
Abstract
Emerging infectious diseases pose a serious threat to public health security; this is especially true in the underdeveloped world because of limited resources to combat them. These emerging pathogens are characterized by a novel mode of pathogenesis and, in some cases, a broad host range. Over the past few decades, Pakistan has suffered a great deal from infectious diseases such as dengue, Crimean-Congo fever, hepatitis, measles, and polio. Changing climate conditions, environmental degradation, global warming, loss of biodiversity, and other ecological determinants have a direct effect on these diseases and result in the emergence and reemergence of infectious entities. The causes of such disease outbreaks are complex and often not well understood. Dealing with an outbreak requires an integrated and coordinated approach, with decision making by various state departments. Stringent biosecurity and biosafety protocols can help to reduce the chances of infection dissemination. In order to mitigate the risks associated with emerging pathogens, there is a greater need to understand the interactions of pathogen-host-environment, to monitor molecular evolution and genomic surveillance, and to facilitate the gearing up of scientists across the globe to control these emerging diseases. This article reviews recent outbreaks in Pakistan and challenges for the development of an agile healthcare setup in the country.
Emerging infectious diseases pose a serious threat to public health security; this is especially true in the underdeveloped world because of limited resources to combat them. This article reviews recent outbreaks in Pakistan and challenges for the development of an agile healthcare setup in the country.
N
Infectious diseases are among the leading cause of disability and mortality in Pakistan. Epidemics of new and old infectious agents appear from time to time, having a negative impact on people and magnifying the burden on the economy. 2 Often such incidents are followed by a global response that entails the diversion of developmental funds. After having been in a state of denial for a few decades, the world community has recognized the potential threats of emerging and reemerging infectious diseases, which is evident by the resolve in the Sustainable Development Goals (SDG) to combat infectious diseases like malaria and AIDS and to support the global movement to wipe out such diseases from the face of the earth. Now there are serious efforts, in the form of the Global Health Security Agenda (GHSA), the Global Health Initiative (GHI), and the Cooperative Threat Reduction (CTR), all of which aim to build robust, collective, sustainable, and globally integrated health management systems that are safe and secure. 3
Previous studies indicate that the concentration of pathogenic infectious diseases called the latitudinal species diversity gradient in human pathogens is increasing toward the equator, which is mostly attributable to factors like socioeconomic drivers (eg, population density, overuse of antibiotics, improper agricultural practices) and ecological and environmental disturbances (eg, deforestation, biodiversity loss, pollution, wildlife extinction) in these regions. 4 These emerging pathogens are characterized by broad host ranges and new methods of pathogenesis. This review specifically focuses on the current status and capacity of Pakistan to deal with emerging infectious diseases and outbreaks.
Geography and Demography
Pakistan is a large country (about 800,000 km2) with a population of approximately 184,350,000 people, making it the fifth most populous country in the world according to the World Health Organization (WHO). It is composed of 5 provinces, the Federally Administered Tribal Areas (FATA), and Kashmir. Even though the country has a fairly well-developed organizational infrastructure, the health indicators are poor and show high mortality rates for both communicable and noncommunicable diseases (Figure 1).
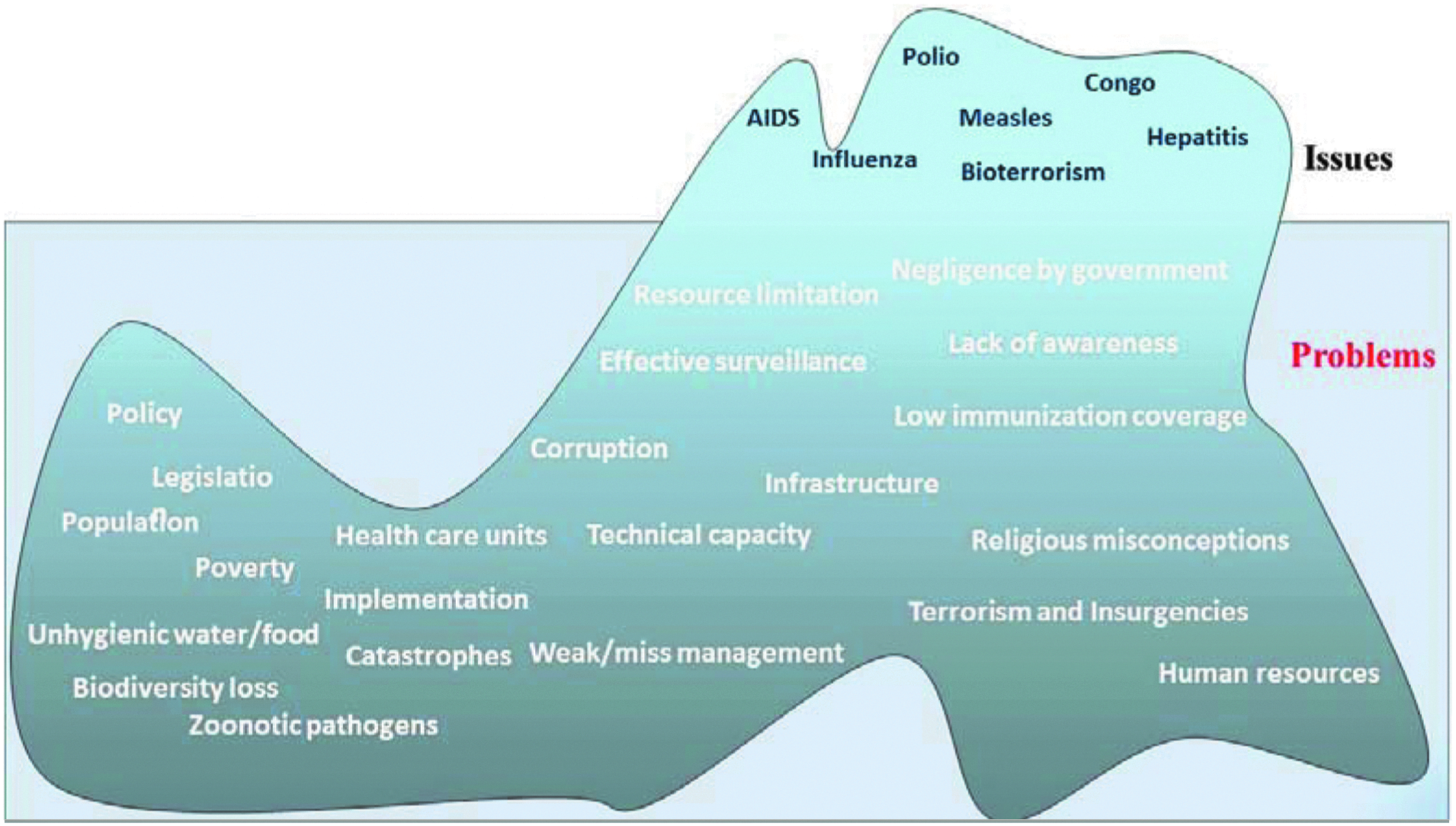
Iceberg Model of the Healthcare Issues in Pakistan
Pakistan in the 21st Century
The occurrence of emerging and reemerging infectious diseases (Figure 2) can be a grim situation for third world nations such as Pakistan. This region has been hit by several epidemics, which we discuss below. According to the WHO, the country is at risk for many outbreaks in the future because of inadequate primary health care, improper sanitation, overcrowded cities, an insufficient number of medical practitioners and insufficient medications, contaminated water, lack of awareness among the public about hygienic conditions, 5 meager attention by the government, a large number of refugees and internally displaced people, religious misconceptions, and resource limitations. Over the years, Pakistan has also suffered from deadly calamities like earthquakes and floods. Beyond these issues, the country is in a state of war against internal and external insurgents over the past decade, causing a major obstacle to primary health care as a result of the diversion of funds to national security and reaching out to needy people in the affected areas.
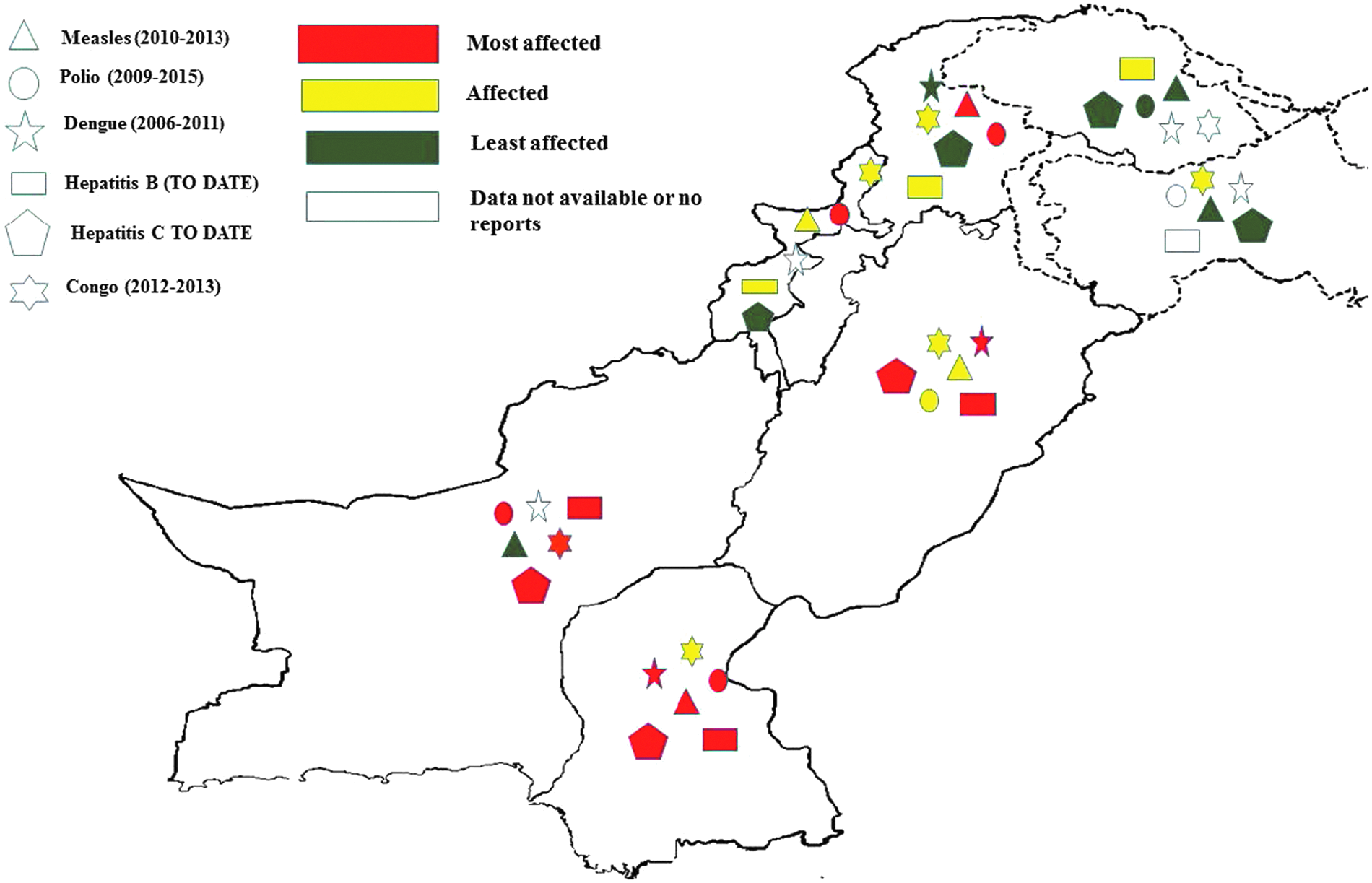
Intensity of Different Outbreaks that Occurred in Pakistan
Pakistan as a developing country faces many challenges because of limited resources and financial constraints. According to recent data, Pakistan spends 4.7% of its total budget on health care, which is not enough for a populous country like Pakistan (Figure 3a and 3b). There are estimated to be 2 primary healthcare units per 10,000 people in the country. The maternal mortality ratio is 170 out of 100,000 people. 6
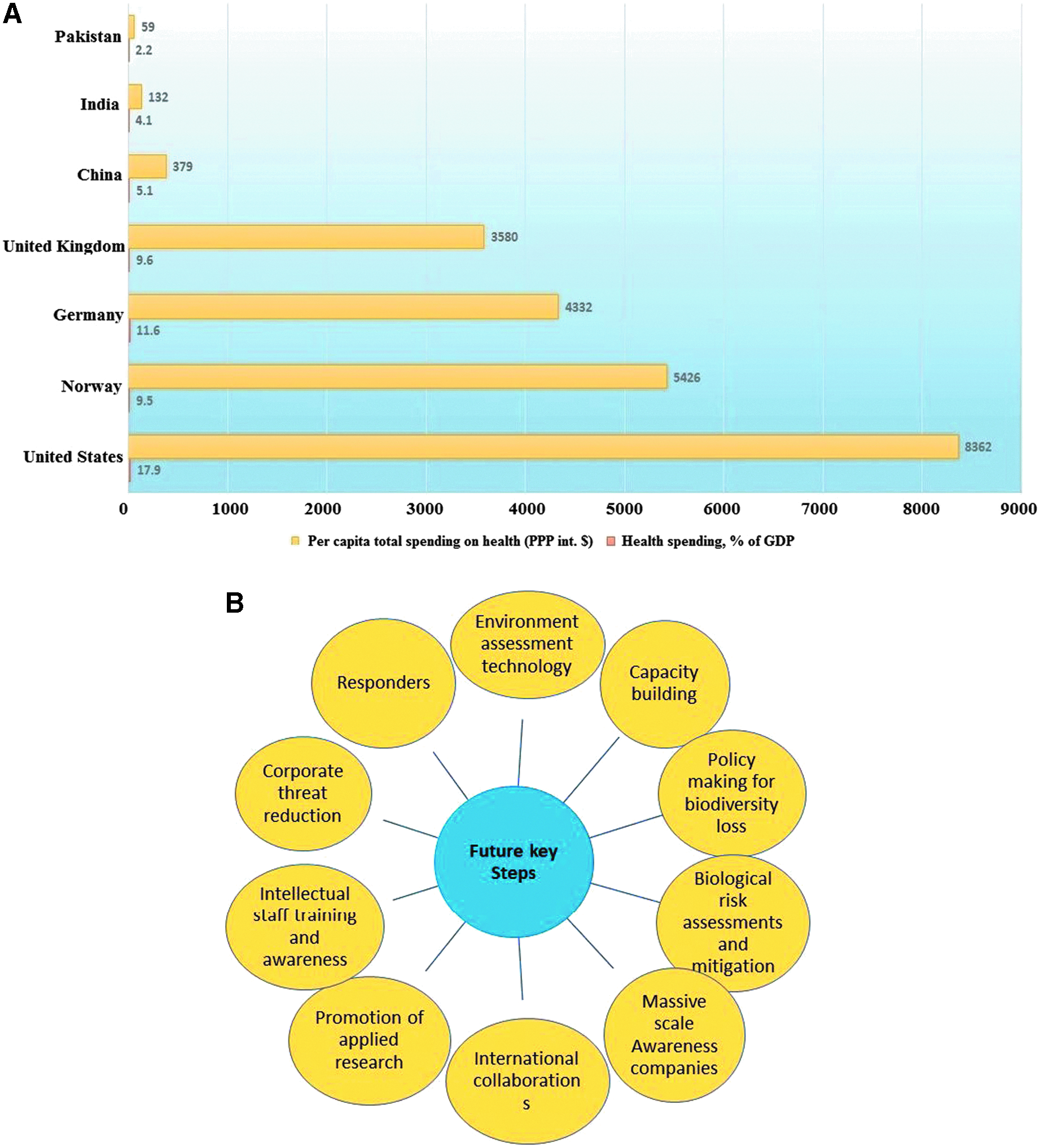
Current Situation in Pakistan and Recommendations for the Future. (A) comparison of healthcare expenditure in Pakistan and some other countries. (B) recommendations to improve health care in Pakistan
Even after massive technical advancements, our knowledge about infectious diseases is not sufficient. This is a greater concern for underdeveloped countries because they lack the technological capacity to deal with such issues effectively. There is a great need for global partnerships to provide a collaborative and multidisciplinary approach to deal with these issues. (These health issues are discussed in the next section in detail.) Because of the flaws in healthcare practices and the environmental conditions, epidemics always find a way to spread in the local population.
Emerging and Reemerging Infectious Diseases
Dengue Virus
Dengue virus, which is now characterized as an emerging infection, affects from 50 million to 100 million people globally, with an estimated 24,000 deaths per year. Dengue virus first appeared during World War II and was reported to have expanded in Asia after the 1980s. 5 It is classified into 4 serotypes: DEN-1, DEN-2, DEN-3, and DEN-4. Viral transmission is brought about by the vector Aedes aegypti mosquito. Although a tetravalent dengue vaccine has recently been registered, the diagnosis time will still remain critical for patient management. 7 Dengue fever may be characterized as classical dengue fever, dengue hemorrhagic fever (DHF), or dengue shock syndrome (DSS). 8
Pakistan has had a history of recurrent dengue fever outbreaks since the 1980s. However, it was first documented in 1994 and considered endemic to Pakistan and other neighboring countries. Outbreaks are reported frequently in the monsoon season—that is, the season of heavy rainfalls, which provide an environment conducive to the virus to propagate, causing hemorrhagic fever. 9 Dengue outbreaks are reported across Pakistan, but Punjab and Sindh have been reported as the provinces most affected.
From 2003 to 2014, there have been recurrent outbreaks of dengue across the country. In September 2015, there were 20 reported cases of dengue at Rawalpindi (Punjab), a city near the federal capital of Islamabad. Dengue is also reported in the northern part of the country; the contributing reason for this expansion is competent mosquito vectors. According to the WHO weekly epidemiology report, in September 2013, of 4,388 suspected cases countrywide, 3,177 were reported in Khyber Pukhtunkhwa (KP), and 1,098 cases were reported from Sindh province. In November 2015, the total suspected cases of dengue hemorrhagic fever reached 8,894 in KP, while District Swat was the worst-affected area during this period. Dengue virus was also reported in Baluchistan in September 2013. 10 According to WHO, the first vaccine (developed by Sanofi Pasteur) against dengue virus infection was registered in December 2015, and 5 additional vaccine candidates are currently at different stages of evaluation. The efficacy, effective vaccination in the target population, cost-effectiveness, and safety of these vaccines will play a key role in preventing dengue virus infection in Pakistan.
Measles Virus
Measles is a contagious but vaccine-preventable viral disease that mostly affects the respiratory tract (febrile respiratory prodrome); the most general symptoms include maculopapular rashes, cough, and fever, which may lead to death. After global initiatives in the previous decade (2000-2011) to combat measles, the disease prevalence dropped significantly (up to 71%), and mortality rates dropped to just 1 per 1,000. 11 About 95% of measles deaths occur in low-income countries. 12
Measles eradication programs like the Global Measles and Rubella Strategic Plan (2012-2020) represent a success story, but specific circumstances in Pakistan make measles eradication challenging. Pakistan is committed to wiping out measles from the country; for this purpose, it has adopted a resolution of the East Mediterranean Region (EMR) of WHO since 1997. However, the goal is far from completion. The plan was supposed to be executed by achieving measles vaccination coverage of more than 95% among 1-year-old children, using mass immunization campaigns and follow-up vaccinations, increasing awareness levels, and strengthening the capacity and technology for surveillance of the deadly virus. Unfortunately, due to some issues discussed below, the goals were not achieved. 13
In recent outbreaks of measles, there were 4,000 and 14,000 (∼1,000 cases/million population) confirmed cases in 2011 and 2012, respectively, resulting in the deaths of 238 people. 14 In 2013, a total of 321 people were reported to have lost their lives to measles in Pakistan. 11 The country has a case-based survilliance system in target areas, 15 but the situation calls for improved strategies for effective vaccination in the country, especially focusing on large cities (eg, Karachi, Lahore, Peshawar, Quetta), remote areas (eg, Lasbella, Dir upper, Karak, rural Sindh), and areas affected by the war on terror (FATA).
Crimean-Congo virus
Crimean-Congo hemorrhagic fever (CCHF) is another deadly pathogen that is prevalent in certain parts of Africa, Europe, Asia, and the Middle East; it has a mortality rate of 3% to 30%. 16 Crimean hemorrhagic fever (CHF) first became evident in 1944 in the former Soviet Union. 17 The disease mostly affects farmers and people living in close proximity to livestock. In a recent outbreak in Turkey, 90% of the infected individuals were farmers. 18
Congo virus is associated with ixodid ticks (genus Hyalomma), its natural vector. 18 It was first reported in Pakistan in 1976. Sporadic cases and mini-outbreaks of CCHF have been reported in certain parts of Pakistan, including Rawalpindi, Abbottabad, Kashmir, Peshawar, Karachi, and some parts of Baluchistan. To date, there have been 14 scattered mini-outbreaks, 9 of which occurred in Baluchistan.17,19 About 40 to 60 cases have been reported annually since 2000. Data from the Disease Early Warning System (DEWS) report 49 confirmed cases of Congo hemorrhagic fever in 2012; 60 infected individuals were reported in 2013. Increased awareness, rapid diagnosis, proper training of healthcare workers, and community-based infection control measures can be effective tools to prevent Congo virus outbreaks.
Polio Virus
Although polio virus has been eradicated from the rest of the world, the disease continues to be reported in Pakistan, Nigeria, and Afghanistan. The virus is mainly transmitted by oral-fecal and sometimes by oral-oral route. It invades the nervous system and can lead to paralysis in the infected individual within a few days. Polio virus can be found in sewage water from the affected area and can be transmitted through infected respiratory secretions and sneezing. 20
Pakistan is still struggling to eradicate polio infections due in part to political instability and to some social and religious misconceptions. Until 2005, the incidences of polio infection were declining, and the vaccination campaigns were quite effective. However, in 2009, 89 poliomyelitis cases were reported in Pakistan. The number increased to 144 and 198 in 2010 and 2011, respectively.20,21 The highest number of poliomyelitis cases was 306 in 2014 in 44 districts of the country (reported by the National Emergency Action Plan for polio eradication). Extensive vaccination and environmental sampling, accompanied by massive awareness campaigns in these target areas, resulted in a decreased number of cases (a total of 22) in 2015. It is hoped that these polio eradication programs will soon eradicate the disease from the country.
HIV-AIDS
Human immunodeficiency virus (HIV, a lentivirus from the Retroviridae family of viruses) is the causative agent for acquired immune deficiency syndrome (AIDS), which attacks the immune cells of the infected patient, resulting in a decline in CD4 T cells. 22 It is estimated that <0.1% of the Pakistani population has been reported to be infected with HIV;23,24 however, the incidence is high among sex workers, especially when they interact sexually with injection drug users. 25 Ghani and colleagues screened 626,413 blood donors from 1998 to 2013 from northern Pakistan for anti-HIV antibodies; they reported that 0.01% of the individuals were reactive for HIV antigens. 26 This is also true of blood donors from Karachi, a major city in the south of the country. 27 Overall, these data indicate that HIV infection in the general population has remained constant (∼0.01%) over the past 2 decades. Awareness programs and stringent surveillance targeting high-risk groups will be helpful in controlling infection in the future.
Hepatitis C Virus
According to WHO, about 130 to 150 million people are affected by hepatitis C virus infection. A significant number of those people develop chronic liver disease, and an estimated 500,000 die each year globally. Hepatitis C virus (HCV) has wide genetic diversity and variations from region to region based on prevalence of its different genotypes. Globally, genotypes 1 and 3 are most common.28,29
Hepatitis viral infections are highly endemic in Pakistan, with hepatitis B and C being a major disease burden with maximum mortality. Prevalence of HCV is around 5%, with an estimated 10 million infected individuals in Pakistan. 30 Six genotypes have been identified, with genotype 3 (74%) as the most prevalent.31,32 Phylogenetic analysis based on the full-length HCV genome revealed that the HCV-3a prevalent in Pakistan is genetically distinct from those prevalent in the rest of the world. 33 A study by Ali et al reported emerging HCV variants with drug-resistant mutations in Pakistani patients undergoing interferon and ribavirin therapy. 34 The combination treatment of interferon alfa (IFN-α) and ribavirin (RBV) continues to be used widely in routine practice in HCV-infected patients in Pakistan, 35 because recently developed antivirals (eg, ledipasvir and sofosbuvir) and PEG-interferon therapy are quite expensive35,36 and in limited supply. The cost for sofosbuvir-based HCV therapy has been estimated to be US$85,000 to US$110,000 37 in the United States; however, the therapy is available at subsidized rates in Pakistan. HCV prevalence in some underdeveloped pre-urban and rural areas is quite high (up to 25%). 38 The situation has been further worsened by the poverty level, with 30% to 40% of people living on less than US$1 a day. 39 It would be interesting to investigate the effect of recently developed antiviral therapies in HCV-infected Pakistani individuals. Moreover, proper management of resistant HCV variants (both nonresponders and relapsers) is needed.
Avian Influenza Virus
Avian influenza virus represents a major threat to the country's economy, as it can cause infection in humans, birds including poultry, horses, and pigs. The poultry industry constitutes a major portion of the country's economy. 40 Since 1995, there have been 5 epidemics of avian influenza reported in Pakistan, including subtypes H7, H9, and H5. An epidemic of H7N3, a highly pathogenic avian influenza (HPAI), emerged in scattered areas across the country and lasted for about 4 months. 41 In 1998, an outbreak of H5N2, a low pathogenicity avian influenza (LPAI), appeared in broiler chickens and poultry. Similar outbreak of H7N3 emerged in 2000. In 2003-04, the epidemic of H7N3 resulted in severe economic devastation. During the same epidemic, H9N2 was also found in some of the flocks, resulting in a mortality of 70% to 80% in the affected flocks.42,43 Avian influenza viruses isolated from poultry in Pakistan (in 1998-99) were found to be closely related to H9N2 viruses that caused human infections in Hong Kong. 44 Constant surveillance and vaccination programs are recommended for preventing future bird flu influenza infections in the country.
Swine Flu Virus
Influenza viruses have been emerging and reemerging over the past 3 decades, with novel strains of pandemic potential circulating globally. 45 The first outbreak of H1N1 (swine flu) occurred in 2009 in Mexico and spread to several other countries. In Pakistan, the first case of swine flu was confirmed on June 18, 2009. There were a total of 1,242 suspected cases, with 262 laboratory-confirmed cases and 29 deaths reported. But the 2009 swine flu pandemic appeared to be of lesser concern in Pakistan compared to other affected countries. 46 However, an epidemic of swine flu in India (December 2014 to early 2015) was followed by another one in central Pakistan, resulting in an estimated 16 deaths by January 2016. Continued surveillance and mass awareness are important to overcome the disease. 45
Next Steps
Ebola virus has emerged as a global threat, 47 and coronavirus has caused outbreaks in the Middle East, 48 so it is imperative that preemptive practical steps be taken to protect people. In 2014, the first suspected case of Ebola was reported from Karachi, and, because there was no facility there for identifying the virus, the samples were sent to Cairo. 49 There were no negative consequences in this case, but the threat remains. There have been no confirmed cases of coronavirus in Pakistan, but because the Middle East is a favorite spot for travelers and a place where many earn their livelihood, increased and vigilant surveillance should be adopted at airports to screen travelers. In addition, Muslims from all over the world (more than 10 million), gather in Saudi Arabia, to perform the Hajj/Umrah pilgrimage, an important religious festival. 48 The chances of an infection spreading cannot be ignored, 48 and therefore a dedicated health and disease surveillance system for pilgrims is needed.
Recently, in November-December 2016, more than 30,000 people in Karachi were reported to have viral fever and joint pain. The disease symptoms were suspected to be a mild Chikungunya virus epidemic, but the virus has not yet been confirmed. We suggest that facilities need to be developed and strengthened in all major cities for rapid diagnosis of infections in case of sudden epidemics.
Biotechnology Progress Raises Biosecurity Alarms
It is well-established and internationally recognized that life sciences research in Pakistan is considered to be a success story. One reason for this is the increased attention by the government to the biotechnology sector by declaring it a priority area. Significant human resources are generated in life sciences through universities and research institutes. If research activities continue on the same pace, Pakistan will be ranked 27th in biology research by 2018. 40
On the other hand, this progress in biotechnology raises serious questions about biosafety, biosecurity, and dual-use research of concern. 50 A recent survey conducted in Pakistan about the level of awareness among professional scientists raises alarms because it indicated that their awareness levels about biosafety and biosecurity issues are low. 51 There are already experiments being carried out around the world exploring the creation of vaccine-resistant smallpox virus and resurrection of Spanish flu virus and polio virus from scratch.52,53 Considering advances in biological research and viral disease outbreaks, a proactive strategy is required to ensure safety and security.
One category of emerging infections is referred to as “deliberately emerging infections,” which represent not only natural infectious entities but also man-made, genetically engineered infectious entities, which could be engineered for nefarious activities. Bioengineering of potential infectious agents can increase their pathogenicity by introduction of virulence traits or by making their transmission easy, resulting in enhanced infectivity. 54 Since engineered infectious entities can be used for hostile applications, the threat of infectious diseases cannot be ignored, as they can be used to jeopardize the state economy, safety, and the health of the people. 50
The fast spread of infectious diseases is an important transnational global challenge. Since the anthrax attacks in the United States in 2001, the threat of infection-causing agents has become a serious security concern that directly affects the basic and most important element of state security: the individual. Emerging and re-emerging viral pathogens also pose a strategic and economic threat. The magnitude of threat of viral outbreaks is growing because of the increased resistance of continuously evolving pathogens to available therapeutics. 55 Thus, a biosecurity strategy is needed—that is, development of comprehensive measures to prevent and control the biological agents of potential threats. It can be regarded as the life sciences battle line of the national security strategy that encompasses military, economic, and social security. 56
As infectious viral agents continue to evolve and affect the globe, Pakistan needs to pay heed and to assess and manage its capacity to respond to this menace. It becomes even more important given the fact that several infectious disease outbreaks have occurred in the country and that terrorism threatens the country's security internally as well as externally.
Let's take, for example, the re-emergence of the polio virus that persists in Pakistan (along with Nigeria and Afghanistan). Poor public health infrastructure (see Figure 1) and other social and political challenges, such as impediment to vaccination campaigns by terrorist groups in North Waziristan, indicate that the impacts of bioterrorism will be more likely in states like Pakistan where health security is compromised. 57 Thus, a strong public health infrastructure to deal with an outbreak, whether natural or intentional, should be the foremost priority of the country. Prevalence of hemorrhagic fever causing viruses such as dengue and Crimean-Congo fever, zoonotic pathogens such as severe acute respiratory syndrome (SARS), and influenza virus (swine-origin H1N1) and other infectious pathogens in Pakistan indicate a potential future biothreat. Although preventive measures have been successfully employed at the government level, such as vector control strategies to deal with dengue virus, more needs to be done in terms of vaccine development and stockpiling and federal investment in infectious disease research. The possibility of a natural as well as intentional outbreaks exist.
We need to learn a lesson from natural outbreaks in dealing with deliberate ones, as they will require the same strategy. Infectious disease intelligence, surveillance, and epidemiologic strategies as well as laboratory techniques to detect and contain an epidemic are the best means of mitigating the chances of disease spread. 58 Response also requires up-to-date laboratories with the ability to sequence the infectious agents, with the support of government, medical response units, and a prepared work force. 59
Future Prospects
From the discussion, we can conclude that Pakistan faces numerous challenges in health care, which can be broken down into social issues; technical constraints; effective legislation, policymaking, and implementation; awareness and negligence; terrorism; infrastructure; lack of trained human resources; and religious misinterpretations, among other factors (see Figures 1 and 2).
The instability of health in Pakistan originates from several challenges, including poor health indicators, lack of investment, and rising levels of expenditures. This vulnerability is further aggravated by illiteracy, gender inequality, and rapid urbanization. Difficulties in gaining access to essential pre- and postnatal medical services all over the country, in addition to health disparities among provinces and sudden viral outbreaks, further fuel the miseries. Pakistan is vulnerable to multiple disasters like floods, earthquakes, storms, epidemics, and tsunamis. Communicable diseases spread like fire due to unhygienic water and poor sanitation facilities. A versatile healthcare system is crucial for provision of a rapid response to any infectious disease outbreak.
Recent data about the health indicators of provinces show an appalling situation. In 2007, the infant mortality rate in Khyber Pakhtunkhwa (KP) was 63 per 1,000 births. In the past decade, infant mortality has increased from 69 to 79 deaths per 1,000; this is a serious concern for the provincial leadership. A total of 13,702 “lady health workers” were actively working in Khyber Pakhtunkhwa (KP) in 2011, which, according to an estimate, covers about 58% of the total population. Only 64% of the population in Sindh has access to clean water, and a mere 24% of individuals have proper sanitation facilities. The recently recorded mortality rates for infants, neonates, and mothers were 81, 53, and 3 per 1,000 live births, respectively, which is very distressing. Activating healthcare facilities has remained a dilemma for nearly 96 million people of Punjab. Both communicable and noncommunicable diseases pose multiple stresses on the current health system. Even though the Punjab government has made a huge investment in recent years, health indicators are yet not significantly improved. In Baluchistan, poverty and low literacy has adversely affected health status. 60 The literacy rate in Baluchistan among females is the lowest of any place in the world. Due to persistent low-intensity transmission of wild polio virus across the Pakistan-Afghanistan border, polio is endemic in most parts of Baluchistan.
Social issues
Religious Misconceptions
About 97% of the population in Pakistan is Muslim, and the impact of religion is persistent in many aspects of life. Polio cases are continuously emerging from different regions in Pakistan. About 72 new cases were reported in 2015, ahead of Nigeria (50 cases) and Afghanistan (9 cases). 61 The misconception in Pakistan that vaccines have certain infertility or harm agents is promulgated by some religious preachers, 62 thus paving the way for viral infections. Family planning in Pakistan is a highly debated topic because of its religious implications. 63 Pakistan is among the 115 countries globally that accept that public health care is a right, yet there is huge discrimination between genders, and especially women who live in rural areas fall victim to religious extremism. One study reveals that in Pakistan girls are at a higher risk of death (68%) compared to boys (57%), indicating a clear bias in the accessibility of social determinants of health. 64
Sanitation and Poverty
Poor people living in rural areas or slums of Pakistan are highly prone to waterborne bacterial and viral diseases (eg, measles, diarrhea, polio). 65 Besides unhygienic water and food sources, poverty represents a major hindrance to health care. According to a government survey, 4 million babies are born annually in Pakistan, and most are born into poor families. 66 Many families lack information on disease prevention and effective hygiene. Poor health, poverty, and poor education often accompany each other. The literacy rate in Baluchistan among females is the lowest in the country; lack of literacy hinders economic development and the means to escape poverty for millions of families. And because of poverty, people do not have economic access to hospitals and medications. Improving sanitation and upgrading the social standards of the people can play a great role in alleviating the incidence of infectious diseases and significantly improve the quality of life for all people.
Internally Displaced People and Refugees
Large numbers of refugees from Afghanistan, an underdeveloped region that is at war, and internally displaced people due to the ongoing war against terrorism represent another major obstacle to the health care of the people. 67 Massive gatherings provide a suitable environment for an outbreak to occur. Pakistan is among the few countries that have a high burden of internally displaced people and refugees from neighboring countries. Internally displaced people are prone not only to common infections but also to serious infectious diseases like scabies, hepatitis, malaria, typhoid, and parasitic infections.68,69 Lack of clean water, a congested environment that facilitates the transmission of communicable diseases, and environmental contamination that weakens the immune systems of internally displaced people aids the development of respiratory and gastrointestinal diseases in immunocompromised children and elderly patients. Current confounding factors and unfavorable conditions for internally displaced people can further aggravate the prevalence of viral disease and ultimately lead to disease outbreaks in the susceptible population and a genetic mixing of pathogenic agents.
Terrorism
Underfunded and ill-equipped healthcare facilities due to the ongoing war and infrastructure collapse due to terrorist activities represent the biggest obstacles to health care for the people of Pakistan. No emergency medical services (EMS) exist in Pakistan, and initial help to victims is commonly provided by untrained but well-meaning people at the scene. 70 Attempts to eradicate viral diseases like polio and measles have been prevented by attacks by militants since 2012. The targeted killing of immunization teams in tribal areas and major cities in Pakistan pose a serious hurdle in the eradication of viral disease from the region. 71 In the past few years, a considerable decrease in terrorist activities has been reported, and the situation seems to be improving, but it still requires enormous effort to attain harmony.
Technical Capacity
Disease Surveillance and an Integrated Healthcare System
In Pakistan, a Disease Early Warning System (DEWS) was created in 2005 through the collaboration of WHO and the Federal Ministry of Health with the goal of early detection of infectious pathogens to reduce the morbidity and mortality rate; unfortunately, it was not implemented at the grassroots level. 69 Recent outbreaks of dengue and measles across the country raise questions about the efficiency of DEWS. 72 This failure also raises concerns regarding the country's preparedness for some highly pathogenic viral entities such as Ebola, measles, Marburg, and others that could be used as biological weapons. 73 Is Pakistan really prepared to cope with an emergency situation involving an infectious disease outbreak? The dilemma is not only restricted to natural outbreaks, but also bioterrorism attacks using engineered viruses by non-state agents cannot be ignored in the region. An integrated healthcare system at the grassroots level is needed to eradicate the menace of sudden outbreaks, and a proactive infectious agent alarm system is needed to cope with the threat of germ warfare.
The recent mission report (2016) of the Joint External Evaluation (JEE) of the International Health Regulations (IHR) in collaboration with the World Health Organization mentions some positive aspects of the healthcare system, but there are also areas of concern that need to be addressed. 74 The report indicated that some staff members in the provincial ministries lack the essential experience and background knowledge about health issues. Problems of coordination exist among human and animal healthcare departments. Adequate funding for the Ministry of National Health Services and allocation of a specific amount for implementation of health measures in the fiscal year can play a pivotal role in promoting health and well-being. Concerns exist over antimicrobial resistance, healthcare-associated infections, emergency response plans, surveillance, and prioritization of zoonotic pathogens. The mission also recommended a uniform implementation procedure for biosecurity and biosafety procedures across the country.
Legislation and Policymaking
The structure and function of the current healthcare system in Pakistan are far below international standards. Core health issues should be addressed through discussion with stakeholders to formulate a potential health policy that could be implemented at the grassroots level for efficient execution. Pakistan does not have an organized healthcare system; even health priorities are not properly defined. 75 Policies should be organized to ensure low-cost medicines and affordable treatment are available to everyone. Efforts in the past few years have resulted in improvement in coordination by developing online resources and databases for healthcare management and disease surveillance in Pakistan (Table 1). Self-reliance in pharmaceutical production is a step toward the reduction of health treatment cost. In Pakistan, the circulation of counterfeit medicines in the market is also on the rise; hence, the current scenario demands more transparency plus licensing and standardization in the pharmaceutical sector. Quackery, which should be considered a serious crime and eradicated, is further pinching our health system. Current public health education demands formulation of a national health education curriculum that will enable every citizen to understand the do's and don'ts of public health. 76
Online resources and database for healthcare management and disease surveillance in Pakistan. Information from both national and provincial levels is manipulated for coordinated efforts to find sustainable solutions to health problems caused by infectious and other diseases in the country.
The recent incidence of Middle East respiratory syndrome coronavirus (MERS-Cov), reported in 2012 in Saudi Arabia, took the lives of almost 500 people, demonstrating the need for the development of public policy. 77 Terrorism is not the only reason that such action needs to be taken. Emerging infectious diseases can arise from an innocent occurrence: Pilgrims will acquire the coronavirus in Saudi Arabia and bring it back to their countries. Proper screening protocols should be adopted for every person returning home from the Hajj in order to mitigate the risk of a coronavirus outbreak. Public health is vital for any modern state and is a moral obligation.
Infrastructure
Healthcare infrastructure in Pakistan is wide and diverse; it includes approximately 919 hospitals, 5,334 basic health units, 4,712 dispensaries, 288 tuberculosis centers, and 560 rural healthcare centers. 60 Recently, efforts are being pursued for proper coordination among all healthcare units, giving hope for full utilization of this infrastructure for disease surveillance.
The country spends almost 2.2% of its GDP in the health sector, while private spending as a percent of total spending is 61.5%. Per capita total spending on health is almost 59% (see Figure 3a). There are 8.13 doctors per 10,000 population. 78 To solve problems in the health sector, government designed a devolution plan in 2000 to completely reform the health sector and the social sector. This plan was focused on a transfer of power to the grassroots. According to the WHO report (2006), Pakistan is 57th globally in health staff deficiency. 79 This deficit is further aggravated by the lack of clear and well-defined health policies; formal training in the health sector is also deficient. The health infrastructure in Pakistan is continuously targeted by terrorists. About 29% of health facilities in Khyber Pakhtunkhwa (KP) have been damaged, while in Swat, 18 health facilities were affected, ultimately costing PKR 150 million.80,81 Damaged healthcare facilities, especially in the tribal areas, delay the treatment of infectious diseases, which could lead to the dissemination of infectious agents.
Future Outlook
The 2014-15 national health budget of Pakistan was released with huge expectations, but unfortunately the poor were once again neglected, with an insufficient budget of 26.80 billion rupees, which cannot provide healthcare services to 18 million Pakistanis. An insufficient amount—31 million rupees—was allocated for the prime minister's dengue and pollen allergy program. However, a substantial allocation of 63 billion rupees was made for promoting higher education, which will ultimately improve the capacity of health professionals. 82 Considering overall high costs and increased poverty, the health budget should have been increased for public relief and to guarantee health services to the ignored segments of our society.
Among the goals we must achieve for a healthy future is a healthcare provision system that is strengthened and implemented with a focus on the resources for health services (Figure 3b). The concept of free treatment should be converted to affordable treatment for everyone by developing national competencies for producing pharmaceuticals and medical equipment. Promotion of genuine research in the field of medicine will ultimately pave the way for potential inventions that have market value. A service carrier structure for doctors should be clearly defined, with proper mechanisms of accountability. The staff for an infection control program should be made part of the preventive health structure so that it can be used in a holistic and rapid response to emerging infectious diseases on all fronts.
These emerging infectious diseases may occur because of environmental factors such as climate change, global warming, and anthropogenic activities; Pakistan faces a huge challenge in conserving biodiversity resources. Loss of animal hosts can lead to the zoonosis of pathogens, which can lead to exotic epidemics. 83 Such infectious agents will be difficult to cope with because they exploit novel ways of approaching a human host. Use of a real-time environmental assessment in the current infrastructure at the grassroots level and in remote areas can curtail the chances of a novel epidemic. Biosensors pave the way for real-time, multiple analyses of viral pathogens. Training of medical personnel at all levels and in all sections of the country is essential for the general well-being of the people.
Another important issue in the fight against disease and its spread is in the area of public trust. In order to deal with healthcare issues, corruption must be stopped. It may be one of the major causes of not being able to deal with infectious outbreaks effectively. Pakistan has been declared to be among the leading countries with a corrupt system, which directly affects the provision of healthcare for the country. Corruption is on the rise in every aspect of health care, including drug pricing, funds allocation, and the like, ultimately leading to a fragile healthcare system in Pakistan.
Finally, another factor hindering a flourishing healthcare system is the lack of public-private partnerships, which should be strengthened to make primary healthcare facilities available to the common people of the country.
Conclusions
The failure to achieve a good healthcare system has resulted in Pakistan being a reservoir for infectious diseases, like polio, which have elsewhere been wiped from the face of the earth. Besides the endemic entities, there is a global threat of Ebola virus that demands serious and dedicated efforts to be undertaken at federal and provincial levels, with effective participation from civil society and religious scholars. Zika virus is among the heavily debated issues across the world. Recent statements by the health ministry and WHO indicated that the risk of a Zika virus outbreak is insignificant. Even if there is a low risk, there is a great need to monitor the virus globally and respond immediately if a suspected Zika case is found in the country. An outbreak response and implementation strategy should be immediately developed against pathogens like Ebola, Zika, and MERS.
At present, Pakistan may not have the capacity to deal with these issues by itself, so efforts are required by the international community to reduce the existing threat of emerging infectious diseases. The emergency response teams should be properly trained and equipped to respond to any event. Biosecurity issues must be taken care of. Poor and slow response to natural disasters like floods and earthquakes should be improved. A dedicated, well-planned, integrated effort at all levels of society is needed to cope with the menace of infectious diseases.
Footnotes
Acknowledgments
The authors are grateful to Dr. Kafeel Ahmad, Assistant Professor, Centre of Biotechnology and Microbiology, University of Peshawar, Pakistan, for his valuable suggestions. The authors declare no conflicts of interest.