
Abstract
Pope Francis visited Philadelphia for 2 days during September 2015. Preparedness functions managed by the Philadelphia Department of Public Health (PDPH) were similar to those of other mass gatherings but also required accommodation of special security arrangements and the location of public events in central areas of the city. Public health planning involved collaborations with multiple city, state, and federal agencies and neighboring jurisdictions. PDPH preparations encompassed incident command procedures, contingency planning, disease surveillance and prevention, food safety, vector control, BioWatch air sampling, volunteer management for first-aid services, and continuity of operations. These were based on, or informed by, existing emergency plans and prior experiences in responding to public health crises, supporting large public events, managing regional preparedness exercises, engaging Medical Reserve Corps volunteers, and executing routine functions. Although the papal visit concluded without the occurrence of a substantial public health or healthcare emergency, lessons learned have and will continue to improve coordination with partner agencies in planning and executing large-scale events, as well as managing regional disease surveillance procedures and medical volunteer engagement. Another area identified for improvement concerns enhancing the role of local health departments in planning for responses to possible BioWatch alerts.
Pope Francis visited Philadelphia in September 2015. Preparedness functions managed by the Philadelphia Department of Public Health were similar to those of other mass gatherings but also required accommodation of special security arrangements and the location of public events in central areas of the city. Public health preparations encompassed incident command procedures, contingency planning, disease surveillance and prevention, food safety, vector control, BioWatch air sampling, volunteer management for first-aid services, and continuity of operations.
O
Background and Context
The Philadelphia Office of Emergency Management managed and coordinated the engagement of Philadelphia city agencies and served as the focal point for the city's interactions with other event partners, including local and state governments across a metropolitan area spanning 4 states (Pennsylvania, Delaware, New Jersey, Maryland), federal agencies, and nonprofit and private-sector organizations. Overall planning and role delegation followed principles articulated by the National Incident Management System 7 and federally defined Emergency Support Functions, 8 under a “unified command” led by a core group of senior decision makers from the city of Philadelphia, the US Secret Service, the Federal Bureau of Investigation (FBI), and the World Meeting of Families—an entity affiliated with the Catholic Church and the official event host. 6 Aspects of the papal visit that affected planning in general and public health preparedness in particular included security arrangements, the anticipated number and characteristics of attendees, and maintenance of the continuity of public services beyond those focused on the World Meeting of Families.
Security Arrangements
The US Department of Homeland Security (DHS) declared the pope's visit a National Special Security Event (NSSE)—a designation for events of national or international importance where there is a potential for terrorism or criminal activity. 5 Under this declaration, the US Secret Service had lead responsibility for planning and security, the FBI for intelligence and crisis management, and the Federal Emergency Management Agency (FEMA) for consequence management. 6 Although protection of the pope and public safety were shared concerns across all levels of government, federal agencies were primarily concerned with the former and state and local agencies with the latter.
Public events in central Philadelphia were contained within a carefully controlled security perimeter that included city hall and other city government buildings, including the location of the health commissioner's office and other PDPH services (eg, finance, human resources, and information technology) and several PDPH program offices. Other sites within this perimeter included hotels, restaurants, other businesses, office buildings, tourist destinations, apartment and condominium buildings, and other residences, embracing approximately 6 square miles on Saturday and a smaller area on Sunday (Figure 1). To establish and protect the secure area, authorities closed streets, 2 central Philadelphia rail transit stations, and sections of interstate highways, including the primary bridge across the Delaware River between Philadelphia and Camden, New Jersey, beginning on Thursday or Friday preceding the pope's arrival in Philadelphia through the following Monday. 9 Beyond the secure perimeter, a larger area surrounding the central district was closed to incoming vehicle traffic from Thursday evening through Monday morning, except for limited access times to allow for essential and event services (Figure 1). No hospitals were located within the secure perimeter, but several hospitals and long-term care facilities were located within the zone that was closed to incoming traffic, as were office locations for additional PDPH divisions, including those responsible for infectious diseases, public health preparedness, environmental health, the medical examiner's office, and administration of the department's network of primary care clinics.
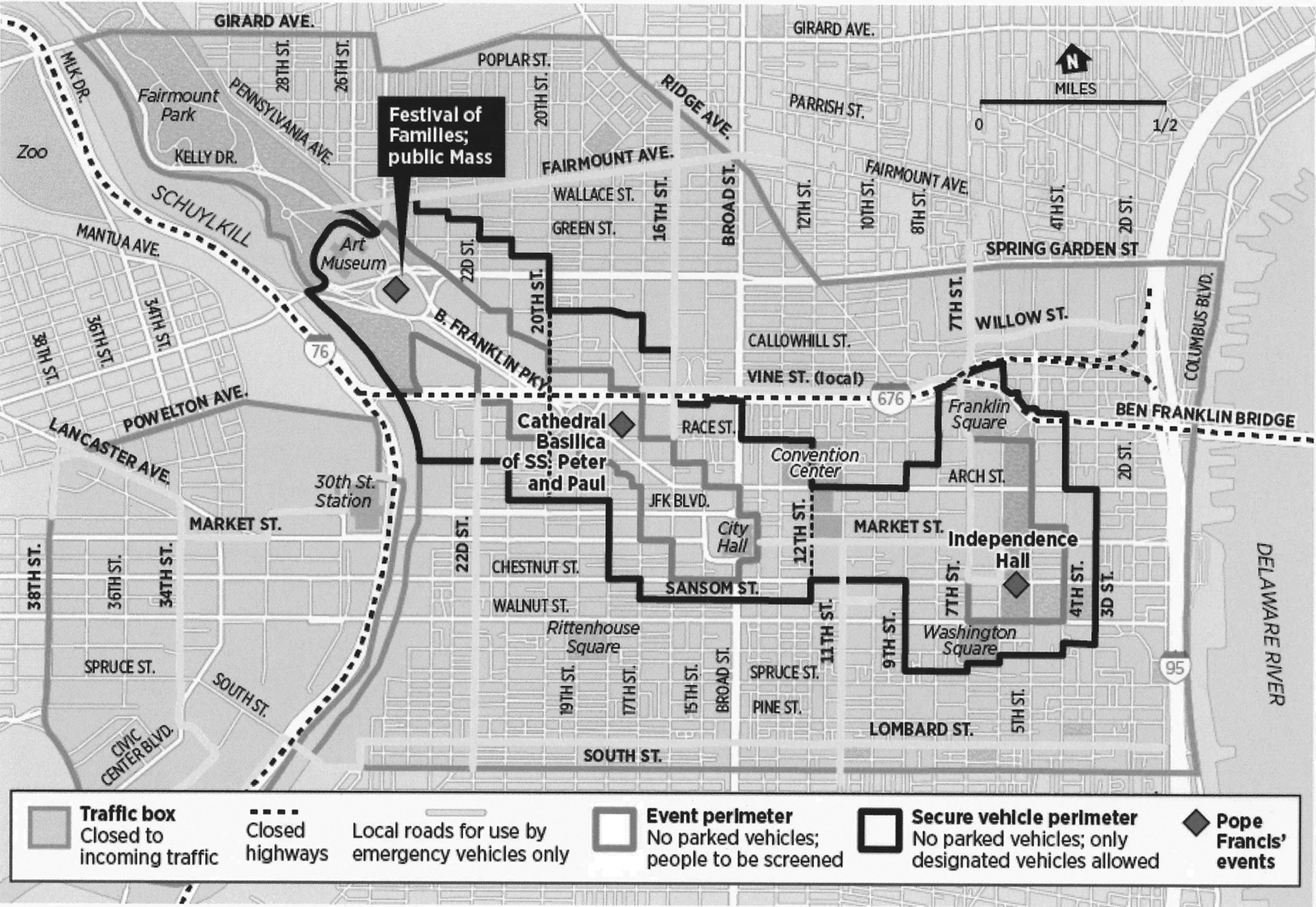
Secure vehicle and event perimeters for papal visit, central Philadelphia, September 2015. Public events included a speech at Independence Hall followed by a parade to the Festival of Families event near the art museum (Saturday) and a parade from city hall to a mass near the art museum (Sunday). Reproduced with permission from the Philadelphia Inquirer.
Crowd Estimates and Characteristics
Event planning was predicated on an initial estimate that 2 million or more people might attend the weekend events. As a global event, visitors were expected from multiple countries, with attendant concerns regarding possible disease importation. The 2014-15 Ebola crisis was waning but persistent, and public health tracking of travelers from affected West African countries was ongoing. 10 Because alcoholic beverages would not be sold at event venues and because the World Meeting of Families was a religious and spiritual gathering, lower risks of unruly crowd behaviors and accompanying alcohol-related health problems were expected compared to other public events held on the Benjamin Franklin Parkway, such as the annual 4th of July celebration. A temporary campground was planned to be located in a nearby city park, requiring consideration of public health needs for food, water, and sanitation, but this plan was cancelled a few weeks before the event due to a lack of interest as manifest by low numbers of required advance reservations, one of several indications that event attendance might be lower than initial estimates.
Continuity of Operations
Although the papal visit occurred over a weekend, roadway closures, traffic restrictions, and disruptions in transit service, along with closure of city buildings in the secure perimeter, spanned Thursday to Monday, affecting PDPH staff and clients. The PDPH sexually transmitted diseases and tuberculosis clinics were outside the secure perimeter but within the zone where vehicular entry was prohibited, and routine Friday and Monday services were cancelled or shifted to more distant primary care clinics operated by PDPH. Schools operated by the Catholic Archdiocese of Philadelphia were closed for the entire week preceding the papal visit and the following Monday; public schools were closed from Wednesday through Monday; and many private schools also closed for all or part of this period, creating childcare demands for many PDPH employees.
Work schedule negotiations between the city of Philadelphia and the 2 unions representing its employees were not finalized until a few weeks before the event. These policies had to account for those employees whose workplace sites were closed or within the zone of prohibited vehicle entry, those who had a direct role in supporting event-related activities and would likely work overtime, those whose routine responsibilities included after-hours or weekend duty, and those who worked at locations removed from the event areas where services remained open but where routine means of transportation to and from work might have been disrupted.
Planning and Preparations
Under the overall coordination of the city's Office of Emergency Management, responsibilities for local ESF8 public health and medical functions were divided among PDPH, a fellow city department responsible for behavioral and mental health services, the Philadelphia Fire Department's Emergency Medical Services (EMS) unit, and the Hospital and Healthcare Association of Pennsylvania (HAP) (Table 1). In brief, EMS had lead responsibility for planning and providing first-aid and ambulance services, and HAP for supporting the continuity of operations at nearby hospitals and hospitals' preparations for mass casualties. EMS based its plans for first-aid services on initial attendance estimates. Consideration was given to reducing the number of first-aid tents amid indications that attendance might be lower than initially projected, but, because of uncertainties surrounding attendance predictions, EMS did not scale back those plans. Although EMS had the lead for first-aid services, PDPH was responsible for engaging Medical Reserve Corps volunteers to staff first-aid stations. Within the committee structure organized under the unified command, public health functions were part of an overarching health committee led jointly by EMS and the Secret Service.
Roles of the Philadelphia Department of Public Health and other state and local agencies in addressing functions under the Federal Emergency Support Function #8 (ESF8), Public Health and Medical Services, World Meeting of Families Papal Visit, September 2015
For PDPH, event planning touched multiple programs across the health department, including those with a core role (eg, emergency preparedness, outbreak prevention/response and disease surveillance, food safety, sanitation, vector control, and BioWatch 11 air sample collection), those with a potential role (eg, the public health laboratory in the event of an infectious disease outbreak, the medical examiner's office in the event of a mass casualty event), those with a supportive role (eg, information technology, facilities and vehicle services, human resources, finance), and those whose routine operations might be affected even though their locations were outside areas affected by traffic controls (eg, primary care clinics, air pollution monitoring, the Philadelphia Nursing Home). Event planning was centralized in the health commissioner's office and managed by the Public Health Preparedness Program, a unit that normally operates in the division dedicated to infectious disease prevention.
Beginning approximately 6 months before the event, the health commissioner convened and the preparedness program director managed an executive planning committee, which coordinated the development and execution of a department-wide response plan. This involved leads from divisions responsible for core event functions. Initially this group met monthly, then bi-weekly and weekly as the event neared. Representatives from other divisions were involved on an ad hoc basis, summaries of executive committee meetings were shared with all division directors, and preparations were discussed at routine monthly meetings with all division leads. In addition to ongoing staff interactions with the Pennsylvania Department of Health, beginning approximately 2 months before the event, executive committee meetings concluded with a brief call with lead representatives from the state health department. These conversations focused on engagement of Medical Reserve Corps volunteers statewide and the state's role in engaging federal partners in the event of the detection of a potential pathogen from a BioWatch air sample 11 or the need to request emergency mass prophylaxis resources from the Strategic National Stockpile. 12
The development of the PDPH event plan drew from its existing emergency preparedness documents, including protocols for incident command, outbreak response, mass dispensing, mass fatality response, and continuity of operations, that had been developed using guidance and state funding from the Centers for Disease Control and Prevention's (CDC) Public Health Emergency Preparedness program. 13 These protocols and attendant staff capacities had been honed by experience from prior nationwide infectious disease emergencies and local crises, including a demolition-related building collapse that killed 6 people in 2013 14 and an Amtrak train crash that killed 8 people earlier in 2015. 15 In both of the these events, the PDPH medical examiner's office was involved in victim identification, family notification, and cause-of-death determinations. In addition, PDPH had served as a coordinator and convener for annual regional preparedness exercises during 2009 to 2011 and a full-scale regional preparedness exercise involving a plague scenario in fall 2014. PDPH's department-wide papal visit public health response plan was submitted to the city's office of emergency management and became an annex to the city-wide World Meeting of Families Health and Medical Operations Plan. PDPH preparations were also informed by its experience in addressing annual mass events, such as 4th of July celebrations and Labor Day concerts that are convened on the Benjamin Franklin Parkway—a site of papal events on both visit days.
Incident Command and Event Management
The organization of PDPH's internal incident command structure reflected NIMS guidance with modifications reflecting the department's event functions (Figure 2). Two weeks prior to the pope's arrival, PDPH convened leadership from across the department and representatives from the state health department to review key elements of the PDPH incident command structure and event plan, including personnel assignments and communications procedures, and to conduct a tabletop exercise that invoked the PDPH incident command procedures. The exercise considered 3 scenarios: a power disruption affecting internet connectivity, disease surveillance, and communications; a stampede with approximately 150 fatalities that invoked mass fatality responses; and a common-source foodborne infectious disease outbreak with clinical manifestations that largely appeared after visitors began to return home to destinations across the country and the globe. Although the major lesson learned was to reaffirm the value of such exercises in building team capacity, the exercise also informed minor changes or clarifications to internal PDPH communication procedures.

Philadelphia Department of Public Health incident command organizational chart for the World Meeting of Families Papal Visit, September 2015
PDPH assigned 2 senior staff to serve as its incident commanders—a deputy commissioner for public health programs and the director of the emergency preparedness program—both of whom had been closely involved throughout event preparations (including co-author SA). These individuals were embedded in the Office of Emergency Management's citywide emergency operations center (EOC) during its 4-day activation and worked alternating 12-hour shifts coincident with the EOC's overall staffing rhythm. Their location in the citywide EOC facilitated communications with incident managers from other agencies, particularly those involved in supporting medical field operations and volunteer support services. In addition, 2 PDPH media/communications staff participated either in person or remotely in a separate federal joint information center.
PDPH convened a public health emergency coordination center (PHECC) at the usual office location of the preparedness program, a few blocks from the secure area. This office was staffed during each 12-hour shift by approximately 10 people working in teams to support communications among PDPH event participants, medical field operations (support to first-aid stations), disease surveillance, BioWatch air sampling, and food safety inspections (Figure 2). These staff interfaced with the PDPH incident commander at the citywide EOC and coordinated departmental communications and local and regional information sharing.
No substantial public health threats emerged during the event. Problems managed by the public health response teams and PDPH incident commanders were mainly limited to logistic complications that affected multiple agencies, not just public health, such as the timely delivery of meals for volunteers and last-minute but quickly resolved problems regarding access to secure areas for credentialed staff and vehicles.
In addition to the summary of roles in addressing ESF8 functions in Table 1, additional consideration will be given to selected functions.
ESF8: Public Health and Medical Information
For the first time, local and state public health departments in the 4-state metropolitan region standardized the content and synchronized the timing of successive health advisories related to a large-scale event, which PDPH coordinated via its role as chair of the Philadelphia-Camden-Wilmington Metropolitan Statistical Area Public Health Workgroup. This included health information for visitors 16 and alerts to area hospitals and the medical community regarding symptoms and evaluation of patients with infectious diseases that might be carried by travelers from anticipated countries of origin and information about diseases that might arise from intentional acts of biological, chemical, or nuclear terrorism, based on information resources from the CDC. In advance of the event, PDPH provided updates to local hospitals regarding procedures for event-related disease surveillance, prevention, and potential response procedures through regular contacts with hospital preparedness coordinators and through engagements with state hospital association representatives who were co-participants in event-related health planning committees.
ESF8: Health Surveillance
Public health surveillance during the event represented a mix of special and enhanced routine surveillance capacities. MRC volunteers stationed in first-aid stations documented and recorded nonidentifying data regarding patient encounters using smartphone technology. These data were uploaded via wifi service that had been enhanced for this event to a data system jointly managed by the state's hospital association, the city's EMS, and the city's Office of Emergency Management, which shared the data with PDPH for disease surveillance purposes. In addition, PDPH established a paper-based encounter tracking system for the first-aid stations, including plans for collection by bicycle messenger, as a back-up in the event of a technology failure, which was not invoked.
PDPH used its existing syndromic surveillance system, derived from a state-wide system managed by the Pennsylvania Department of Health, for monitoring patient visits to most of the city's hospital emergency departments. This system monitors a spectrum of disease syndromes based on patients' “chief complaints” or discharge diagnoses, including syndromes designed to capture infectious respiratory and gastrointestinal illness.
PDPH served as the lead for collating and summarizing disease surveillance information from health departments in nearby counties in 4 states, building on the existing planning forum and coordination practices of the Philadelphia-Camden-Wilmington Metropolitan Statistical Area Public Health Workgroup. PDPH collaborated with surveillance partners in these areas to identify data sources, expand and modify existing systems, develop a web-based reporting mechanism for local and state jurisdictions, analyze and interpret findings, and compile a regional public health surveillance report that was disseminated widely to incident managers at 12-hour intervals, providing a regional snapshot of disease activity. This report was disseminated daily for 4 days in advance of the pope's arrival in Philadelphia and then twice daily for the 2 days of the papal visit and the following day. The report included data updates and a brief synthesis of findings from syndromic surveillance, case reports of unusual disease occurrences, findings from surveillance activities in neighboring counties, and information culled from social media regarding potential disease-related events. PDPH surveillance leads reviewed incoming reports to determine what information to include or clarify before including in surveillance reports. For example, during the event a neighboring health department reported a case of botulism, which, upon follow-up, had been determined to be naturally occurring and not related to potential bioterrorism, an essential fact given the distribution of the surveillance report not only to public health agencies but also to law enforcement agencies and DHS.
Syndromic surveillance based on data from emergency department visits for hospitals within or nearby the event sites demonstrated fewer visits than expected based on historical precedents despite the influx of visitors, and there were no concerning spikes in visits for specific syndromes. These declines in total emergency department visits were slightly offset by modest increases in visits to hospitals at a greater distance from the event, but total ED visits area-wide remained lower than usual. This probably reflected a combination of multiple factors: Some residents of center-city neighborhoods left Philadelphia to avoid the crowds; street closures and travel constraints might have deterred the use of ED care for noncritical illnesses; travelers are likely to be relatively healthy; the weather was mild, minimizing the risk of heat-related illness; alcohol was not sold or allowed into the secure event perimeters; and attendance at the event was largely motivated by its religious and family-oriented themes, which minimized unruly behaviors that can precipitate injuries.
Similarly, tracking of visits to first-aid stations, as well as regular checks with MRC staff in the stations, did not detect any substantial public health problems among event attendees. Nearly all visits were for relatively minor first-aid needs. Some problems were observed in the use of the automated visit tracking system, and occasional discrepancies were noted regarding numbers of visits between data entered into the automated visit tracking system and paper-based logs maintained at some sites, particularly in the few instances when transport to a nearby hospital was warranted.
PDPH monitors Philadelphia air quality through programs supported by the federal Environmental Protection Agency and the state of Pennsylvania's Department of Environmental Protection. In addition, it is responsible for routine daily sample collection and transport for BioWatch, the multi-city DHS program that monitors air for the presence of microbiologic agents that might be used in a bioterrorist attack. 11 PDPH assisted DHS in deploying extra BioWatch samplers inside the secure perimeter. These samplers were serviced by federal authorities during the event, while PDPH maintained responsibility for specimen collection from existing BioWatch air monitoring locations and for transporting those specimens to the state health department's public health laboratory, approximately 25 miles from Philadelphia. Special security procedures also led to a diminution of the PDPH role with respect to usual BioWatch engagements with state and federal agencies in planning for the initial assessment and response procedures in the event of a possible positive test. No BioWatch alerts came to the attention of PDPH during the event.
ESF8: Medical Care Personnel
PDPH was responsible for coordinating the involvement of Medical Reserve Corps 17 volunteers from Philadelphia and, in collaboration with the Pennsylvania Department of Health, throughout Pennsylvania to staff medical first-aid stations. Coincidentally, the papal visit followed the completion of a 3-year effort led by PDPH to develop the Pennsylvania Intrastate MRC Volunteer Deployment Plan, which was finalized in May 2015 and tested in June 2015. The demand for volunteers to support medical field operations during the visit provided an opportunity to activate the plan, mobilize volunteers from across the state, and put key elements of the plan into practice. This included coordination of multiple MRC units, transportation from multiple rally points, and activation of a volunteer reception center where volunteers registered and received training.
MRC volunteers staffed 9 of 10 first-aid stations located throughout the event site, including 1 station that was located in the waiting area of the PDPH STD clinic. PDPH provided and delivered first-aid supplies to these stations prior to their activation, which required special planning given road closures. For 8 of the stations where MRC volunteers were deployed, the volunteers worked under the supervision of EMS, which had lead responsibility for first-aid services at these sites. A ninth first-aid station where MRC volunteers were positioned was managed by staff from the Pennsylvania Department of Health and the US Department of Health and Human Services (HHS). A tenth station, which offered a higher level of medical care services and was located adjacent to the stage used for evening events on Saturday and Sunday, was operated and equipped by HAP in coordination with local hospitals and did not involve MRC volunteers. The city's Office of Emergency Management was responsible for feeding and sheltering event volunteers, including the MRC volunteers. Volunteer credentialing was managed by the Secret Service. PDPH also collaborated with EMS to assure appropriate disposal of medical waste from all 10 sites.
As planned by EMS, this 10-site operation involved a 3-day, 24-hour operation. This was predicated on the initial assumption that the event could draw up to 2 million visitors and, based on consultations with colleagues in other cities that have hosted large events, that an estimated 60,000 persons might seek medical services, potentially stressing the city's hospital emergency departments. Because event attendance was low relative to planning assumptions, several sites saw little patient traffic, due to their location beyond crowd concentrations or proximity to other sites, and few patients were seen during the overnight hours. Altogether, 169 Medical Reserve Corps volunteers from across the state were engaged for a 60-hour deployment period. Although this number was substantially lower than expected based on pre-event MRC surveys and volunteer commitments, it was sufficient to meet the demand for services. 18
Coordination of first-aid services during the event was complicated by the involvement of individuals from multiple agencies (city, state, and federal), including people with decision-making authority who had not been substantially engaged in planning these services. It quickly became apparent that the scope of practice of volunteers and others staffing first-aid tent stations was not sufficiently defined, and personnel from several agencies were operating in medical field sites with varying levels of expertise and experience and conflicting instructions and expectations. 18 While these problems did not result in any adverse consequences for those who sought first-aid services, they were identified as areas for improvement.
ESF8: Food Safety
Food services inside the event perimeter were provided at 9 sites by a primary food service contractor and by 40 independent vendors who operated mobile food trucks. Because security procedures limited vendors to 1 early-morning entry and 1 evening exit per day, PDPH imposed restrictions on the scope of menus, reflecting the nature of foods that could be safely managed and served under these entry and exit constraints. On-site inspections of vendors as they entered the secure perimeter to establish operations required special staff credentialing and coordination with the FBI to assure PDPH vehicle access, as well as collaboration with the city's garbage disposal service to assure safe and environmentally appropriate disposal of food if vendors failed to meet food safety requirements. PDPH sanitarians required the disposal of approximately 500 pounds of food, primarily because of failures to pass food safety inspections upon vendors' entry into secure areas. Otherwise, the food safety situation was uneventful.
ESF8: Vector Control
Control of disease vectors focused on mosquitoes and rats in areas routinely frequented by visitors and used as the sites of papal events. Access to sewers for mosquito larvicide applications and rodent baiting was constrained, however, because manhole covers were welded shut as a security provision 6 to 8 weeks in advance of the event, requiring adjustments of vector control schedules.
Conclusions
The papal visit occurred without the emergence of any substantial public health concerns, and, as a result, the PDPH capacity to respond to a major public health crisis in the context of a mass gathering was not tested by this event.
Key lessons learned arose from the PDPH experience in 2 areas concerning interactions with other response partners. First, regarding the deployment of MRC volunteers at the first-aid stations, which were primarily managed by another agency, opportunities were identified and addressed in the PDPH after-action assessment to improve multi-agency coordination, clarify authorities for volunteer supervision and medical decision making, and scale the deployment of first-aid services as attendance estimates are modified. These insights informed and improved MRC engagement in first-aid services during the Democratic National Convention in July 2016. 18 Second, regarding BioWatch air monitoring, given the engagement of supplemental testing technology, PDPH was not sufficiently engaged in pre-event planning with state and federal partners regarding the response to a potentially positive or positive BioWatch test result. Had a BioWatch alert occurred based on sampling from one of the supplemental collection sites, the ability of PDPH to contribute effectively to decisions regarding response options would have been diminished or delayed without greater awareness of the implications of test results based on the supplemental technology. This occurred despite the obvious role of PDPH in responding to a major threat to public health in Philadelphia and in apparent disregard of a 2011 recommendation from the Institute of Medicine that the BioWatch system “needs better collaboration with public health systems to improve its usefulness.” 19 That potential role would include participation in assessing the public health implications of a positive finding in the BioWatch system and, if needed, implementation of any public health response.
Public health surveillance efforts, beyond those routinely managed by PDPH, included data collection from first-aid stations using hand-held device technology and the collation and summation of surveillance reports from neighboring counties. Although both functioned reasonably well and neither was challenged by a crisis, opportunities for improvement were observed. For the former, this included a need for better training of MRC volunteers in the use of hand-held devices for data collection. For the latter, needs for PDPH to follow-back to other counties for clarifications or additional information would be reduced if initial reports included more contextual information, such as insights from any preliminary queries that might have been made into the potential source or cause of disease. This is important because the audience for surveillance reports, which become part of regular situation reports issued over the course of events, includes not only public health officials but also public safety officials who are primed to respond quickly to potential acts of bioterrorism. For example, knowledge regarding the likely source of exposure for a disease cluster or an individual case of a rare disease, if possible, is critical.
The papal visit created unique planning and operational challenges for PDPH that warranted a collaborative, cross-divisional approach to develop and execute a comprehensive department-wide response plan. For any large health department, which contains a mix of categorical and cross-cutting functions, a common organizational question concerns when and whether cross-cutting functions should be located at the director level or embedded within a division. In PDPH, the emergency preparedness function is part of the infectious disease control division, reflecting historical and federal funding connections among preparedness, bioterrorism, and pandemic influenza planning and the experience of that division in responding to infectious disease crises. Given the breadth of involvement and the potential impact of this event on different parts of the health department, elevating the planning function for this event to the health commissioner's office enhanced the ability of the preparedness team to engage people from throughout the department.
This point may be meaningful for other local health departments in planning for large special events, as organizational structures vary greatly across jurisdictions, including the placement of preparedness programs in health departments and their corresponding authority to direct department-wide planning initiatives. Decisions regarding whether that step is taken in future events in Philadelphia will likely depend on the scope and potential impact of those events, as well as the preference of future commissioners regarding organizational strategies.
Public health functions in anticipation of and during the papal visit, a brief but intensive event, were similar to those in larger-scale and longer situations. In their comprehensive report following the 2004 Olympic Games in Athens, Tsouros and Efstathiou outlined the domains of public health responsibility: assurance of healthcare capacity and readiness for mass casualties, disease surveillance and outbreak response, environmental health, food safety, public information, and preparedness for the health consequences of potential terrorist acts. 4 Each of these domains was part of the response of PDPH to this event, which included coordination with multiple neighboring local and state health departments and was just one part of a much larger multi-agency effort.
PDPH's capacity to prepare for this event was based on experience with prior crises and on capacities developed through investments in public health emergency preparedness following the events of 2001, largely due to federal funding and guidance, most notably from CDC and to a lesser extent from the DHS. Core aspects of preparing for the papal visit also represented extensions or special adaptations of routine public health functions, such as food safety, disease surveillance, and vector control, demonstrating that a key predictor of public health capacity to prepare for a crisis is to manage routine functions successfully.
Footnotes
Acknowledgments
The authors wish to acknowledge Palak Raval-Nelson, PhD, Director of the Division of Environmental Health, who contributed to the sections on food services, sanitation, and vector control and who directed these activities, and Edward Braun, Interim Director (former) and Program Manager (current) of the Division of Air Management, who contributed to the section on BioWatch air sampling and who directed these activities. Others from the Philadelphia Department of Public Health who played key leadership roles in the activities described in this article include Carolyn Johnson, MD, Deputy Commissioner, (former) Director of the Division of Disease Control, and public health incident co-commander; Jane Baker, Chief of Staff; José Lojo, MPH, Division of Disease Control, Surveillance Manager. During the period covered by events described in this report, the lead author (JWB) served as Health Commissioner for the city of Philadelphia.