
Abstract
Improving preparedness in the European region requires a clear understanding of what European Union (EU) member states should be able to do, whether acting internally or in cooperation with each other or the EU and other multilateral organizations. We have developed a preparedness logic model that specifies the aims and objectives of public health preparedness, as well as the response capabilities and preparedness capacities needed to achieve them. The capabilities, which describe the ability to effectively use capacities to identify, characterize, and respond to emergencies, are organized into 5 categories. The first 3 categories—(1) assessment; (2) policy development, adaptation, and implementation; and (3) prevention and treatment services in the health sector—represent what the public health system must accomplish to respond effectively. The fourth and fifth categories represent a series of interrelated functions needed to ensure that the system fulfills its assessment, policy development, and prevention and treatment roles: (4) coordination and communication regards information sharing within the public health system, incident management, and leadership, and (5) emergency risk communication focuses on communication with the public. This model provides a framework for identifying what to measure in capacity inventories, exercises, critical incident analyses, and other approaches to assessing public health emergency preparedness, not how to measure them. Focusing on a common set of capacities and capabilities to measure allows for comparisons both over time and between member states, which can enhance learning and sharing results and help identify both strengths and areas for improvement of public health emergency preparedness in the EU.
Improving preparedness in Europe requires a clear understanding of what EU member states should be able to do, whether acting internally or in cooperation with each other. The authors developed a preparedness logic model that specifies the aims and objectives of public health preparedness, as well as the response capabilities and preparedness capacities needed to achieve them.
E
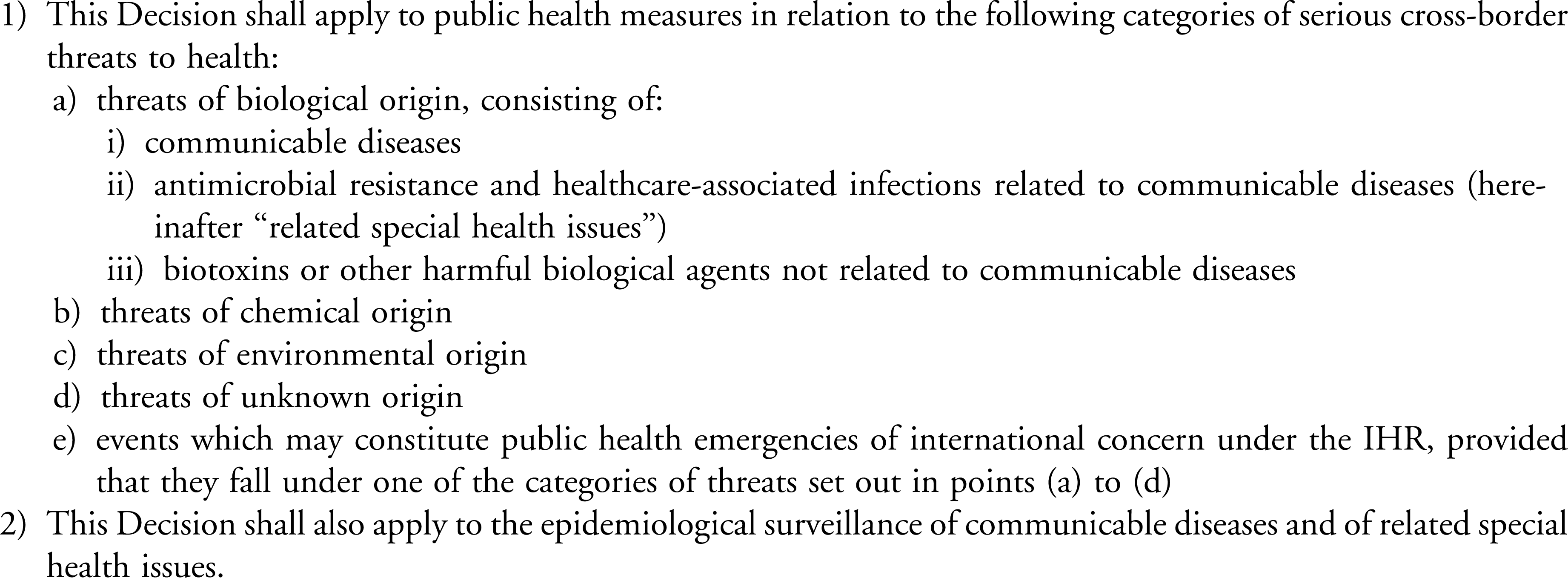
Scope of Decision No. 1082/2013/EU
Assessing—and improving—preparedness requires that member states possess a clear understanding of what actions they are able to take in response to a threat, whether acting internally, in cooperation with each other, or with EU and other multilateral organizations. However, measuring the basic components of preparedness is difficult, as serious public health emergencies are relatively infrequent and possess many aspects specific to their respective contexts, leaving few opportunities to assess outcomes by direct observation in critical incident reviews. 2 Therefore, public health system researchers sometimes develop a logic model to address these challenges, identifying the factors that, based on scientific evidence and practitioner experience, contribute to positive outcomes. 3 A preparedness logic model should specify the aims and objectives of public health preparedness, as well as the response capabilities and preparedness capacities needed to achieve them. Analyzing the response to actual incidents can strengthen the evidence base supporting a logic model. However, even without a strong evidence base, logic models can be an effective method for identifying provisional measures based on current knowledge.
In order to enable EU member states to identify preparedness gaps and to assist the European Centre for Disease Prevention and Control (ECDC) in developing a set of competency-based training programs, we adapted a preparedness logic model, originally created to capture elements of the US preparedness enterprise,4,5 using 4 approaches.
First, we examined the results of a literature review of 6 cross-border emergencies that occurred in Europe to understand differences in capabilities in the European context. 6 The events were: biological hazards (an outbreak of E. coli in 2011 and pandemic influenza H1N1 in 2009 and 2010), chemical hazards (a sludge reservoir breach in 2010 in Hungary threatening the Danube River and melamine contamination of milk in 2008 in products imported from China), and hazards of environmental origin (a heat wave affecting several European countries in 2003 and a volcanic ash cloud originating in Iceland in 2010).
Second, we reviewed reports of peer review visits on the European response to Ebola in 2014 conducted by the ECDC in 3 EU member states. (Examples from the review of these incidents are mentioned below to illustrate the meaning of the capabilities, but due to space limitations, not all of the examples we used are listed.)
Third, we reviewed existing competency statements developed by ECDC for public health epidemiologists, 7 microbiologists, 8 and healthcare infection control experts. 9 We also consulted the scientific literature about public health emergency preparedness and guidance.10,11
Finally, we invited participants at the 2015 annual meeting of the ECDC National Focal Points for Preparedness and Response to identify which capabilities were implemented during the responses to the recent Ebola and Middle Eastern respiratory syndrome (MERS) outbreaks.
The following section provides a series of definitions that anchored the development of the logic model, particularly in distinguishing between capabilities and capacities. We describe the method used for identifying both the critical capabilities and capacities in the European context.
Defining Preparedness
Our logic model is grounded in the definition of public health emergency preparedness developed by Nelson and colleagues:
… the capability of the public health and health care systems, communities, and individuals, to prevent, protect against, quickly respond to, and recover from health emergencies, particularly those whose scale, timing, or unpredictability threatens to overwhelm routine capabilities. Preparedness involves a coordinated and continuous process of planning and implementation that relies on measuring performance and taking corrective action. 12
This definition's core concept is the “public health emergency preparedness system,” a complex network of individuals and organizations that play critical roles in creating the conditions for health. The Institute of Medicine (IOM) represents this system with the government public health infrastructure at the core and the healthcare delivery system, civil protection agencies, employers and businesses, the media, academia, and other public and private community organizations as important components. 13 While these actors operate as separate entities, a robust public health emergency preparedness system requires that all components work together when necessary.
Our logic model incorporates a fundamental distinction between capacities (eg, infrastructure, trained personnel, policies and procedures) and capabilities, or the ability to use these capacities to effectively identify, characterize, and respond to emergencies. For example, having strong laboratories and skilled microbiologists may be insufficient if they cannot be mobilized in a timely manner, or if laboratory results cannot be shared with and acted on by decision makers. Capacities and capabilities are both important for an effective emergency response; however, depending on the context, different kinds of capacities are needed to achieve the required capabilities. The logic model focuses measurement efforts largely on capabilities, allowing different EU member states to determine how to best achieve them in their own context. For instance, member states with widespread integrated national electronic medical record systems might rely on them for syndromic surveillance to detect disease outbreaks, but countries or regions with less well-developed systems might rely on more traditional surveillance methods.
Capacities represent the means that a country uses to achieve its preparedness capabilities but necessarily reflect variations in member states' government and private-sector organizations. In some member states, for instance, surveillance is conducted at the national level, whereas in others surveillance and other public health activities are conducted at the local level. Some countries have a national, government-run healthcare delivery system, whereas others have a regional system with significant private-sector involvement. Consequently, it is difficult to specify capacities in a way that applies to all EU member states. Capabilities, on the other hand, describe what member states are expected to achieve during an emergency and can be described in a consistent way for all countries. For this reason, this analysis focuses on capabilities rather than capacities.
The capabilities and capacities in this logic model represent a theoretical framework for identifying the key dimensions of preparedness member states need to assess. Capacity inventories, exercises, critical incident analyses, and other approaches are all useful methods for conducting the assessments, but they are beyond the scope of this article.5,14
ECDC Logic Model
Below we describe the logic model (Figure 2) that emerged from the process described above, beginning with descriptions of the capacities and capabilities included in the model. The capabilities are described in more detail in Figure 3. Consistent with Decision 1082, the logic model focuses on “cross-border threats to health.” However, most of the capacities and capabilities are also important for responding to public health emergencies that are entirely confined to member states.

Logic Model for Public Health Preparedness in EU Member States

Proposed ECDC Public Health Preparedness Capabilities
Capacities
The public health emergency preparedness logic model begins with Potter and colleagues' grouping of public health emergency preparedness capacities into legal, economic, and operational domains. 15 Our research suggests the importance of adding “social capital,” which describes the partnerships and informal relationships between individuals and organizations critical to effective emergency operations and community resilience.16,17 The Toolkit for Assessing Health System Capacity for crisis management, 10 created by WHO Europe, the WHO's Joint External Evaluation Tool, 11 and the WHO's Strategic Framework For Emergency Preparedness 18 also describe important public health emergency preparedness capacities.
Capabilities
Given the number of capabilities in the logic model, it is helpful to organize them into high-level categories. The first 3 categories—(1) assessment; (2) policy development, adaptation, and implementation; and (3) health services—represent what the public health system must accomplish to respond effectively. The fourth and fifth categories represent a series of interrelated functions needed to ensure that the system fulfills its assessment, policy development, and prevention and treatment roles: (4) coordination and communication concerns information sharing within the public health system, incident management, and leadership, and (5) emergency risk communication focuses on communication with the public.
Evaluation and training are critical components of the preparedness cycle but are not “response capabilities” per se. We recognize that conducting post-incident reviews, and sometimes research, in a timely manner is of critical importance for system learning. This can require performing these analyses or collecting appropriate data during or shortly after an event. Similarly, an effective response can include just-in-time training and exercises. However, these activities are more properly categorized as capacity development, rather than response capabilities, despite their timing.
The case examples cited in the following discussion are intended to illustrate the concepts and demonstrate the importance of these capabilities for cross-border threats to health. They also document the process we used to develop the capabilities described above.
As a whole, assessment capabilities enable member states' preparedness systems to recognize and characterize a threat, monitor its impact on the population, and evaluate the efficacy of interventions to contain the threat. Assessment depends on having laboratory and surveillance capacities, including appropriate legal arrangements, in place before an event. Information derived from assessment activities must be communicated to all segments of the public health preparedness system and the public in order to support policy development and implementation, prevention, and treatment efforts.
The group of policy development, adaptation, and implementation capabilities reflect member states' ability to adapt existing authorities and policies to the new and emerging circumstances of a cross-border threat to health, and to enforce both existing and new laws and regulations needed to implement these policies. Adaptation and implementation must be timely and flexible, reflecting developing information about the threat. These capabilities are focused on the national level, although it is recognized that a lack of consistency within member states, or among bordering member states, can erode public confidence. All of these activities require communication and coordination across a variety of actors working at the global, European, national, and subnational levels, and these supporting capabilities are described below. The capabilities in this section apply to the development and implementation of substantive policies, regulations, and official guidance regarding infection control and disease treatment in clinical settings and for population-based disease control activities.
This group of capabilities addresses prevention and treatment services delivered to individuals by the member states' health sector. This includes provision of vaccines and other countermeasures to the general public and to healthcare workers, as well as physical and mental health care for those affected by mass-casualty and long-running incidents. The medical countermeasures, supplies, and equipment needed to provide these services are considered capacities, but procuring additional supplies, managing the stockpile, and distributing them during a crisis are critical capabilities and thus are included in this section. The most effective and efficient means for delivering healthcare services to individuals—whether preventive or therapeutic—will depend on the nature of the threat and the way in which the public and private sector is organized, as the organization of the health sector varies markedly among member states. Thus, these capabilities focus on what must be accomplished during an event, rather than on how to accomplish it. The WHO Regional Office for Europe's toolkit for assessing health system capacity for crisis management 10 provides more detail on how to assess and improve member states' preparedness in this regard.
This group of capabilities comprises efforts to communicate within the public health emergency preparedness system to coordinate and manage a complex system's response to a cross-border threat. The first 3 groups of capabilities describe what must be accomplished during a crisis; the capabilities are not ends in themselves, but rather describe how member states achieve these ends. Effective leadership and governance structures are important for crisis management, but because these factors vary across member states, here the focus lies on key aspects of coordination and communication needed during an emergency. Similarly, it is recognized that existing regulations and resource constraints may limit the amount of coordination, but these and other factors that explain why a member state was not able to coordinate their efforts are appropriate topics for a critical incident analysis.
The focus of this group of capabilities is the real-time exchange of information, advice, and opinions between experts or officials and people who face a threat (hazard) to their survival, health, or economic or social well-being. The ultimate purpose of this group of capabilities is to ensure everyone at risk is able to make informed decisions for mitigating the effects of the threat (hazard) and to take protective and preventive action.
Discussion
The ECDC logic model presented in this article, with its associated capabilities and capacities, represents a theoretical framework for identifying what to measure in capacity inventories, exercises, critical incident analyses, and other approaches to assessing public health emergency preparedness, not how to measure them. Focusing on a common set of capacities and capabilities for measurement allows for comparisons both over time and between member states, which is important for enhancing learning and sharing results across all approaches and, ultimately, for identifying both strengths and areas for improvement in public health emergency preparedness in the EU. The capabilities in the logic model can be useful for structuring a critical incident analysis that covers all relevant dimensions of preparedness.
This article represents the first step in ECDC's plans to eventually develop and deliver competency-based training programs to assist member states in fulfilling their responsibilities under Decision 1082. As training budgets, time, and personnel backfill resources are all limited, public health officials need an efficient and highly practical educational approach that effectively addresses core readiness competencies. However, competencies are characteristics of individuals who work in the public health emergency preparedness system, whereas capacities and capabilities are system-level characteristics. To bridge this gap, our subsequent work will review the strengths and weaknesses of approaches for assessing countries' capabilities and capacities, as specified in the ECDC logic model, such as drills, simulation exercises, and critical incident analyses. We will then develop detailed competencies and related knowledge, skills, and abilities for specific staff roles and capabilities. In this way, EU member states will be able to identify training needs and ECDC can deliver training where it is most needed.
Footnotes
Acknowledgments
This research was supported by a contract with the European Centre for Disease Prevention and Control (ECDC) as part of its efforts under Decision No. 1082/2013/EU to identify both the strengths and the areas for improvement of public health emergency preparedness in the EU member states. The authors are grateful to Carmen Varela Santos, Judit Takacs, and others from the ECDC staff who facilitated this research and commented on earlier drafts of this paper, and to participants in the December 2014 meeting of the ECDC Preparedness Focal Points, who commented on an earlier draft of the logic model.