
Abstract
As US public health faces increasing threats from outbreaks, impending changes to the healthcare landscape in the United States may alter the way that health departments are able to detect and control some of the most common infectious diseases. The Patient Protection and Affordable Care Act (ACA) has made significant changes in the way health care is provided in the United States. While many of the clinical, economic, and policy implications of the ACA are well described, there has been limited analysis of changes, if any, in the surveillance and control of infectious diseases of public health importance—such as tuberculosis, sexually transmitted infections, and HIV—that are anticipated or occurring as the ACA is implemented across the United States. To address these questions, we reviewed the literature for evidence of changing trends and conducted 66 semi-structured, not-for-attribution interviews with 82 participants from healthcare systems; academia; federal, state, and local public health agencies; and professional and nongovernmental organizations across the United States. This analysis identifies several ways in which ACA implementation has not fully addressed the public health needs associated with diagnosis, treatment, surveillance, and control of infectious diseases of public health importance.
The Patient Protection and Affordable Care Act (ACA) has made significant changes in the way health care is provided in the US. While many of the clinical, economic, and policy implications of the ACA are well described, there has been limited analysis of changes, if any, in the surveillance and control of infectious diseases of public health importance—such as tuberculosis, sexually transmitted infections, and HIV. This analysis identifies several ways in which ACA implementation has not fully addressed the public health needs associated with diagnosis, treatment, surveillance, and control of infectious diseases of public health importance.
O
Impending changes to the healthcare landscape in the United States may alter the way that health departments are able to detect and control infectious diseases. Signed into law in 2010, the Patient Protection and Affordable Care Act (ACA) has made significant changes in the way health care is provided in the United States. According to the Department of Health and Human Services (HHS), 20 million uninsured individuals are estimated to have gained coverage under the ACA as of March 2016. 3 As ACA implementation continues, it is possible that the percentage of uninsured Americans will continue to decrease, as nearly half of those who remain uninsured are eligible for financial assistance through Medicaid or subsidized marketplace coverage through ACA exchanges. 4
Historically, public health clinics have served as important sites for diagnosis, treatment, surveillance, and control of a number of infectious diseases and conditions (eg, tuberculosis [TB], human immunodeficiency virus [HIV], sexually transmitted infections [STIs]). Patients who present to these facilities for free medical care typically receive treatment and access to disease control information and other interventions (eg, immunization, condoms). In addition to providing services during these clinical encounters, public health departments are also able to capture demographic and disease-specific data for surveillance purposes.
As previously uninsured patients gain access to other healthcare options, some health departments anticipate that their patient load will shift away from public health clinics and toward private medical providers. This anticipated shift in the locus of care, combined with the economic downturn that began in 2008 and the changing relationship between public health and primary care, has prompted some health departments to scale back or discontinue the provision of clinical services.5,6
We sought to document current and anticipated changes in the diagnosis, treatment, surveillance, and control of communicable diseases following implementation of the ACA and to examine ways to enhance these activities. For this analysis, we focused on a subset of communicable diseases, which we dubbed infectious diseases of public health importance. We define these as the communicable diseases for which public health departments have historically played a lead role in diagnosis, treatment, surveillance, and control—including STIs, TB, and HIV. Each of these diseases is of national public health importance; they represent leading causes of morbidity in the United States and have the potential to cause outbreaks that spread across state lines. Additionally, poverty and limited access to health care are important risk factors for these diseases, making them ideal candidates for examining the impacts of the ACA with respect to infectious disease surveillance and control. The goal of this analysis is to provide public health departments, clinicians, and policymakers with information to help them gauge the impact of ACA implementation on surveillance and control of infectious diseases and develop plans for effectively responding to these changes.
Methods
We conducted a review of relevant literature, covering a range of subjects pertinent to the ACA and its impact on infectious diseases. We identified articles from the peer-reviewed literature, nongovernmental and professional organization research and publications, and government documents, as well as opinions and commentary from recognized experts discussing topics such as the shift in locus of care from the public to the private sector; initiatives and funding for public health and health care; changes to public and private health insurance access, affordability, and coverage; payment and reimbursement reform; Accountable Care Organizations (ACOs) and patient-centered medical homes; and remaining barriers to healthcare access and gaps in insurance coverage. Additional research included reviews of existing healthcare and public health programs, such as the Ryan White HIV/AIDS and Title X Family Planning programs. In addition to highlighting key issues with respect to infectious disease surveillance and ACA implementation, the literature review aided us in identifying key professional organizations, state and local public health agencies, practitioners, and policymakers with expertise in specific areas of interest to our research.
We conducted 66 semi-structured interviews with 82 participants from healthcare systems; academia; federal, state, and local public health agencies; and professional and nongovernmental organizations. Participants represented diverse geographic, economic, and demographic entities and have broad expertise in ACA implementation and control programs for communicable diseases. Participants are listed in Appendix A and mapped in Figure 1. Interviews were conducted on a not-for-attribution basis to promote candid and honest responses. Because of the politically sensitive nature of the subject matter, the interviews were not recorded or transcribed. Instead, a member of the study team served as a dedicated note-taker and captured main points raised by interviewees during each call. After each interview, the research team reviewed the interview notes and distilled the comments into themes.
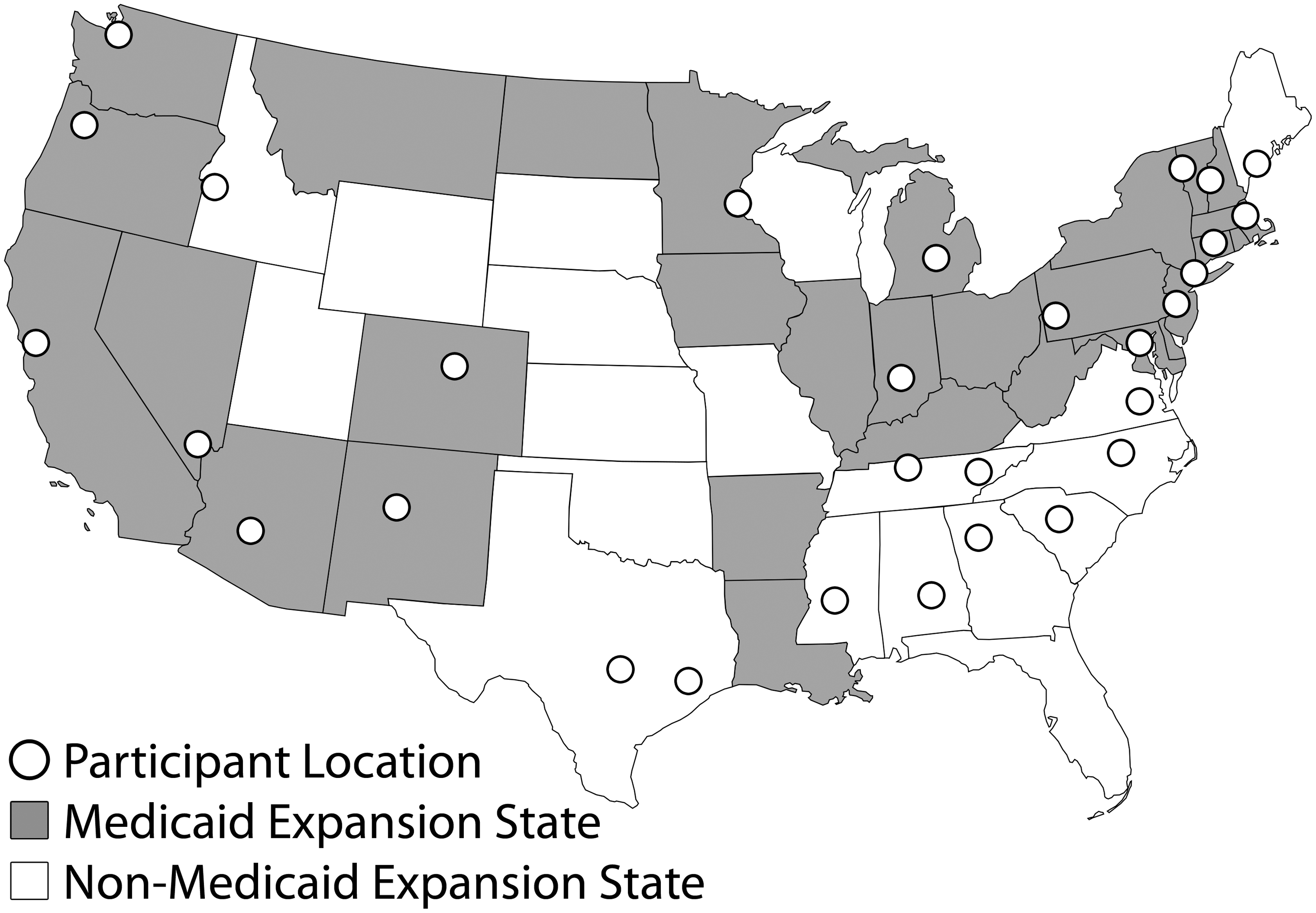
Geographic Distribution of Study Participants
At the completion of the interview process, we synthesized the findings from the review of pertinent research and the themes that arose during the expert interviews. To ensure that the analysis of the literature and expert interviews was accurate, we asked a subset of the interviewees to provide peer review of the findings and recommendations; we received peer-review comments from 11 participants (noted in Appendix A).
This article represents the synthesis of information obtained during our analysis of the literature and expert interviews. The recommendations included in this report are not intended to represent consensus views of all of the participants.
The University of Pittsburgh Institutional Review Board designated this study as “exempt” under section 45 CFR 46.101(b)(2).
Findings
Public Health Departments Will Likely Remain an Important Player in Providing Safety Net Care Under the ACA
Along with federally qualified health centers (also called community health centers) and public hospitals, state and local health departments have historically been important components of the healthcare safety net, providing a wide variety of clinical services to high-risk, underserved populations. The types of services provided vary considerably between jurisdictions and can include dental care, maternal and child health services, and infectious disease screening and treatment. Services in the last category are provided by a majority of local health departments nationwide. 7
Despite expanded insurance coverage under the ACA, significant barriers to care persist that may require health departments to retain or even expand their provision of clinical services. First, while the ACA has extended health insurance coverage to millions of Americans, more than 28.5 million people in the United States remain uninsured, including millions of individuals who are uninsurable because of their immigration status. Additionally, Medicaid expansion under the ACA was originally intended to apply nationally; however, a 2012 Supreme Court decision made implementation optional for states. 8 To date, 19 states have elected not to expand Medicaid. 9 As a result, 2.5 million Americans fall into a “coverage gap,” with income too high to qualify for Medicaid but not high enough to qualify for subsidies intended to defray the cost of purchasing insurance. 4 Considering the link between factors such as immigration status, poverty, and poor healthcare access and the risk for infectious diseases of public health importance, ensuring the continued availability of safety net care for uninsured individuals should remain a public health priority.
Even insured individuals may still encounter barriers to care. Many insurance plans, particularly those on state exchanges, have high cost-sharing requirements, such as deductibles and copayments, that can be financially burdensome for some patients. 10 In some cases, limited availability of private medical providers may make it difficult for insured individuals to have access to care. Some states, for example, have an insufficient number of providers who accept Medicaid to accommodate newly insured populations. 11 Additionally, rural and frontier populations often have decreased access to healthcare providers and may have to travel long distances for care. In these areas, state and local health departments may play an outsized role in providing clinical services.
Regardless of their insurance status, some patients demonstrate a preference for the type or quality of care provided by health department clinics. Several study participants reported that patients may elect to seek care at public health clinics because clinicians in these environments are experienced in providing nonjudgmental and culturally appropriate care for patients with sensitive conditions like STIs. Privacy concerns may also play a role. For example, study participants cited a greater degree of anonymity at public health clinics compared to other clinical options (eg, seeing a family doctor), which may make it easier for patients to disclose and discuss high-risk behaviors or sensitive medical conditions such as STIs or HIV.
Public Health Needs to Work with Private Medical Providers to Ensure that Patients Receive Appropriate Care
The availability of a broader set of resources in the private sector, along with patients' ability to obtain comprehensive primary care, offers great promise for enhanced care of patients with infectious diseases of public health importance in this healthcare environment. Increased recognition of the relationship between comorbidities like mental health and chronic medical conditions on clinical outcomes for patients with infectious diseases supports embedding treatment of these diseases in patients' medical homes. The comprehensive care that patient-centered medical homes are capable of providing can simultaneously address multiple aspects of patient health to improve overall outcomes. Conversely, publicly funded clinics have historically been the primary location for prevention and control of infectious diseases of public health importance in the United States.12,13 As patients are expected to shift to the private sector, numerous study participants expressed concern about private medical providers' limited experience in diagnosing and managing patients with infectious diseases of public health importance.
With respect to HIV, many study participants expressed hope that care for HIV patients will be maintained or enhanced under the ACA. Patients with HIV are typically treated by specialty providers, and it is expected that this trend will continue. Expanded insurance coverage is expected to increase the number of people seen by these providers as well as the services available to them. 14 Other provisions of the ACA, such as prohibiting the exclusion of people with pre-existing conditions from obtaining insurance coverage, are also expected to significantly improve coverage for patients with HIV. Additionally, the continued availability of government funding through programs like the Ryan White HIV/AIDS Program is credited with helping to ensure that care is provided to patients with limited resources and for covering the costs of ancillary services that can improve patients' ability to adhere to HIV treatment regimens. 15 However, despite these programs, barriers to care still exist and need to be addressed. HIV patients have reported that HIV specialty providers may not participate in the health coverage plans that are accessible to them, significantly decreasing their available healthcare options. 16
Multiple study participants expressed concerns about a potential shift in the locus of care for patients with STIs. Private medical providers who have limited experience with STI cases may not have the expertise or the willingness to screen and manage patients in a manner consistent with national public health guidelines established by the US Centers for Disease Control and Prevention (CDC). Evidence indicates that STI screening by physicians is often inconsistent with national recommendations. 17 Study participants also expressed concern about private medical providers' willingness to ask STI patients about their sexual histories and to provide expedited partner therapy, the practice of prescribing treatment for a patient's sexual partner(s) without a physical exam. There is evidence that patients with gonorrhea and chlamydia who are seen by private medical providers may be less likely to be offered expedited partner therapy—recommended in national STI guidelines—than patients who are seen at STI or family planning clinics.18,19 These particular aspects of STI clinical care may be unfamiliar to some private medical providers, but they are vital to controlling the spread of these diseases in the community.
Several study participants expressed the greatest concern about the treatment and management of TB patients in the private sector. Typically, public sector TB control programs are responsible for ensuring the appropriate diagnosis and effective treatment of TB patients and monitoring patients' compliance with their prescribed treatment regimens. As funding for TB control becomes increasingly constrained, however, there have been calls for greater private sector involvement in the treatment and management of TB patients.13,20,21 As a result of TB's decreasing burden, most American private medical providers have limited experience with diagnosing and treating the disease, and several experts we interviewed questioned the quality of care that private medical providers can provide. An analysis of pulmonary TB reported in California during 2007 to 2011 found that patients who received care from private medical providers were less likely to receive care consistent with state and national guidelines than patients treated by health departments. Failures included improper provision of directly observed therapy to ensure patient adherence and lack of documentation of sputum culture conversion to ensure efficacy of treatment. 21
In order for patients with infectious diseases to be appropriately managed by private medical providers in a manner consistent with CDC public health guidelines, a number of barriers need to be addressed. First, education campaigns and specialized training may be needed to improve provider knowledge about CDC screening and treatment guidelines for infectious diseases of public health importance. Second, close collaboration between private medical providers and health departments will be required to ensure that optimal care is provided to these patients. As care shifts to private medical providers, public health departments will likely transition to more of an advisory role, working to ensure that patients are properly screened, diagnosed, and treated in the private sector and that their contacts and partners are identified and appropriately managed.
Several barriers outside the control of individual health departments also need to be addressed. Clinicians have cited lack of time for partner evaluation, risk assessment, and counseling; inadequate facilities or equipment; insufficient staffing; and perceptions about liability and legal authority—particularly with respect to expedited partner therapy—as significant barriers to adopting CDC treatment guidelines. 22 Study participants indicated that private medical providers may also have limited ability to access, store, or administer specific diagnostics or medications for TB (eg, tuberculin, isoniazid) and STIs (eg, bicillin) on site.
Sustained Commitment and Investment Are Needed to Maintain Public Health Surveillance
With the expansion of insurance coverage under the ACA, there may be important shifts in the way surveillance for infectious diseases of public health importance is conducted. On one hand, there is great potential to enhance public health surveillance through the expansion of insurance coverage afforded by the ACA. As more patients gain access to insurance and seek care, the likelihood increases that their condition will be diagnosed, treated, and reported. For example, a recent analysis found that the number of newly identified cases of diabetes in Medicaid patients increased by 23% between 2013 and 2014 in states that expanded Medicaid—compared to an increase of 0.4% in states that did not. 23
Some health departments, however, may experience decreases in the amount of available surveillance information. In addition to receiving notifiable disease reports from private medical providers, public health departments that operate clinics have direct access to demographic and clinical information that can provide insight into illnesses occurring in the community, including risk factors for infection, effectiveness of treatment, and patient adherence to treatment regimens. Such information can be gleaned from clinical records, but it is not typically included in case reports sent to public health departments by laboratories and private medical providers.
Data sharing agreements with private medical providers, Accountable Care Organizations, and third-party payers may be an important step toward improving the availability of vital ancillary surveillance data and providing insight into how infections are diagnosed and treated and what measures may help reduce incidence. However, many health departments do not currently have access to the information technology, personnel, and other resources necessary to capture, manage, and analyze surveillance data obtained from these sources. 24
Public Health Departments Continue to Struggle to Bill Insurers for Clinical Services
Health departments that want to continue offering clinical services have been encouraged to develop the capability to bill insurers for services they provide. 25 Proponents of third-party billing stress that reimbursement for clinical services, such as immunizations and HIV/STI testing, creates a critical revenue stream for health departments in the face of decreasing state and federal funding.26-28 Although a national survey reported that the majority of local health departments receive reimbursement from Medicaid, Medicare, and/or private insurers, study participants indicated that many existing billing arrangements at health departments were established through special agreements and/or carve-out programs (eg, refugee health) and cannot be easily extended to other clinical services. 26
Significant hurdles stand in the way of health departments developing the capacity to bill third-party payers. First, while some health departments have a long history of billing public insurers like Medicaid, many report challenges in dealing with private insurers. 29 Second, while some health departments have made progress in billing insurers for immunization services, study participants noted that it has been more difficult to bill for other clinical services, such as reproductive health or STI screening. Additionally, some health departments have reported challenges in being recognized as a qualified provider under some insurance plans. For example, many health departments rely on nurses with expanded scopes of practice, who are not always recognized by insurance companies as qualified to provide some services. 30 Furthermore, some health departments are having difficulty accepting co-payments from patients as required by some third-party insurers. Grant guidance or other regulatory requirements in some states stipulate that access to care for infectious diseases of public health importance be provided free of charge, making it difficult for health departments to collect insurance information or co-payments.
Health departments are also concerned that persistently high out-of-pocket costs associated with a fee-for-service model may serve as an economic disincentive for individuals to seek care. 31 Though the ACA requires insurance plans to cover the costs of certain vaccinations and other preventive services, there is no national guarantee that private insurance companies will cover, without cost sharing, all of the associated fees for diagnosis and treatment of infectious diseases. As a result, health departments may have to negotiate with payers on a case-by-case basis to cover the cost of diagnostic tests and medications. Study participants also expressed concerns about the diagnostic and therapeutic benefits offered by third-party insurance plans. One state public health participant stated that, when they analyzed the prescription drug coverage offered by plans in their state, they found that the covered drug formularies were not consistent with the standard of care for HIV and TB.
There Are Important Questions About Federally Qualified Health Centers' Readiness to Absorb New Patients
In many areas, federally qualified health centers play an important role in the diagnosis and treatment of communicable diseases. They tend to offer a broad scope of services and be located in close proximity to at-risk communities. Additionally, because they have considerable experience working in these communities, they can often provide culturally competent care to patients from ethnic or sexual minority groups. As a result, these health centers are increasingly being identified as a resource for the provision of safety net clinical services. The Community Health Center Fund established by the ACA is slated to provide $11 billion over a 5-year period for the operation, expansion, and construction of health centers across the country. 32 Additionally, the American Reinvestment and Recovery Act (ARRA) appropriated $2 billion to expand community health centers. 33
There is concern, however, that not all health centers are resourced or staffed to accommodate an influx of patients with infectious diseases of public health importance. While some health centers have hired additional clinical staff in anticipation of increased demand, a national survey of community health center leaders reported the existence of widespread staff shortages and persistent recruitment challenges. 34 Study participants reported that, like private medical providers, some health centers may suffer from a lack of experience with the diagnosis and management of patients with certain infectious diseases of public health importance. While some health centers, such as those run by public health departments, are routinely involved in the diagnosis and management of patients with STIs and TB, others may be unfamiliar with or insufficiently resourced to appropriately screen, diagnose, and treat these diseases and conditions.
Cuts to Clinical Services May Compromise Public Health Surge Capacity
Infectious diseases represent an important and growing threat to the health of US communities. In addition to persistently high rates of infectious diseases, the United States has witnessed a re-emergence of several vaccine-preventable diseases in recent years, including measles and pertussis.35,36 Additionally, outbreaks of emerging diseases such as Zika, Ebola, MERS, chikungunya, and dengue demonstrate the importance of maintaining the capacity to rapidly detect, treat, and control infectious diseases at the local level.37-39 These emergency responses necessitate augmented disease control measures, which require additional staff to implement.
Many project participants stressed that clinical staff employed by health departments are important components of the public health emergency workforce. During outbreaks, public health clinicians may lead or support disease control activities like outbreak investigations and mass vaccination campaigns. These public health professionals work to interrupt disease transmission on a daily basis and have the necessary skills and experience to respond to infectious disease emergencies. Disease investigation specialists—health department employees who conduct contact investigations—are an important resource, providing surge capacity during emergencies. 40 Similarly, in response to the West Africa Ebola epidemic, state and local public health departments nationwide relied on clinical staff from programs like TB control to conduct contact investigations and monitor roughly 10,000 travelers returning from West Africa.41,42 As concern about Zika virus increases, public health departments will again be on high alert; evidence of sexual transmission will likely require the participation of clinical and public health staff with experience managing STIs, including the ability to perform the sensitive work of taking sexual histories, counseling patients on contraceptive use, and engaging in partner notifications. The fact that political debates regarding funding for the US response to Zika centers on the role of reproductive health and family planning clinics is further evidence of the potential overlap of core public health clinical programs and emergency preparedness. 43
Despite this growing threat, funding for public health departments has decreased over the past several years, particularly for preparedness. Federal public health funding has remained flat (unadjusted for inflation) since 2009, and state funding has experienced a significant drop-off. From 2008 to 2014, average state per capita funding for public health decreased from $33.71 to $31.06, “a cut of more than $1.3 billion adjusted for inflation.” Additionally, the federal Public Health Emergency Preparedness grant program administered by the CDC has seen a 30% reduction since 2005.2,44 According to a 2015 survey, 23% of local health departments reported budget cuts in 2014. 6 Decreased funding has forced many public health departments to make significant personnel reductions. In fact, the 2015 survey reports that health departments have eliminated approximately 51,700 jobs since 2008, 6 including more than 5,000 public health nurses, who are often called on to support emergency response operations. 7
Limitations
Although we attempt to evaluate the role of the ACA in changes to the diagnosis, treatment, surveillance, and control of infectious diseases of public health importance following implementation of this new healthcare legislation, our analysis does not demonstrate causality. In truth, many of these changes may have preceded implementation of the ACA. However, we can, with reasonable confidence, conclude that efforts to implement the ACA, and political perceptions of what the legislation does and does not do, play a role in each of the findings contained in this analysis. The ACA may have accelerated the impact of, created conditions that contributed to, or failed to adequately address changes that occurred prior to implementation of the legislation rather than being the impetus for the changes identified in our research.
Public health trends and experiences with ACA implementation can vary considerably by locality. While we attempted to increase the generalizability of our analysis by conducting interviews with a diverse list of participants from multiple states, including those with and without the experience of expanding Medicaid eligibility, we were not able to interview participants in every state. We did not seek to obtain consensus across our study participants. Our findings represent common themes identified in our interviews and literature review, but our conclusions may not be fully applicable for all localities.
Recommendations
1. Ensure full coverage for diagnosis and treatment of infectious diseases of public health importance without cost sharing to patients.
Early diagnosis and treatment can decrease the likelihood that patients will develop serious illness, thereby reducing the chance that they will transmit their infection to others. As a result, it is critical that infected individuals are able to promptly seek medical attention without worrying about the associated costs. Though cost-sharing requirements are intended to reduce unnecessary healthcare expenditures, there is evidence that they may produce the opposite effect. 45 Studies have found that cost-sharing requirements can reduce adherence to therapy for chronic conditions and the use of preventive services, leading to compromised health outcomes.46-49 Patients who are worried about out-of-pocket costs may delay or forgo seeking early medical treatment, potentially increasing the total cost of treating the disease, either due to increased severity of the disease or additional cases resulting from disease transmission.
Coverage of care for infectious diseases of public health importance is not fully addressed by the ACA. Though the ACA requires that insurers cover without cost sharing certain preventive services such as HIV and STI screening, patients who are ultimately diagnosed with an infectious disease of public health importance may be responsible for all or part of the costs associated with follow-up medical testing, treatment, and office visits.
Given that low-income populations remain at high risk for developing infectious diseases of public health importance, it is important that cost barriers be removed to encourage infected individuals to seek care. There are 2 possible ways to ensure full coverage for healthcare costs associated with diagnosis and treatment of these diseases. First, states have the ability to negotiate with insurers to determine which services must be covered. While we know of a few states that are beginning to have conversations with insurers to ensure that costs for diagnosis and treatment of diseases like TB are sufficiently covered, it appears that most states' negotiations with insurers have focused on chronic illness rather than infectious diseases. Another option is to amend required coverage at the national level. The ACA currently requires insurers to provide coverage for items and services in 10 categories:
50
• Ambulatory patient services • Emergency services • Hospitalization • Maternity and newborn care • Mental health and substance use, including behavioral health treatment • Prescription drugs • Rehabilitative and habilitative services and devices • Laboratory services • Preventive and wellness services and chronic disease management • Pediatric services, including oral and vision care
Infectious disease diagnosis and treatment services could be added to this current list of essential health benefits to reduce or eliminate cost-associated barriers to care.
Of these 2 approaches, the national-level approach has one major benefit over the state approach in that nationwide consistency resulting from a common standard eliminates public vulnerabilities resulting from variability between state policies. Inclusion of diagnosis and treatment of infectious diseases of public health importance to essential health benefit benchmark plans should be considered, as outbreaks of infectious diseases that begin in one state can spread across borders, forcing other states to absorb the cost and public health toll.
2. Develop real-world models for public health/private sector integration.
There have been many calls for improved integration between public health and private sector health care, particularly for primary care providers. While all of the study participants representing public health understood the value of enhanced partnerships with private medical providers, most did not have a clear idea of the steps required to develop these partnerships. A number of policy initiatives have encouraged public health and healthcare integration, but few projects have demonstrated how this can be achieved with respect to infectious diseases of public health importance.51-53
Progress toward enhanced integration between public health and health care for the control of infectious diseases of public health importance could be facilitated by the availability of real-world examples. Study participants suggested that efforts to fund pilot projects designed to tackle the practical aspects of forming and maintaining effective partnerships would be beneficial. Efforts to integrate public health and health care would likely have to be tailored to the specific circumstances of each location, but study participants felt that being able to see the specific steps that other health departments took to develop effective partnerships would help in developing their own plans. Additionally, the availability of pilot funding may help public health departments recruit private medical providers to participate, which can be an important first step toward collaboration.
3. State or federal agencies can facilitate health departments' efforts to bill private insurers for clinical services by leading or assisting with insurance company negotiations.
Although health departments across the United States have made significant progress in developing the capacity to bill insurers for the clinical services they provide, a number of important barriers are slowing further progress. One common barrier that health departments are collectively experiencing is the ability to demonstrate to insurers that they are qualified providers. It is clear that the way in which public health clinics operate can be quite different from private sector healthcare facilities, which can be difficult for insurers to understand. Additional work is needed to educate insurers about the type of care that occurs at public health clinics and its value. State and federal agencies (eg, HHS, Centers for Medicare and Medicaid Services [CMS]) should engage with insurers for the purpose of facilitating the process of qualifying providers at public health clinics. In turn, insurance plans can help define minimum requirements for reimbursement of care at public health clinics. This may entail insurers agreeing to set different standards for health departments that provide clinical care, such as recognizing expanded duty nurses as qualified providers for certain services.
Right now, individual health departments are trying to have these conversations with individual insurance plans, but study participants from local health departments reported that the process is inefficient. These negotiations can often yield wide variations in results, depending on the insurance plan (or individual) with which (whom) they are negotiating. Elevating these negotiations to the state and/or federal level may help break through bottlenecks that local health departments are experiencing.
4. Improve surveillance by supporting enhanced use of electronic health records.
As the locus of care for patients with infectious diseases of public health importance continues to shift away from public health clinics, additional work will be required to ensure that important surveillance information is not lost. Health departments will likely continue to receive reports of notifiable diseases for patients; however, as discussed previously, some data that are typically captured during clinical interactions at public health clinics—often critical to surveillance efforts—may be lost when patients seek care from private medical providers. Electronic health records offer considerable potential as a mechanism to supplement surveillance for infectious diseases, and there have been important efforts in recent years to increase public health use of electronic health records. Through the development of requirements for the federal electronic health record program, commonly known as “meaningful use” requirements, the HHS Office of the National Coordinator for Health Information Technology (ONC) has mandated that specific categories of data be captured in electronic health records and submitted to public health departments. 54 To date, meaningful use criteria have increased public health departments' access to electronic health record data categories like electronic laboratory reporting and immunization status.
Despite moderate progress in this area, the greatest potential for electronic health records to supplement surveillance remains untapped. Electronic health records can contain rich data about patients' longitudinal medical history, risk factors for infection, and other clinical and demographic information that can help public health agencies assess whether changes in incidence of infectious diseases of public health importance are occurring in their respective communities. Additionally, electronic health records can potentially provide better and earlier indication of outbreaks than may be possible by waiting for notifiable disease reports, which are typically submitted by laboratories at a later time. Finally, most commercial electronic health record systems were not designed with public health applications in mind. These systems do not include critical data fields for some risk factors (eg, indicator of foreign birth) or prompt private medical providers to test for or report infectious diseases of public health importance.
Together with its partners, ONC has begun to explore these ancillary uses of electronic health records for public health efforts. Initiatives like ONC's Electronic Case Reporting, which aims to improve the speed with which public health departments receive notifications of potential health threats, and pilot projects like New York City's Primary Care Information Projects, are steps in the right direction toward improving the ability of public health agencies to tap electronic health records for monitoring population health. 55 Financial support to local health departments for efforts like these should be greatly expanded. 3
5. HHS should support the development of quality metrics consistent with national public health screening and treatment guidelines.
One of the anticipated public health benefits of the ACA is the law's interest in promoting healthcare quality. The ACA encourages improvements in healthcare quality through several means, such as the development of healthcare quality measures for Medicaid enrollees 56 and the establishment of Accountable Care Organizations—voluntary networks of medical providers working together to improve coordination and quality of care for Medicare patients.57,58 Through efforts like the ACA's Hospital Readmissions Reduction Program, the ACA requires CMS to reduce payments to hospitals with excess readmissions of patients. 59
As efforts to develop, refine, and implement these quality assurance mechanisms continue to progress, the HHS should examine ways to develop quality metrics aimed at optimizing screening, diagnostic testing, and treatment of patients with infectious diseases of public health importance. Considering evidence that care for patients with these infectious diseases by private medical providers is often inconsistent with national guidance, 21 the development of these metrics may help improve quality of care. Most efforts at developing quality metrics to date, however, have focused on reducing costs associated with chronic illness, and additional attention is required for infectious diseases.
6. Public health departments should explore ways to increase private medical providers' ability to manage patients with infectious diseases of public health importance.
With increased participation by private medical providers in the screening, diagnosis, and treatment of infectious diseases of public health importance, health departments may have to assume an advisory role to ensure that care is provided in a manner that is consistent with national guidelines. For complex conditions with which private medical providers have little experience, health departments and other specialists may need to provide technical guidance regarding treatment and patient management. This model is increasingly being used in some states for the clinical management of TB. Nationally, there exist 5 Regional Training and Medical Consultation Centers that consult with health departments and clinicians on treatment regimens and other aspects of TB care. In the same vein, the National Network of STD Clinical Prevention Training Centers provides services to enhance healthcare providers' awareness of sexual health issues. Similar models where specialists or health departments serve as consulting partners should be explored for other infectious diseases.
Telemedicine initiatives could also be used to increase private medical providers' ability to manage unfamiliar conditions. The University of New Mexico's Project Extension for Community Healthcare Outcomes (Project ECHO) uses telemedicine and a hub-and-spoke model to train clinicians to manage unfamiliar conditions. This model demonstrated improved care for hepatitis C patients in underserved communities. 60 A similar approach may also benefit management of patients with infectious diseases of public health importance, as this approach also has the benefit of extending the availability of care in regions, such as rural or frontier areas, where there is a limited provider network.
Conclusion
While the ACA has the potential to improve the public's health by increasing health insurance coverage, its implementation has not fully addressed specific needs associated with diagnosis, surveillance, and control of infectious diseases of public health importance. Additional work is needed to ensure the continued availability of safety net care, which will likely require the continued operation of public health clinics. As private medical providers become increasingly involved in the diagnosis and care of infectious diseases of public health importance, health departments should seek to partner with these providers to ensure that treatment of patients and their contacts and partners occurs in a manner that is consistent with national public health guidelines. Finally, as patient load is expected to shift away from public health clinics, considerable care must be taken to ensure that traditional public health capabilities are maintained, including infectious disease surveillance and control. The ACA has the potential to have a long-term positive impact on America's health, but the relationship between public health and health care must be strengthened in order to promote continued improvement in both areas.
Footnotes
Acknowledgments
The authors wish to acknowledge the Robert Wood Johnson Foundation, which provided financial support for this analysis.
Appendix A: Study Participants
Chris Aldridge, National Association of County and City Health Officials
John Auerbach, CDC Associate Director for Policy
* Heidi M. Bauer, California Department of Public Health
* Robert Belknap, Denver Health and Hospital Authority
Linda Bell, South Carolina Department of Health and Environmental Control
Georges C. Benjamin, American Public Health Association
Stuart M. Berman, CDC National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention
John Bernardo, Massachusetts Department of Public Health
John Billington, Infectious Diseases Society of America
Tricia Brooks, Georgetown University Health Policy Institute
* Sean Cahill, The Fenway Institute
Bob Carr, Massachusetts Department of Public Health
Jennifer Cochran, Massachusetts Department of Public Health
Sabrina Corlette, Georgetown University Health Policy Institute
James Daniel, HHS Office of the National Coordinator for Health Information Technology
Megan Davies, North Carolina Department of Health and Human Services
Maurice Denis, National Association of Community Health Centers
Thomas E. Dobbs III, Mississippi State Department of Health
Jeffrey Duchin, Public Health–Seattle and King County
Jeffrey Engel, Council of State and Territorial Health Officials
* Jennifer Flood, California Department of Public Health
Laurie Forlano, Virginia Department of Health
Evelyn Foust, North Carolina Department of Health and Human Services
Andrea R. Fox, Squirrel Hill Health Center
Jared B. Fox, CDC Office of Health System Collaboration
Petty Gast, Arizona Partnership for Immunization
David Gruber, Texas Department of State Health Services
Christine Hahn, Idaho Department of Health and Welfare
Katrina Hedberg, Oregon Health Authority
Julie Higashi, Curry International Tuberculosis Center
Esther Hing, CDC National Center for Health Statistics
* Christine Ho, CDC Division of Tuberculosis Elimination
Beth Hurley, Cicatelli Associates, Inc.
Debbie Isenberg, Cicatelli Associates, Inc.
Joseph Iser, Southern Nevada Health District
Timothy F. Jones, Tennessee Department of Health
Elizabeth Jones, Cicatelli Associates, Inc.
Diana L. Jordan, Virginia Department of Health
Jessica Kahn, Centers for Medicare and Medicaid Services
* Jennifer Kates, The Henry J. Kaiser Family Foundation
Patsy Kelso, Vermont Department of Health
Anne D. Kershenbaum, Tennessee Department of Health
* Duane Kilgus, CDC Immunization Services Division
Amy Killelea, National Alliance of State and Territorial AIDS Directors
Glenn Landers, Georgia State University, Georgia Health Policy Center
* Dara Alpert Lieberman, Trust for America's Health
Mary-Beth Malcarney, George Washington University Milken Institute School of Public Health
* Jennifer MacFarquhar, CDC Epidemiologist assigned to North Carolina Department of Health and Human Services
Mary G. McIntyre, Alabama Department of Public Health
Kathy McNamara, National Association of Community Health Centers
* Beth Meyerson, Indiana University School of Public Health
Karen J. Minyard, Georgia State University, Georgia Health Policy Center
Judith A. Monroe, CDC Office for State, Tribal, Local and Territorial Support
Jane L. Moore, Virginia Department of Health
* Nuala S. Moore, American Thoracic Society
Melissa Moorehead, Michigan Public Health Institute
Sarah J. Newman, National Association of County and City Health Officials
Leah Northrop, California Department of Public Health
* Stephanie S. Arnold Pang, National Coalition of STD Directors
Liisa Randall, Massachusetts Department of Public Health
Trish Riley, National Academy for State Health Policy
Jill Rosenthal, National Academy for State Health Policy
Michael Sage, Stop TB USA
* Erika Samoff, North Carolina Department of Health and Human Services
Laura Herrera Scott, Maryland Department of Health and Mental Hygiene
Maunank R. Shah, Johns Hopkins University; Baltimore City Health Department
* Umair A. Shah, Harris County (TX) Public Health and Environmental Services
William Smith, National Coalition of STD Directors
Angela Snyder, Georgia State University, Georgia Health Policy Center
Lynn Sosa, Connecticut Department of Public Health
Arjun Srinivasan, CDC Division of Healthcare Quality Promotion
Elizabeth J. Stoller, California Department of Public Health
Bruce Baird Struminger, University of New Mexico School of Medicine, Project ECHO
* Kathy Talkington, Association of State and Territorial Health Officials
Christina G. Tan, State of New Jersey Department of Health
Litjen “L.J.” Tan, Immunization Action Coalition
* Jennifer Tinney, Arizona Partnership for Immunization
Kathy Turner, Idaho Department of Health and Welfare
Andrea Weddle, HIV Medicine Association
James N. Weinstein, Dartmouth-Hitchcock
Diane C. Woolard, Virginia Department of Health
Jan Young, California Department of Public Health