
Abstract
In 2006, China targeted measles for elimination by 2012, but the goal was not achieved. In line with this goal, the timeliness of measles laboratory reporting should be evaluated to improve efficiency in implementing control measures. Laboratory-confirmed suspected measles cases reported to the measles surveillance system in Zhejiang Province, China, from 2009 to 2015 were collected. Three reporting periods were defined: transport duration (period from serum collected to serum received in lab), analysis duration (period from serum received to the result being reported), and total reporting duration. The median was calculated for each period. Associations between total reporting delay and other factors were accessed using logistic regression model. A total of 18,518 laboratory-confirmed suspected measles cases were collected. For transport duration, the median was within 1 day, and no variation was observed among different years. For analysis duration, the median decreased from 3 days in 2009 to 1 day in 2015. For total reporting duration, the median decreased from 5 days in 2009 to 2 days in 2015. The median of total delay was 13 days during the 7 years. The proportion of cases notified within the time limit was found to increase, indicating a tendency toward more efficient laboratory reporting. Moreover, timeliness was influenced by various external factors: reporting from CDC, reporting from counties with higher economic status, and reporting in spring were the variables associated with shorter delays. Timeliness of measles laboratory reporting has increased annually in China. Health administration departments need to pay more attention to measles laboratory surveillance in counties with lower economic status.
China targeted measles for elimination, but the goal has not been achieved, so the authors evaluated the timeliness of measles laboratory reporting. Laboratory-confirmed suspected cases reported to the measles surveillance system in Zhejiang Province, China, from 2009 to 2015 were collected. Timeliness of measles laboratory reporting was shown to have increased annually in China.
T
In 2006, China targeted measles for elimination by 2012. To achieve this goal, a national case-based system of measles surveillance was established in 2009, which has served as one of the web-based notifiable disease reporting systems all over the country. 3 The system users are those people who report suspected measles cases or use surveillance data, including clinical practitioners and Centers for Disease Control and Prevention (CDC) staff. In the system, a suspected measles case is defined as any person with fever and a generalized (characteristic) maculopapular rash (ie, nonvesicular), and any of following: coryza (running nose), cough, or conjunctivitis (red eyes). After the collection of the information on each suspected measles case, the information ultimately is entered into the system (Figure 1).
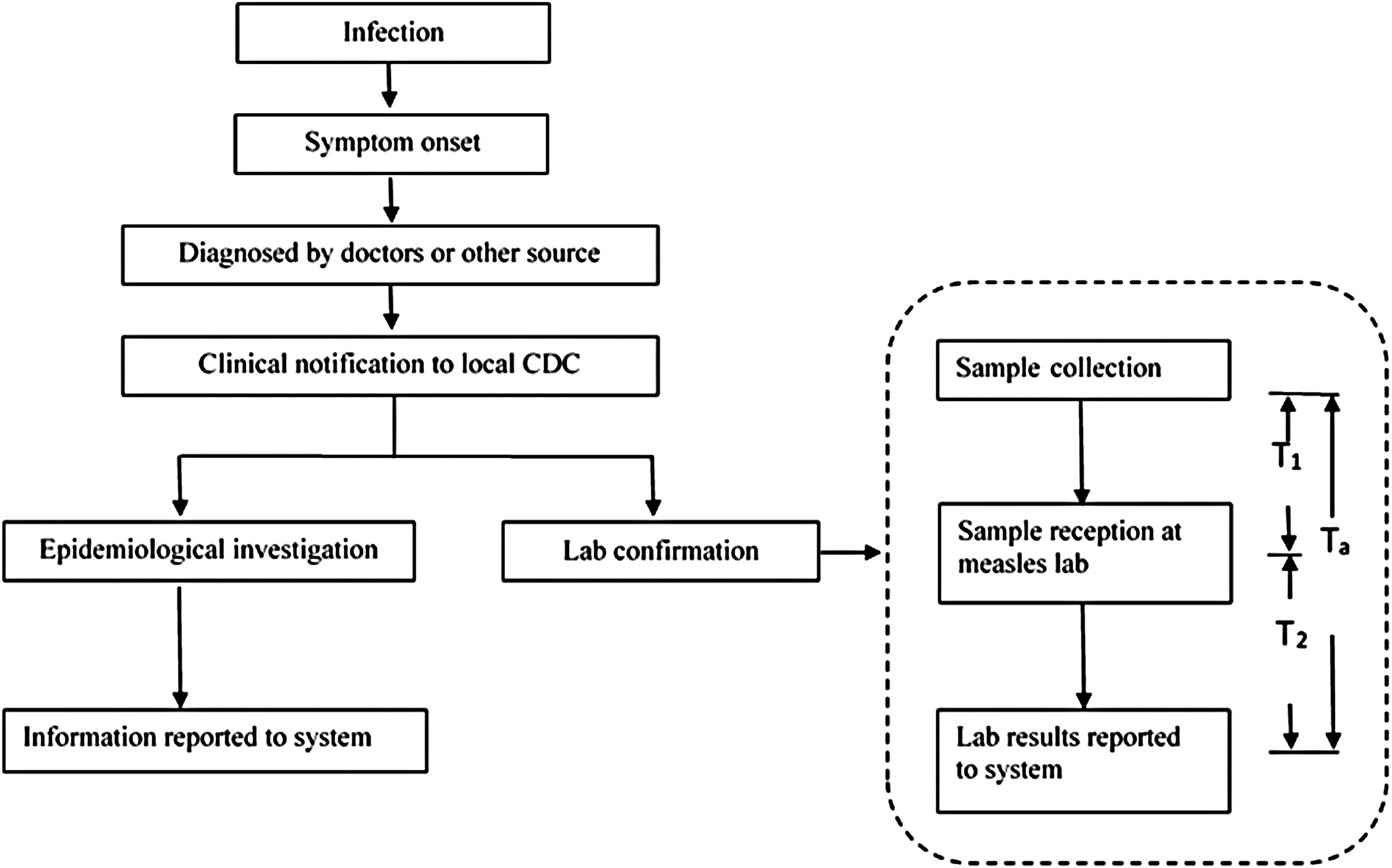
Reporting Chains for Measles Surveillance in China. Transport duration (T1) was defined as time lag from the time when serum was collected to the time when serum was sent to lab and received. Analysis duration (T2) was defined as time lag from the time when serum was received to the time when the result was reported to the surveillance system. Total reporting duration (Ta) was defined as the time from serum collection to laboratory result reporting.
However, the goal was not achieved despite the efforts made by China in the measles elimination program. 3 In line with the elimination goal, the measles surveillance system should be evaluated periodically. Timeliness is one of the key surveillance system metrics, because it can reflect the delay between any number of reporting steps in the measles surveillance process. Evaluating the timeliness of the measles surveillance system is crucial to improving efficiency in implementing the control measures.4,5
Previous measles timeliness studies have been conducted in various countries.2,6-9 All these studies showed the distribution of reporting delays, but few of them explored the influencing factors. Identifying factors would allow for targeted efforts to reduce delays. Moreover, other infectious diseases can appear with a rash resembling measles. Therefore, measles surveillance systems will be required to facilitate the laboratory confirmation of all suspected cases. 5 This study aims to evaluate the timeliness of measles laboratory reporting in China and identify factors associated with the reporting delays.
Methods
Sources of Measles Surveillance Information
We analyzed data regarding suspected measles cases reported to the measles surveillance system from 2009 to 2015 at Zhejiang Provincial CDC, China. All the information relating to each suspected measles case was extracted from the system, including its reporting department, reporting county, reporting date, date of serum collection, date of serum reception at lab, and date of laboratory result (first validated result). Laboratory tests in this study are IgM anti-measles antibody tests.
Reporting Durations and Reporting Delays
We intended to analyze the timeliness of measles laboratory reporting by measuring 3 time durations (Figure 1). Transport duration (T1) was defined as the time interval from when serum was collected to the time the serum was sent to the lab and received. Analysis duration (T2) was defined as the time interval from when the serum was received to the time when the result was reported to the surveillance system. Total reporting duration (Ta) was defined as the time from serum collection to laboratory result reporting. According to WHO-recommended standards for surveillance of measles, 10 Ta should be no more than 7 days. At least 80% of Ta should be within 7 days (≤7 days), and the total reporting delay was defined as a delay >7 days from serum collection to laboratory result reporting.
Sources of Potential Influencing Factors
According to a published study 1 and the available information in the surveillance system, reporting department and reporting season were thought to be 2 potential factors contributing to delays. The information of reporting department and reporting date were extracted directly from the surveillance system, after which the reporting dates were further divided into 4 seasons, based on traditional classification methods.
Moreover, previous studies showed that economic level had been used as a stratified factor to evaluate the notifiable infectious disease surveillance system. 11 Using 5 economic indicators (per capita GDP, per capita total investment in fixed assets, urban and rural residents' savings balance at the end of the year, finance gross income, and proportion of tertiary industry in GDP), 90 reporting counties in Zhejiang were categorized into 3 levels (levels I, II, and III) in an official economic report. Counties with higher levels have lower economic status. In an unpublished study, CDC staffs in economic level III were different from those in economic level I in terms of age and education level. Therefore, economic level was hypothesized to be a potential influencing factor.
Statistical Analysis
The median was calculated for each interval. Total reporting duration (Ta) was categorized into 2 groups, depending on whether or not the duration was within 7 days. Differences in the distribution of factors between the 2 groups were estimated by using Pearson chi-square test. Moreover, comparison was made between the median durations of T1 and T2 using Wilcoxon signed rand test. Using a chi-square trend test, the trend of proportions of cases notified within the time limit was statistically analyzed for the period of 7 years. For the comparison of time durations (T1, T2, and Ta) over the 7 years, nonparametric Kruskal-Wallis test was performed, followed by Bonferroni-Dunn multiple comparison test.
Associations between Ta and factors were accessed using a logistic regression model, including the following variables: reporting department, local economic level, and season.
All statistical tests were 2-sided, and P-values less than 0.05 were considered statistically significant. Statistical analysis was conducted with the SAS statistical software, version 9.2 (SAS Institute, Cary, NC, USA).
Results
Timeliness of Measles Laboratory Reporting
A total of 19,659 suspected measles cases were reported to the surveillance system from 2009 to 2015. The annual numbers of cases were: 2009 = 2,928; 2010 = 2,406; 2011 = 3,436; 2012 = 2,340; 2013 = 3,135; 2014 = 2,540; 2015 = 2,874. Among them, 18,518 were experimentally confirmed.
Medians of laboratory reporting durations are shown in Table 1. Medians of T1 in 7 years were all less than 1 day. T2 was longer than T1 (P < 0.001), and its median decreased from 3 in 2009 to 1 in 2015. For Ta, median decreased from 5 in 2009 to 2 in 2015.
Median time delays (days) between the time points of surveillance, 2009-2015
Figure 2 showed the cumulative duration distribution for 3 durations. For both T2 and Ta, the curve for duration in 2009 was always below those in other years, thus indicating that the duration in 2009 was longer than in other years. According to Bonferroni-Dunn multiple comparison, a decreasing trend was found from 2009 to 2012, which proved a tendency toward shorter durations. Nevertheless, no obvious difference was observed between durations in 2012 to 2015, neither in length nor in trend.

Cumulative Distribution for T1, T2 and Ta. For both T2 and Ta, the curve for duration in 2009 was always below those in other years, thus indicating that the duration in 2009 was longer than that in other years. According to Bonferroni-Dunn multiple comparison, a decreasing trend was found from 2009 to 2012, which proved a tendency toward shorter durations. However, no variation was observed for T1.
As for WHO-recommended standards for surveillance of measles, 1,870 laboratory reports exceeded 7 days, and the median of total reporting delays was 13 days. In addition, 89.82% of laboratory reports were received within 7 days (Table 2). The number of cases notified within the time limit for all years (excluding 2009) were above 80%. Also, an increasing trend was found, which confirmed the tendency toward more efficient laboratory reporting.
Proportion (%) notified within the WHO-recommended time limit
P for χ2 test.
P for χ2 test for trend.
Associations Between Factors and Total Reporting Delays
Associations between factors and Ta are presented in Table 3. Odds ratios (ORs) and 95% confidence intervals (CIs) were evaluated. Cases within time limits differed from the cases exceeding the time limit in terms of the reporting department (P < 0.001), local economic level (P < 0.001), and season (P < 0.001). CDC had a shorter delay than hospitals (OR = 0.184, 95% CI: 0.101-0.337). The OR for counties with level III relative to level I was 1.740 (95% CI: 1.566-1.933). Moreover, reporting in summer and winter both were associated with longer laboratory reporting delays (summer: OR = 1.229, 95% CI: 1.089-1.388; winter: OR = 2.157, 95% CI: 1.883-2.471).
Association of factors with Ta
P for χ2 test.
P for logistic regression.
Discussion
To evaluate whether the measles surveillance system could support timely notification, we assessed the timeliness of measles laboratory reporting in Zhejiang, China. Key intervals in the laboratory reporting chain were identified, followed by the calculation of associated durations.
To the best of our knowledge, published studies describing timeliness of measles surveillance systems generally do not explicitly describe the timeliness of laboratory reporting.6,7 Moreover, the measles surveillance system process in China might be different from that in other countries. Therefore, an international comparison of timeliness for measles laboratory reporting between China and other countries remains difficult.
The web-based measles surveillance system was not perfect at the beginning. 12 In this study, durations in 2009 were identified as the longest and the proportions of cases notified within the time limit was the lowest. These results are consistent with the facts. Furthermore, there was a decreasing trend in durations for both T2 and Ta. An increasing trend for proportions of cases notified within the time limit could be observed, indicating that great efforts have been made to improve the timeliness of reporting (ie, more technical training and management training, stricter assessment of laboratory operation). 13
Based on the results, T2 was longer than T1. Shorter T1 can be attributed to a highly motivated group of healthcare workers in hospitals and convenient transport from remote locations. However, reasons for longer T2 include the laboratories waiting to accumulate a group of specimens before testing and apathy among certain technical staffs.
In order to improve timeliness, some factors associated with delayed reporting were identified. According to the measles surveillance system, the majority of suspected cases are reported by hospitals. Blood samples were collected at the first contact with cases by hospitals, after which they were sent to the local CDC. Subsequently, the sera were separated and delivered to the appropriate laboratory for testing. There are also a small number of cases reported by CDC either in active search or in epidemiologic investigation. Blood samples of these cases were collected directly by CDC and sent to the laboratory afterward. Therefore, there is no doubt that cases reported by CDC had a shorter delay than those reported by hospitals.
In addition, economic level was one of the influencing factors. Our results showed Ta was attributed to T2. Therefore, the economic level was mainly affected Ta by influencing T2. There were 2 potential reasons for longer T2 in areas with economic level III. First, awareness of cost saving in areas with economic level III is more likely to be stronger than in areas with level I. For staff in areas with economic level III, more time was required to accumulate as many samples as possible for a single test. Second, as noted in our unpublished study mentioned above, the specialized skills of staff in areas with economic level III might not be as good as those in economic level I. As a result, more time might be required for sample analysis.
As for the season, studies have documented that yearly measles outbreaks usually occurred in spring, usually from March to May, in China. 14 Naturally, more attention is paid to measles surveillance during spring. Samples are tested as quickly as possible for outbreak detection. As a result, a shorter laboratory delay is found in spring.
According to factors associated with delays discussed above, corresponding feasible ways should be identified to improve timeliness. Government investment into measles laboratories in level III counties should be increased. For example, more investments should be made in measles laboratory construction (ie, to build new laboratories, to buy and maintain the equipment). Otherwise, a high-quality experimental technical team should be assembled to meet the management requirement in level III counties (ie, more professional skills training, more investment in attracting talent). Furthermore, efforts to investigate new cost-effective methods for sampling (ie, oral fluid samples) and testing (ie, dried whole blood spots for detecting measles virus by PCR) should also be emphasized.15,16
Several limitations should be noted in our study. In this study, the factors available for assessing associations are based on the measles surveillance system. However, the number of these available factors is limited. There are other factors that might have contributed to laboratory reporting delays (eg, computer system down-time for upgrades, maintenance, or new application development; data validation or error checking). 17 Moreover, due to the small sample size of cases detected by virus isolation and the lack of relative WHO-recommended standards, timeliness of virus isolation and genetic characterization was not evaluated, so further studies on more complete timeliness evaluation in measles surveillance systems are warranted.
In summary, research results provide the preliminary evidence that timeliness of measles laboratory reporting increased annually, and we identified factors associated with reporting delays. In further studies, other factors that might contribute to laboratory reporting delays need to be identified, and the timeliness of other steps in the measles reporting chain should be assessed.
Footnotes
Acknowledgments
The authors declare that they have no conflict of interests. Timeliness data were collected from the measles surveillance system. The patients' information contained in the records was removed before analysis. Therefore, no informed consent was required, and there were no ethical issues relevant to the study. Our work was funded by the Natural Science Foundation of Hangzhou Medical College, grant number: 2016XZA05.