
Abstract
Countries around the Mediterranean Sea share epidemiologic characteristics and public health problems. From 2007 to 2013, a Mediterranean collaborating framework called the EpiSouth Network was established to share knowledge and develop joint activities. Under the coordination of the Italian National Public Health Institute (ISS), this network implemented 2 projects, the first focused on communicable disease surveillance and training and the second on strengthening preparedness for common health threats and biosecurity risks. After the first 3 years of activity, the network included public health institutes, ministries of health, and laboratories of 27 countries in southern Europe, the Balkans, North Africa, and the Middle East. The network worked in collaboration with and with the support of the European Commission, the European Centre for Disease Prevention and Control, the World Health Organization, and the Italian Ministry of Health. This article provides an overview of the key strategic approaches and achievements of this regional network, as well as its impact on public health policies and current projects. Through this example, we discuss how regional collaborative networks can contribute to the development of public health policies on the control of cross-border public health threats.
Countries around the Mediterranean Sea share epidemiologic characteristics and public health problems. From 2007 to 2013, a Mediterranean collaborating framework called the EpiSouth Network was established to share knowledge and develop joint activities.
C
In practice, however, developing a regional Mediterranean collaboration mechanism to ensure timely sharing of information and coordinated preparedness and response activities is complicated. Countries bordering the Mediterranean basin are included in 3 World Health Organization (WHO) regions, and only some are member states of the European Union (EU). There is only 1 common international legislative framework to facilitate collaboration and communication in the Mediterranean region—the WHO International Health Regulations (IHR) 4 —while EU member states also operate under the framework of the EU Early Warning and Response System. 5
A possible role for regional networks in the trans-boundary landscape of emerging public health threat detection and control has been introduced in article 44 of the IHR. A similar message from an animal health perspective was relayed by the Food and Agriculture Organization in a position paper on regional networks in 2010. 6
Nevertheless, there is a lack of evidence on what network governance models could best favor the development of ideas and activities and foster respect and mutual trust. There is no consensus on which working strategies are more appropriate to enable networks to contribute to health policy outcomes. It is also unclear which evaluation methods could be best suited to assess the networks' impact and added value in those fields.
A Mediterranean collaborating framework, called the EpiSouth Network, was established in 2007, and it implemented 2 projects. The aim of the first, the EpiSouth project (2007-2010), was to create a framework of collaboration on epidemiologic issues to improve communicable disease surveillance, communication, and training across the countries of the Mediterranean and the Balkans. 7 The second project, EpiSouth Plus (2010-2013), 8 had a broader approach aimed at enhancing and strengthening preparedness for common health threats and biosecurity risks at national and regional levels, within the framework of IHR.
Looking back at the 7 years of the EpiSouth Network's activity, this article provides an overview of the key strategic approaches and achievements of this regional network, as well as its impact on public health policies and current projects.
Methods
In 2004, experts from Spain, Bulgaria, Greece, France, and Italy, collaborating in relevant initiatives in the Mediterranean region like the WHO Mediterranean Zoonoses Control Programme, 9 designed a cooperative framework to address common Mediterranean health priorities such as cross-border early warning and epidemic intelligence and preparedness for emerging zoonosis. These core countries proposed the EpiSouth project to the other countries of the Mediterranean and Balkan region and to the EC for funding in 2005, the Year of the Mediterranean. The project (2006-2010) was approved in the European program of community action in the field of public health under the priority area “Responding rapidly and in co-ordinated fashion to health threats.”
EU member states and nonmember states of the Mediterranean basin and Balkans were included in the initiative. The European project supported only the participation costs of the EU member states. The Italian Ministry of Health provided funds for the nonmember states.
During the project implementation, the EpiSouth Network consolidated, and a second project, EpiSouth Plus (2010-2013), was developed and co-financed by the EC Public Health Programme and the EC Instrument for Stability under the Directorate General of International Cooperation and Development. Directorate funds supported the participation of EU nonmember states with the collaboration of the Italian Ministry of Health.
Network Development
Structure and Governance
Based on lessons learned from prior initiatives,10-14 the EpiSouth coordination team designed a structure for the governance of the network, which was shared with the steering committee and then with the countries' representatives during the first network meeting, held in March 2007. The coordination team and the steering committee shaped the EpiSouth Network around the definition coined by Chisholm in 1998, which identifies a network as “a set of autonomous organizations that come together to reach goals that none of them can reach separately.” 10
Coordination
The coordination team addressed aspects related to sustainability and visibility and reported about the network, with the support of the project activity leaders (work packages' leaders), in national and international workshops and seminars. The coordination team also ensured the framework of collaboration and information exchange among the participating countries by organizing network meetings and the projects' websites, 8 the projects' schedules, and the quality of the projects' outcomes. The network and its activities were coordinated initially by 1 EU member state's public health institution with scientific advice from an advisory board and technical support from a steering committee. Starting from EpiSouth Plus, 1 EU member state and 1 nonmember state institution shared the coordination tasks.
Steering Committee and Advisory Board
The steering committee included the project leader and the work packages' leaders. Representatives from institutions and organizations (eg, WHO, the EC, the European Centre for Disease Prevention and Control [ECDC], and other international organizations) relevant to the network's activities were part of the steering committee. In EpiSouth Plus, the steering committee agreed that representatives of institutions and external experts not involved in the projects' activities should be external to the steering committee, and, therefore, they were invited to join an advisory board established for this purpose in 2010.
Technical Leadership and Countries' Participation
Both EpiSouth projects were implemented through work packages. During EpiSouth Plus, work package co-leadership was introduced: each work package was headed by 2 co-leaders (1 from an EU member state and 1 from a nonmember state or an international organization), both members of the EpiSouth Network. To enhance the participation of the countries, each work package leader established a steering team of 5 to 9 partner countries.
Network Participants
The public health institutes or ministries of health of the EU member states from southern Europe were the original core of the EpiSouth Network. Representatives of public health institutes and ministries of health from 18 nonmember states surrounding the Mediterranean basin were invited to the first network meeting in March 2007 to be informed about the network establishment and its activities. The involved countries were represented by 2 focal points, who were officially appointed by the relevant countries' authorities.
Participation in network activities was voluntary. Staff from participating countries were not paid for their contribution. However, all costs related to their involvement were paid by the projects. The focal points were involved in work package steering teams according to their interests, needs, and capacities. All focal points met during the network meetings. These meetings addressed governance, sustainability, and specific technical topics related to the project activities.
Mediterranean Regional Laboratory Network
During the EpiSouth Plus project, based on the recommendations of the network's members, the Mediterranean Regional Laboratory Network (MRLN) was established. The MRLN worked alongside the EpiSouth Network but had its own specific activities, including training of laboratory staff to build capacity in diagnosing emerging zoonoses and in biosafety as part of lab biosecurity measures. 15
Implementation Strategy
An implementation strategy was proposed by the coordination team and developed with the support of the steering committee. The network had to be ready for big challenges: It had to accomplish the objectives set by the projects, which were intrinsically connected with the strength and capacity of the countries to work as a network (ie, the focus was on cross-border activities). Therefore, it needed to consolidate the network with an appropriate methodology while performing the project activities. The countries' representatives had to communicate and share experiences, participate in the activities, and perceive the priorities set by the projects as in line with their national priorities to ensure that the projects' achievements could be considered valuable and worthy contributions to national and international policies.
Because of the number and diversity of countries involved in the EpiSouth Network, it was critical to converge the national priorities of 27 countries toward common regional priorities. In fact, cross-border needs may sometimes identify priorities that might not yet have been identified at the national level (eg, capacities in monitoring potentially threatening events in the neighborhood; operational multi-country frameworks to respond to threats; harmonized preparedness plans, etc). The methods used by both projects to set regional priorities for action included needs assessments, prioritization exercises, context analysis, and consensus workshops. These methods, extensively used in other contexts, were adapted to the EpiSouth Network's specific needs.16-18
On the basis of the identified regional priorities, the work packages set capacity building targets and/or identified areas to further investigate through studies aimed at analyzing specific issues and providing contextualized recommendations. Ensuring a long-lasting impact was identified as a priority. For this reason, critical aspects, like sustainability, were also included in the implementation strategy.
Intervention Sectors
The work packages implemented activities in the sectors of capacity building (epidemiology and laboratory training), cross-border epidemic intelligence, early warning, and IHR implementation.
Capacity Building
The activities were aimed at reinforcing capacities on preparedness with a cross-border and multisector focus for both epidemiologists and laboratory staff. The steering committee developed a capacity-building process that started with identifying training needs, followed by implementing workshops and training sessions and elaborating a tool, and ended with conducting a simulation exercise to consolidate the cohesion of the network and to assist countries in testing their level of preparedness (Figure 1).

Capacity-Building Process
Epidemiology Training
A training needs assessment was conducted during the EpiSouth project and led to the identification of the following topics: epidemiologic analysis of surveillance data, epidemic intelligence and IHR, emerging infectious disease control, and outbreak management and communication. 16 The second training needs assessment, conducted during the EpiSouth Plus project, identified the following topics: generic preparedness planning and development of emergency preparedness plans, communication in public health emergencies, risk assessment, and spatial cluster analysis on surveillance data. 17 To better connect the training sessions with national priorities, each training session was preceded by a 2-day workshop in which participants had the opportunity to share and discuss with colleagues their national policies and procedures as well as their personal previous experiences in the training topics.
Laboratory Training
Laboratory training priorities were identified through several phases. During the inception phase of the EpiSouth Project, the core-involved EU member state countries identified the control of cross-border emerging zoonoses, using a multisector approach (ie, collaboration between human and veterinary public health), a common priority for the Mediterranean area. During the implementation of the EpiSouth Project, the relevant work package steering team carried out an assessment (2007) to identify which priority emerging zoonoses were particularly in need of multisector collaboration in the countries of the region. The questionnaire included indices of disease emergence (ie, increased incidence in humans, spread of the disease in novel geographic areas, detection of the pathogen in novel animal species) and of surveillance needs (ie, absence of surveillance systems, human or zoonotic; necessity for improvement of intersectoral collaboration). 16
In 2011, during EpiSouth Plus, the work package steering team representing the MRLN, on the basis of the above-mentioned prioritization, identified a set of topics to be addressed in the training sessions in accordance with national relevance for diagnostic capacities and cross-border and networking activities. Specific training needs were assessed accordingly. 18
Cross-Border Epidemic Intelligence and Early Warning
To facilitate early detection of potential cross-border threats, an early warning system is needed, 19 and it needs to be based on epidemic intelligence activities. * All EU member states and the majority of nonmember states have long-established disease surveillance systems that provide proper indicator-based surveillance data. For most countries, the challenge lies in developing and structuring the event-based † component of epidemic intelligence in national institutions in charge of public health surveillance. The relevant work package leader, with the support of the work package steering team, developed a stepwise process to strengthen early warning capacities in this region with the support of a project-secure platform for information exchange.
Regional needs for early warning were assessed, and consensus among participating countries was reached for the working definitions of epidemic intelligence and cross-border epidemic intelligence. ‡ At the beginning of the network's activities, the focus was on epidemic intelligence with a global perspective, in order to familiarize participants with the concept, tools, and outputs of event-based surveillance. Later the focus shifted to cross-border epidemic intelligence, focusing on events occurring within the Mediterranean region.
Analysts of the work package steering team monitored health events using event-based surveillance.19-21 Validation of events occurred through the project-secure platform and calls. The main objective of the secure platform was to allow the exchange of information that (1) did not respond to mandatory notification criteria, and/or (2) would not be readily shared through existing information exchange systems to all the project partners. The platform acted in synergy and conjunction with all relevant mandatory notification systems (EWRS and WHO-IHR).
The electronic Weekly Epi-Bulletin (e-WEB) was used to publicly disseminate the results of the early warning system. E-WEBs included global information captured through epidemic intelligence activities and, since the summer of 2008, validated health events occurring within network countries or across their borders. In addition, in-depth thematic notes were prepared on issues of particular interest to the network.
IHR Implementation
The relevant work package steering team analyzed WHO data with the identification of priority areas for intervention 22 that supported the final decision on the priority area for EpiSouth during a consensus workshop with the relevant leadership, work package steering team members, and representatives of the network. This area was studied in depth using a situation analysis methodology, designed in close collaboration with WHO, in 4 partner countries. This study was called the EpiSouth National Situation Analysis (ENSA) study. 23
Monitoring and Evaluation
To reduce conflict of interest, the monitoring and internal evaluation was led by the only institution not involved in the management and implementation of activities. This work package monitored the development and consolidation of the network during the first project through questionnaires submitted to all participants during the network meetings. The team assessed whether the participants had understood and shared the network's purpose and goals and whether they felt they were part of it (network's membership). In addition, aspects related to communication (ie, mechanisms for providing feedbacks to all the members), governance (ie, decision taken process, distribution of leadership, management of conflicts), the network's added value (ie, the use of network members' skills, support from other members, level of cohesion), and opportunities (ie, capacity for creativity and growth, risk taking) were assessed. During EpiSouth Plus, the internal mid-term and a final evaluation were carried out by a contractor.
Main Results and Achievements
Network Development
Structure and Governance
The network was structured according to the model shown in Figure 2. Each component of the structure met in specific contexts (left part of Figure 2) and was interacting with the others as per its role.
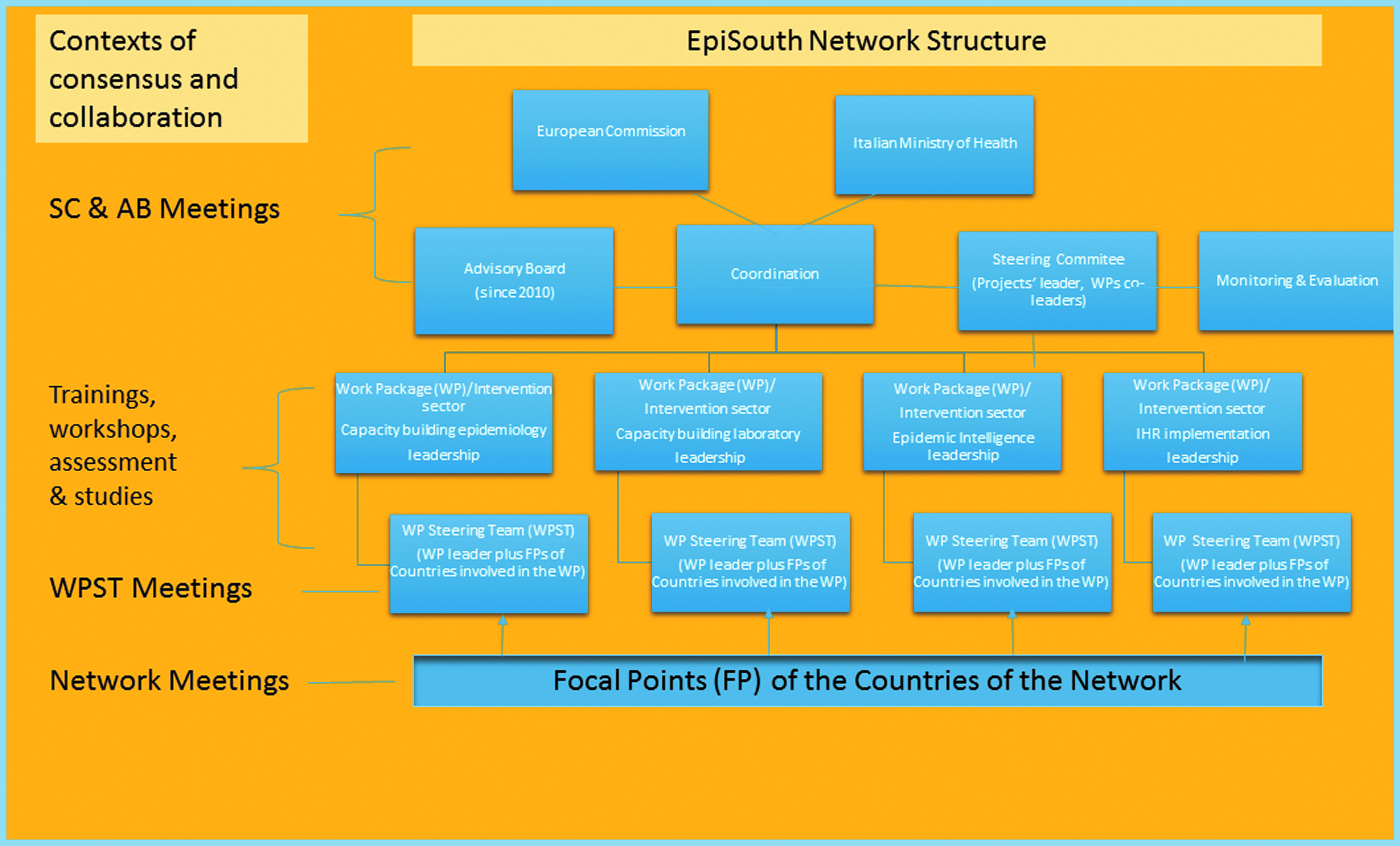
EpiSouth Network Structure
Coordination
During the first project, the coordination team with the steering committee devoted most efforts and resources to the establishment of the network and its consolidation. This included the organization of 4 network meetings in 2007, 2009, and 2010 involving 225 focal points. During the second project, there were 2 network meetings, in 2012 and 2013, involving 159 focal points, in favor of technical meetings focusing on specific project activities (Figure 3). The network strategies and lessons learned were reported to EC bodies and international institutions in several technical meetings on cross-border health threats and health security. 24
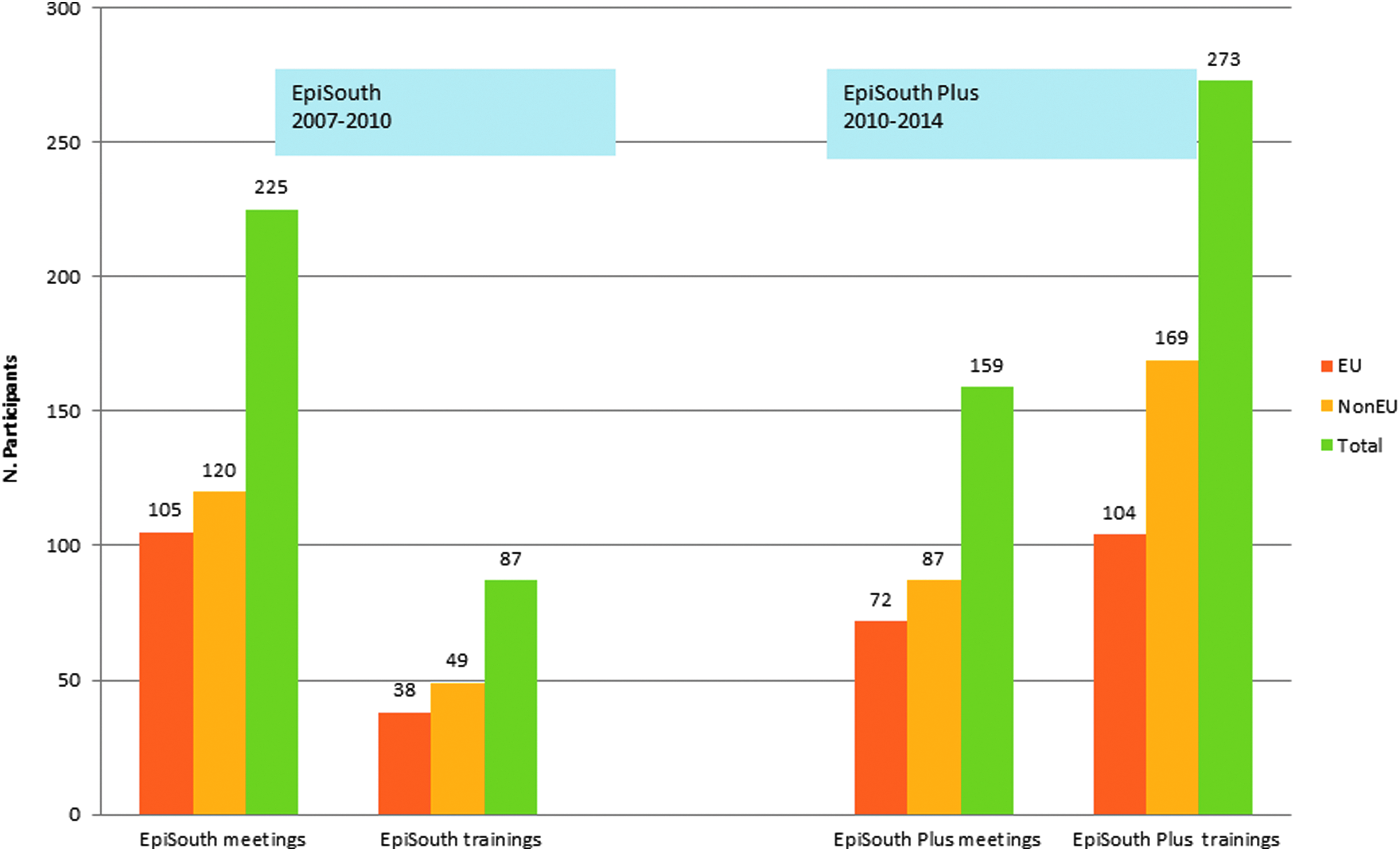
Meetings and Training Sessions of EpiSouth and EpiSouth Plus Projects, 2007-2014
Steering Committee and Advisory Board
The coordination team asked relevant institutions and organizations to formally appoint 1 representative for the advisory board and countries of the network to recommend expert(s) to be included in the advisory board. The advisory board was composed of 18 members: 13 experts from collaborating institutions and 5 recommended by the participating countries. The steering committee and advisory board met at least once per year.
Technical Leadership and Countries' Participation
Each work package steering team identified the regional priorities for the related sector of intervention and developed the needed tools and the conducive environment to meet the objectives and requirements. The work packages' leaders organized work package steering team meetings that were implemented with the collaboration of the work package steering team members and held in different countries of the network or during ad hoc sessions of the network meetings.
Network Participants
Upon its approval in 2007, the EpiSouth Network included 9 EU member states: Italy, France, Spain, Bulgaria, Greece, Romania, Slovenia, Cyprus, and Malta. After the first project meeting in March 2007, 13 interested non-EU member states were formally invited to appoint 2 focal points to be part of the network. The focal points were all working at the national level (in the ministry of health or in the public health institute) on preparedness and risk management of communicable diseases and other public health threats. Preferably, EpiSouth focal points were also working as IHR and/or EU early warning and response system focal points. The network subsequently expanded to 27 countries, including 10 EU member states (Bulgaria, Croatia, Cyprus, France, Greece, Italy, Malta, Romania, Slovenia, and Spain) and 17 non-EU member states from southern Europe, the Balkans, North Africa, and the Middle East (Albania, Algeria, Bosnia and Herzegovina, Egypt, former Yugoslav Republic of Macedonia, Israel, Jordan, Kosovo, Lebanon, Libya, Montenegro, Morocco, Palestine, Serbia, Syria, Tunisia, and Turkey). By October 2010, all these countries had officially appointed 74 focal points.
Mediterranean Regional Laboratory Network
By the end of July 2013, the national reference laboratories for arboviruses of 24 countries § of the EpiSouth Network were represented in the MRLN. 25 They met during 2 coordination meetings (held in 2011 and 2012, involving 32 laboratory representatives) to identify priorities and needed expertise. They also participated in training sessions (see below), exchanged expertise, and came in contact with other laboratories and networks identified as relevant for EpiSouth's activities. 26
Implementation Strategy
Specific methodological objectives were identified to be achieved with specific strategic approaches (Figure 4). One of the methodological objectives was to strengthen EU and non-EU country collaboration. This was fostered using several strategic approaches: the establishment of an early warning project secure platform, the establishment of joint leaderships, the identification of “regional” priorities, and the design of tailored training sessions. Also, the visibility and relevance of the network was a methodological objective, and, in order to ensure it, the network's activities and strategies had to be reported at technical meetings, at national and international levels. This would have, in our view, also showed the network's potential and increased its sustainability.
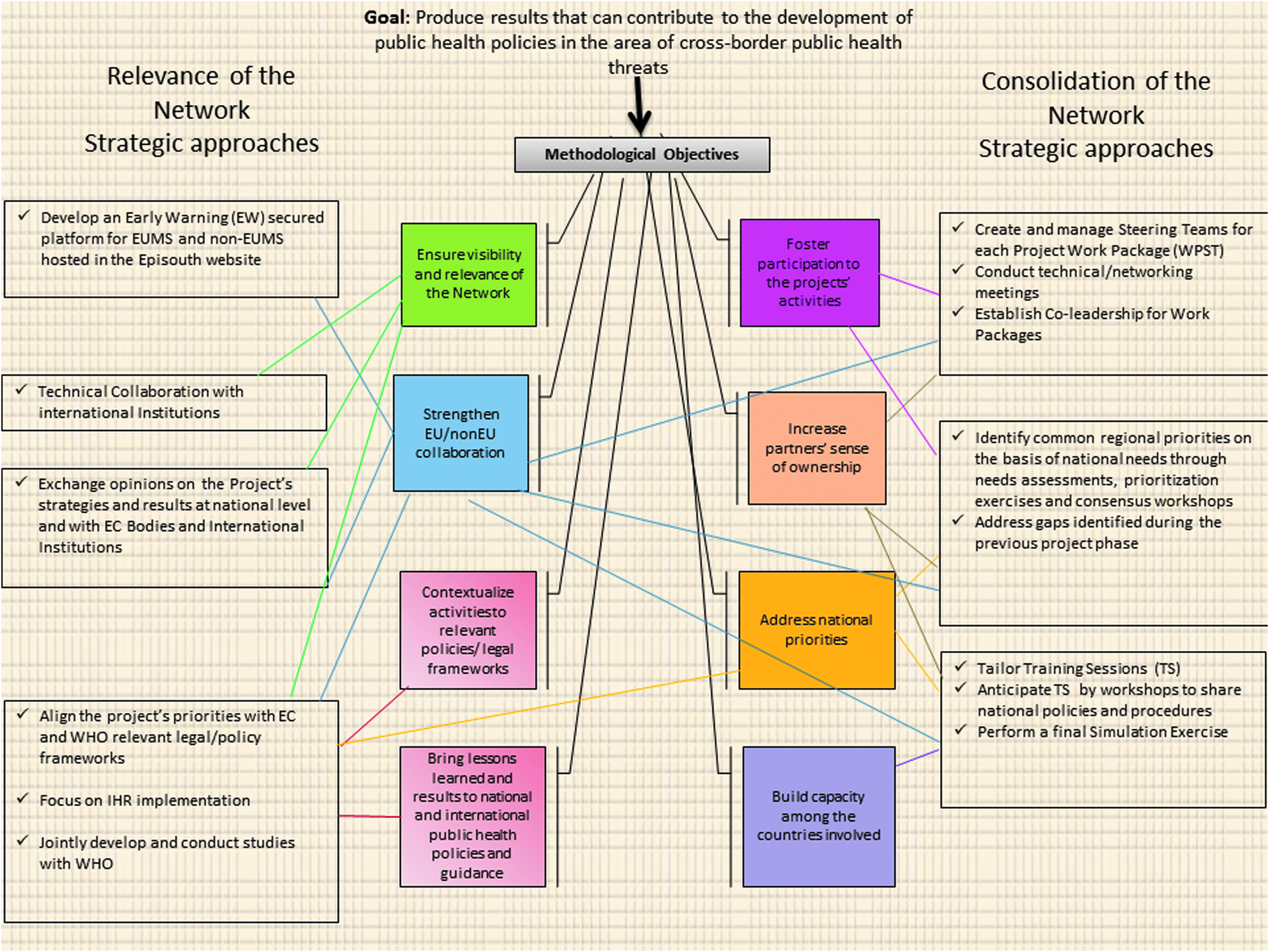
EpiSouth Implementation Strategy
The implementation strategies and the results achieved by the EpiSouth projects (Table 1) were shared and discussed with the partners from a regional health policy perspective to produce strategic guidance documents for the region, called EpiSouth strategic documents.27-31
Intervention Sectors and Results Achieved by the EpiSouth Projects
Sectors of Intervention
Capacity Building
As shown in Figure 3, training activities increased during EpiSouth Plus. In this project, a total of 273 participants (104 from EU member states and 169 from non-EU member states) benefited from capacity-building activities, compared with 87 during EpiSouth.
Epidemiology Training Sessions
During EpiSouth, 3 training sessions on field epidemiology were conducted in 2007, 2008, and 2009, involving 87 participants (38 from EU member states and 49 from non-EU member states). During EpiSouth Plus, 4 field epidemiology training sessions (in 2012 and 2013) were implemented involving 90 participants (28 from EU member states and 62 from non-EU member states).
To reinforce capacity in generic preparedness, an emergency preparedness planning tool was developed by the relevant work package steering team. 29
The capacity-building process culminated in October 2013 with a simulation exercise called “Nautilus.” Nautilus was designed as a command post exercise. One national evaluator was present in each participating country, and 1 external evaluator was present in the crisis room of the coordination center for public health alerts and emergencies at the Spanish Ministry of Health in Madrid (the command post). The WHO headquarters offices in Lyon and Geneva, ECDC, and EC-DGSANCO–C3 supported its organization and implementation. Twenty countries and 250 staff were involved in the simulation exercise, and 80 people trained for the implementation. The exercise was evaluated and was deemed successful in testing national core capacities in emergency preparedness and response and identifying opportunities for improvement. 32
Laboratory Training Sessions
The priority topics identified for the training sessions were West Nile virus, dengue, and biosafety. The training on dengue and biosafety 33 was attended by representatives from 17 laboratories (7 EU and 10 non-EU); the training on West Nile virus and biosafety 34 was attended by representatives from 20 laboratories (7 EU and 13 non-EU). Not all the non-EU laboratories could participate due to difficulties in obtaining travel visas on time for the proposed participants.
Cross-Border Epidemic Intelligence and Early Warning
A secure platform was developed and made operational at the end of 2009. From November 2009 to April 2013, 156 events were shared through the EpiSouth secure platform. Of these, 133 (85%) of the shared events focused on EpiSouth countries and 46% on vector-borne diseases. From March 2008 to October 2013, 264 weekly issues of the EpiSouth e-WEB and 14 thematic notes were published on the EpiSouth Network website. 35 Four residential stages on epidemic intelligence involving 12 participants (5 from EU member states and 7 from non-EU member states) were also implemented. 36 Figure 5 shows the main milestones of the process to enhance awareness and capacities on cross-border epidemic intelligence and early warning and the main outputs produced.
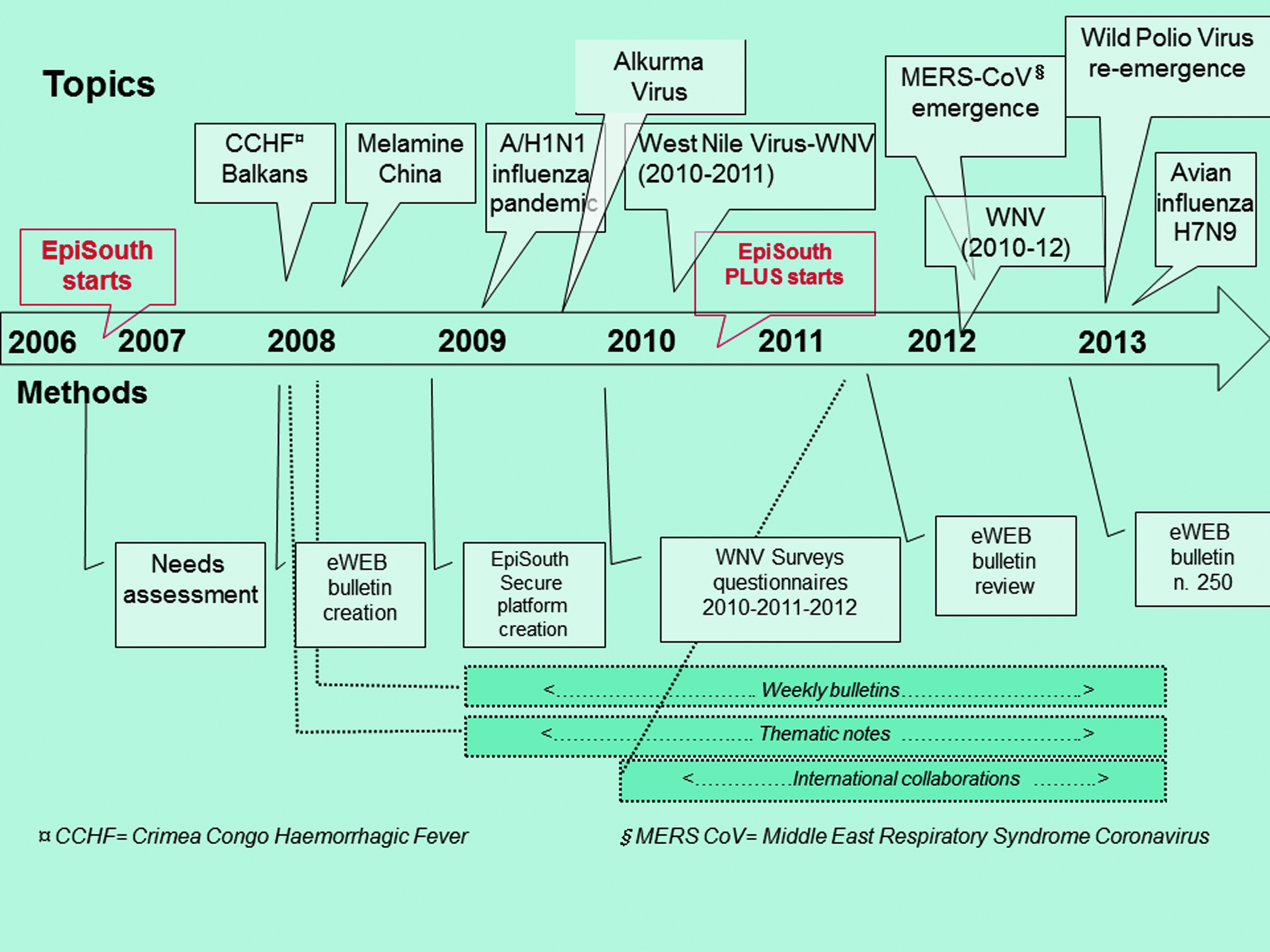
Cross-Border Epidemic Intelligence and Early Warning Milestones
The information and data provided with the e-WEB bulletins and thematic notes were widely disseminated and captured the attention of international institutions that cited EpiSouth as a source in their reports and early warning bulletins or articles;37-39 the work package steering team was also consulted for risk assessments. 40
IHR Implementation
Enhancing the coordination of surveillance between points of entry ** and the national health systems in the Mediterranean region was the most relevant gap identified by the work package steering team. 41 This gap was filled by the analysis of coordination of surveillance and response between points of entry and national health systems in the EpiSouth Region (review of relevant scientific literature and of existing monitoring) 42 and by the ENSA study involving Italy, Malta, Jordan, and Morocco. 43 Based on the overall findings, EpiSouth defined 4 strategic lines for improving surveillance coordination at points of entry in the Mediterranean: (1) invest in a legal framework linking IHR national focal points with competent health authorities; (2) ensure the presence of competent health authorities at points of entry; (3) elaborate on or update relevant protocols, processes, and procedures; and (4) ensure, through training, correct and consistent application of protocols, processes, and procedures. 30
Monitoring and Evaluation
The assessments of the consolidation of the network during the first project showed the aspects to be further strengthened.44,45 This guided the action of the coordination team.
The EpiSouth Plus project was evaluated with a mid-term 46 and a final evaluation, 47 with questionnaires and interviews to internal (leaders and participants) and external (advisory board members, representatives of collaborating institutions, etc) stakeholders. The evaluations focused on many aspects, assessing in particular the achievements in terms of future sustainability and strengthening of collaboration between the EU and non-EU member states.
The EC Directorate General of International Cooperation and Development evaluated EpiSouth Plus, through contractors, using results-oriented monitoring in 2011 and, in the framework of the evaluation of the Instrument for Stability, in 201248 and 2015.
The project was considered highly relevant, not only for the instrument for stability but also for the public health security of the EU itself, with regard to the acquisition, validation, and sharing of epidemiologic intelligence. In particular, the discussion of the results of the monitoring and evaluations during steering committee meetings and workshops that involved the participating partner countries was appreciated.
Finally, the establishment of a “sustainability plan” was positively underlined. This transition planning involved, among other factors, the identification of key outcomes (ie, systems, tools, protocols for information sharing and alert features, infrastructure) that needed to be continued and preserved even after external funding ceased. The use of experts and expertise from within the network, to reduce dependence on external expertise and support, and the mobilization of alternative funding sources, both within the partner countries involved in the network and outside, were identified by the Directorate General of International Cooperation and Development evaluation as relevant measures for sustainability.
Discussion
A cornerstone of the EpiSouth Network's success was the focus on national needs and regional common priorities to enhance participation and ownership and consequently consolidation of the network, which was critical for the achievement of the projects' aims. However, identifying those priorities in such a large network of countries not used to working together was complex.
The projects had a strong focus on “cross-border” health threats, so the priority was to cover gaps and needs to strengthen collaboration between countries, increase exchange of data and information, and implement IHR, in order to be prepared for possible cross-border threats. Sometimes these aspects were not initially perceived as national priorities, and there was no preexisting agreement on what should be considered a regional cross-border health threat. Formal prioritization and needs assessment processes were key to overcoming this initial uncertainty and to creating a regional perspective.
It was also very useful to engage relevant institutions in this process and to be engaged as EpiSouth (through the project work package steering team) in the WHO expert consultation to develop guidance on coordination between points of entry and the national health system in Lyon in 2012. 49
The fact that the network was increasingly invited to report about its strategies and lessons learned in conferences and workshops by the EC, the ECDC, and WHO, and was requested to provide information and insights on international risk assessments,24,40 was, in our view, indicative of its growing credibility and, in turn, enhanced its sustainability.
The network also faced numerous challenges. The concomitant participation of EU and non-EU member states, undoubtedly the main strength of the initiative, complicated the administrative and legal framework. Aspects related especially to fund eligibility (as mentioned, not all the European programs can support costs of non-EU partners) and to legal obligations for the exchange of confidential information (under specific legislation frameworks)4,5 on cross-border health threats, had to be considered and overcome.
Flexibility was needed to favor the participation of partners in fragile contexts (eg, significant internal upheaval and social instability). During the Arab Spring (2011), the coordination team was forced to rearrange schedules and locations, with some delays in implementation. Nevertheless, the network continued to work. Showing that the project advanced successfully, even with defensible modification, was considered one of the best tools to gain credibility vis-à-vis the current and future supporters and funders. 48
Finally, evaluating the impact during each project implementation, as required by the funding agencies, was extremely challenging. First, looking at each project separately did not take into account the network's life span nor measure its long-term impact. Second, appropriate methods and indicators are lacking to evaluate the level of trust created and the countries' sense of ownership, to quantify the contribution of networks to regional security and stability, and to identify their role in the development of international health policy outcomes.
Notwithstanding these methodological challenges, there are indications of the impact of the EpiSouth Network on public health policy at national and international levels. The capacity-building process enhanced the countries' awareness of the relatively new concepts of epidemic intelligence and generic preparedness, stimulating the development of spontaneous related initiatives at the national level.50,51
On the basis of EpiSouth's situation analysis and studies, and having consulted all WHO regions, WHO concluded that coordination of surveillance with points of entry was not only a priority for the Mediterranean region but also a global priority, and it developed WHO global guidance on this topic. 52 This guidance cites the work of the EpiSouth Network and recommends using national situation analysis for national assessments. The lines of interventions set and implemented by EpiSouth have been recognized as strategic to reinforcing health policy indications on regional preparedness to cross-border health threats in the EU neighborhood. 53
EpiSouth was recognized as the largest collaborative health network in the Mediterranean, and its added value was recognized and rewarded with the 2014 European Health Award as “the Mediterranean project to counteract cross-border threats to health.” 54
These achievements confirm, in our opinion, the relevant potential of regional networks in building capacity, developing common technical understanding, consolidating trust, and providing guidance for regional strategies.
EpiSouth also promoted new regional initiatives and strategies that are now expanding. For example, the need for intersectoral collaboration to cope with cross-border emerging zoonosis, supported by EpiSouth since 2010, is now being enhanced with the MediLabSecure project.55-57 This project, aimed at reinforcing the One Health policy, involves former EpiSouth epidemiologists and laboratory experts in addition to experts from other critical sectors (eg, veterinary medicine and entomology).
Former members of the EpiSouth Network are also involved in the Mediterranean Programme for Intervention Epidemiology Training (Medipiet), which builds on approaches and tools developed by EpiSouth and is reinforcing cooperation between the EU and neighboring countries located along the shores of the Mediterranean Sea. 58 The network is now also engaged in other common priorities, like migration, which has been affecting the Mediterranean and Balkans since 2011. 59
While further research is needed to define quantitative tools and qualitative frameworks to measure and assess the effectiveness of network management models and implementation strategies, we believe that EpiSouth provides evidence of how regional collaborative networks can contribute to shaping international health policy in specific sectors.
Footnotes
Acknowledgments
The authors would like to thank Germain Thinus, European Commission Directorate General for Health and Consumers (SANCO); Cinthia Menel Lemos, Executive Agency for Health and Consumers (EAHC); Philippe Servais and Simonetta Riva, European Commission—EuropeAid Development and Cooperation Directorate-General (DEVCO); and Dr. Stefania Salmaso, head of the National Centre for Epidemiology, Surveillance and Health Promotion (Italy), for their constant support of the EpiSouth Network. The authors also thank all the people who throughout the years have contributed to the work of the network: the EpiSouth Network Focal Points, the EpiSouth Network Advisory Board, and the EpiSouth Network Secretariat (![]() ).
).
The cost of publication of this article is being covered by the European Health Award received by EpiSouth Plus Project. The EpiSouth network was co-funded by the European Union DG-SANCO/EAHC and DEVCO/EuropeAid, together with the Italian Ministry of Health. The contents of this manuscript are the sole responsibility of the authors and can in no way be taken to reflect the views of the funding institutions.
The EpiSouth Working Group:
Giovanni Putoto, Azienda Ospedaliera di Padova, Italy; Cinzia Montagna, Azienda Ospedaliera di Padova, Italy; Fernando Simon Soria, Instituto de Salud Carlos III/Ministry of Health, Madrid, Spain; Conception Martin Pando, CIBER Salud Pública Instituto de Salud Carlos III, Madrid, Spain; Rosa Cano Portero, CIBER Salud Pública Instituto de Salud Carlos III, Madrid, Spain; Danijela Simic, Institute of Public Health of Serbia “Dr. Milan Jovanovic Batut,” Belgrade, Serbia; Djohar Hannoun, Institut National de Santé Publique, Alger, Algeria; Philippe Barboza, Institut de Veille Sanitaire, Paris, France; Fatima Aït-Belghiti, Santé Publique France, Paris, France; Mira Kojouharova, National Center of Infectious and Parasitic Diseases, Sofia, Bulgaria; Rengina Vorou, Hellenic Center for Disease Control and Prevention, Athens, Greece; Giuseppe Salamina, ASL TO1, Torino, Italy; Kathleen Victoir, Institut Pasteur, Paris, France; Gulay Korukluoglu, Public Health Institution of Turkey, Ankara, Turkey; Alex Leventhal, Ministry of Health, Jerusalem, Israel; Mohamed Husein Adel Belbeisi, Ministry of Health, Amman, Jordan; Asa'd Ramlawi, Ministry of Health, Ramallah, Palestine; Pierre Nabeth, WHO Health Emergencies Programme, Lyon, France.
*
Epidemic intelligence encompasses all activities related to early identification of potential health hazards, their verification, assessment, and investigation in order to recommend public health control measures. 20
†
Epidemic intelligence integrates both an indicator-based and an event-based component. “Indicator-based component” refers to structured data collected through routine surveillance systems. “Event-based component” refers to unstructured data gathered from sources of intelligence of any nature. 19
‡
Epidemic intelligence:“monitoring of health events occurring outside the EpiSouth geographic area but possibly affecting EpiSouth countries”; cross-border epidemic intelligence: “monitoring of health events occurring within the EpiSouth area for early warning and information sharing.”
§
Albania, Algeria, Bosnia and Herzegovina, Bulgaria, Croatia, Cyprus, France, former Yugoslav Republic of Macedonia, Greece, Italy, Israel, Jordan, Kosovo, Lebanon, Libya, Malta, Montenegro, Palestine, Serbia, Romania, Slovenia, Spain, Tunisia, and Turkey.
**
Point of entry in the IHR context: “a passage for international entry or exit of travellers, baggage, cargo, containers, conveyances, goods and postal parcels, and the agencies and areas providing services to them upon entry or exit,” including ports, airports, and ground crossings.