such as those available on the CDC website—materials that have been measured at an 8th-grade reading level or higher.39,40 Because of the serious consequences of exposure to a dirty bomb, it is important that disaster planning and management teams address the accessibility of risk communication materials designed for limited-literacy groups, so that everyone will have equal access to potentially life-saving information.
This limitation may also be exacerbated in urban centers with large minority populations. Studies indicate that these groups are also most at risk for low literacy and have general distrust of authorities (defined in this study as police, firefighters, local and national government, public health agencies, etc). Emergency planners will need to think creatively about how to deliver information in accessible ways that are also seen as credible by the population and that address the general distrust they may have for emergency directives. For example, the use of community spokespeople, such as local pastors, community center staff, or block captains, may be appropriate methods for getting emergency information to urban minorities who may have limited literacy.
An important finding of this study is that communication interventions, including who the spokespeople are and how the information is delivered, may need to be varied even in areas with similar population demographics. Clearly, perceptions about a radiological terror event are subjective, and risk perception may be different depending on individual characteristics, previous experiences with law enforcement, and cultural ideas about discrimination and stigma. A fairly high number of survey respondents in this study indicated that they did not trust “authority” in general (overall mean of 5.92 out of 10), including the anticipated response that would be provided in an emergency. But more important, certain groups had much higher distrust (mean 8.89 in “distrust information and response” segment and 7.96 in “trust local, not global” segments). This is an important finding for emergency planners who are looking to develop information materials and response plans. Thinking about how emergency information is provided will be key to developing trust in these harder to reach groups.
Responses to threats are often related to perceived risk and whether an individual sees that risk as serious. Risk, however, is a subjective concept, one that Slovic and Weber noted was invented to help us understand and cope with the dangers and uncertainties of life. 63 This subjectivity makes effective risk communication an especially daunting task. Risk communication must contextualize, for heterogeneous groups in the population, perceived versus actual (probability based) risks and benefits, as well as the uncertainties and ambiguities that accompany a crisis. While this risk perception can be heightened in any population, it may be especially skewed in a group with low literacy and who have other social characteristics 44 —race, income, education level—that make them more at risk for negative health effects, as well as having less access to information and resources in an emergency. In order for health and risk communication efforts to be successful, it is important to match messages to the literacy skills and cultural beliefs of the intended audience to ensure comprehension and the ability to adequately judge risks and benefits. As such, providing information about a radiological terror event and dirty bomb is further complicated by the fact that, even with the availability of material focused on this topic, the public at large does not have a good understanding of the recommended action to take in the event of a radiological terror event. 64 This was clearly evident in this study, where most respondents inflated their knowledge of what a dirty bomb is and what to do if one exploded, based on their overall agreement with the statements “I know what to do if a dirty bomb exploded” (mean 7.90), and “I have confidence in my knowledge about dirty bombs” (mean 7.48). Despite this confidence, most indicated that they would “get out of town” or “leave their house to get their children or family members,” indicating that the confidence in knowing what to do does not translate to intended behavior. This was especially true in the respondents in the “trust local, not global” segment, who indicated highest agreement with these noncompliant statements.
Overall, it will be critical in an emergency such as a radiological terror event that the needs of all population segments be adequately addressed, whether it involves literacy, cultural mistrust of authorities, race, or geographic region. Response planners must refrain from a “one size fits all” strategy, thinking that presenting information about a recommended response will be accepted and understood by all. As the results of this study show, even within a seemingly homogenous group, vast differences in understanding and intended compliance with emergency directives exist. If emergency response strategists do not think creatively about how to help the public understand and prepare for a radiological terror event, people with limited literacy will be inadequately prepared for such events.
Limitations
This study took exceptional care to identify and recruit adults from urban environments in a large Northeastern city, who were then tested to ensure that they met the study's limited-literacy criterion. Regardless of the difficulty of reaching and recruiting such individuals, the final respondent pool remains a convenience sample. As such, our results cannot be generalized beyond this study population. In addition, while the large majority indicated they were members of a minority group, 80% reported their race as African American. Although larger studies of literacy in the United States indicate that African Americans have higher rates of low literacy, it is difficult to assess if the findings are related to literacy or the racial make-up of the group.
A larger study involving more diversified settings and a larger sample size might identify a broader range of barriers and facilitators to sheltering in place during a radiological terror event, and might reveal other population subgroups not identified in this study. In addition, since the survey was orally administered, participants could have found the community settings intimidating or distracting. This may have affected the way participants responded to the questions or caused them to feel they needed to respond in a certain manner. However, because we intercepted respondents in a number of settings and did not find differences in how they answered, and oral administration ensured that respondents understood the question items, we do not believe this affected participation in this study. Questions were also closed-ended, which did not allow for respondents to clarify answers or provide nuance to their perceptions.
Another limitation involves the focus on the topic of radiological terror events. Individual responses will likely vary with different types of content (eg, what to do in natural vs man-made disasters; active-shooter vs kidnapping/ransom events; bombs at a public event vs bombing a building, etc). Public health officials will have to develop preparedness materials for these types of differences as the likely frequency of such events increases. Also, because we focused on intended and not actual behaviors, it is hard to discern how respondents would actually respond in the event of a radiological terror event and if their reported trust of authorities and the response would be low as noted by a significant portion of respondents. Some studies suggest that trust in government actually rises in crises, and our findings may not be an accurate reflection of how people will respond.65-67
Conclusion
Public trust and confidence can help mitigate and improve the ability to manage a terror threat, 24 but this is severely compromised if a large segment of the population is unable to access or process emergency communications, especially if they already have lower confidence in emergency response because of other socioeconomic factors.13,14,46 Effective risk communication is essential for containing the public's fear and fatalism and for ensuring public cooperation during crisis events. 24 However, risk communication is especially challenging when applying the messages to high-risk–high-outrage situations, 20 such as a dirty bomb, due to their capacity to produce widespread fear, which reduces complexity of information processing and inhibits memory abilities. 8 While race and education level are inextricably related to literacy, these limitations may be further accentuated in those with low literacy, as distrust may be exacerbated by use of complicated terminology that assumes the public has more information and understanding than they do, placing them at significant risk for negative outcomes. It thus becomes critical for risk communication to address the needs of all segments of the population to ensure that disparities in response and outcomes are minimized.
Footnotes
Acknowledgments
This study was funded by the National Institute of Biomedical Imaging and Bioengineering, 5RO3EB9561-2 (Health Literacy mechanism): “Developing Radiological Risk Communication Materials for Low-Literacy Populations,” Bass, SB – Principal Investigator.