
Abstract
The 2014-2016 Ebola outbreak in West Africa prompted a select group of US hospitals to establish high-level isolation units equipped with advanced engineering controls, trained staff, and stringent protocols to safely treat highly infectious disease patients. This survey details the comprehensive infection control protocols developed by these units, including for decontamination of units, post-mortem management, liquid waste disposal, and personal protective equipment (PPE) use. In spring 2016, a survey was electronically distributed to the 56 original Centers for Disease Control and Prevention (CDC)–designated high-level isolation units. Responses were collected via a fillable PDF and analyzed using descriptive statistics. Thirty-six (64%) high-level isolation units responded; 33 completed the survey, and 3 reported they no longer maintained high-level isolation unit capabilities. Nearly all responding units had written procedures for decontamination, liquid waste disposal, and PPE use; however, infection control protocols varied between units. High-level isolation units implemented multiple strategies in promoting hand hygiene among staff and in monitoring correct PPE use. Maximum time allowed in full PPE was restricted in all but 2 units (average of 3.45 hours per shift). Almost all (94%) had written procedures for the management of human remains, although only 2 units had written protocols for an autopsy of a patient with a highly infectious disease. While the vast majority of high-level isolation units reported having written protocols for infection control practices, staff compliance and procedural application are the true indicators of the state of preparedness. Therefore, rigorous training and staff adherence to infection control practices is critical to minimizing exposure risks.
In spring 2016, a survey was electronically distributed to 56 original CDC-designated high-level isolation units. The survey detailed the comprehensive infection control protocols developed by these units, including for decontamination of units, post-mortem management, liquid waste disposal, and personal protective equipment (PPE) use.
D
In late 2014, the CDC announced a new system of categorization of US hospitals' differing abilities to care for patients with EVD or other diseases requiring high-level isolation, classifying hospitals as frontline hospitals, Ebola assessment hospitals, or Ebola treatment centers. 1 In this new system, 56 hospitals across the United States were designated as Ebola treatment centers and were deemed capable of providing the highest level of isolation care to patients with highly infectious diseases. In addition, 1 Ebola treatment center in each of the 10 US Department of Health and Human Services (HHS) regions was subsequently designated as a regional Ebola and other special pathogen treatment center (RESPTC) and given funding for additional enhancement to their physical units, labs, training, and other activities. 3
Although the CDC did provide guidance on the specific augmented operational and infection control capabilities they believe form the foundation for creation of high-level isolation units in the 56 Ebola treatment centers, each facility had to work with its existing physical plant, infrastructure, budget, and safety culture to establish its high-level isolation unit. Therefore, although previous consensus reports from both European and US infectious disease experts have identified numerous recommended elements in the design and construction of high-level isolation units,4,5 hospitals generally labored to develop their high-level isolation capabilities with consistent adherence to these recommendations, and notable differences have been previously reported in the choices each hospital has made in developing its unit.6-8
It is noteworthy that similar isolation units have existed in Europe for more than a decade, with greater agreement among them on the specific details regarding operational commonalities such units should share. European infectious disease experts have defined high-level isolation units as clinical units specifically designed for highly infectious disease care, equipped with enhanced engineering controls and stringent infection control protocols to minimize the potential for disease transmission to healthcare workers, hospital personnel, and the public; they have detailed recommendations and specifications for these units. 4
The newly developed network of high-level isolation units in the United States has been operational for more than 2 years, but little detail is currently available about the comprehensive protocols developed by US high-level isolation units to protect the safety of their healthcare workers and patients. This article details routine and terminal decontamination procedures of high-level isolation units and medical devices, postmortem management, liquid waste disposal, and PPE selection and protocols of US high-level isolation units.
Methods
In spring 2016, a survey (with institutional review board exemption University of Nebraska Medical Center IRB #172-16X) was electronically distributed to all 56 original CDC-designated high-level isolation units, including the 10 regional Ebola and other special pathogen treatment centers. The survey was developed referencing robust checklists used by the European Network for Highly Infectious Diseases (EuroNHID) in a 2009 evaluation of European high-level isolation units 9 and consisted of 70 questions of varying types: open-ended qualitative questions; discrete, multiple-choice questions, some with the option to provide qualitative information for “other”; and multiple-choice questions allowing for multiple selections. Most questions had additional subquestions that were dependent on the response.
The survey was distributed electronically via email as a fillable Adobe PDF and organized into thematic sections. Sections of the survey, which were further divided into 3 to 4 subsections, were: personnel management, management of PPE, infection control procedures and promotion, laboratory capabilities, and operational capabilities. We discuss the results of the data related to PPE management and infection control here; other results will be detailed in later publications. If the high-level isolation unit had completed the 2015 pilot survey inventorying unit capabilities and listed a point of contact, the follow-up survey was delivered to the provided email address. For all other high-level isolation units, the survey was sent to personnel with publicly accessible email addresses. The survey was completed by site representatives and collected via Adobe Pro. Nonrespondents were emailed with follow-up requests 2 weeks after the initial return deadline. Responses were coded and analyzed using descriptive statistics in an electronic spreadsheet (Microsoft Excel).
Results
Thirty-six (64%) high-level isolation units responded: 33 completed the survey, and 3 responded by stating their facility was no longer maintaining high-level isolation unit capabilities.
Infection Control
Thirty-two (97%) high-level isolation units reported their strategies to promote hand hygiene and procedures established to monitor staff adherence to correct hand hygiene practices (Table 1). High-level isolation units implemented a variety of strategies for hand hygiene promotion, with the majority using posters (n = 27, 84%), hand hygiene campaigns (n = 26, 81%), on-site exercises (n = 20, 63%), and videos (n = 17, 53%).
Infection Control Protocols and Procedures for US High-Level Isolation Units
For each high-level isolation unit, more than 1 selection was allowed.
29/32 high-level isolation units described their procedures.
Six high-level isolation units plan on either solidifying and/or treating with disinfectant and flushing down toilet.
Written protocols for routine hygiene (ie, daily cleaning) of the high-level isolation units were available in all 32 facilities that responded to the decontamination section of the survey and were available in 31 (97%) for final decontamination of both the unit and medical devices (Table 2). Twenty-seven (87%) of the 31 high-level isolation units with final decontamination procedures designated staff to observe the final decontamination to provide quality assurance of the process. Figure 1 displays infection control tasks performed in the high-level isolation units and designated responsible staff members.
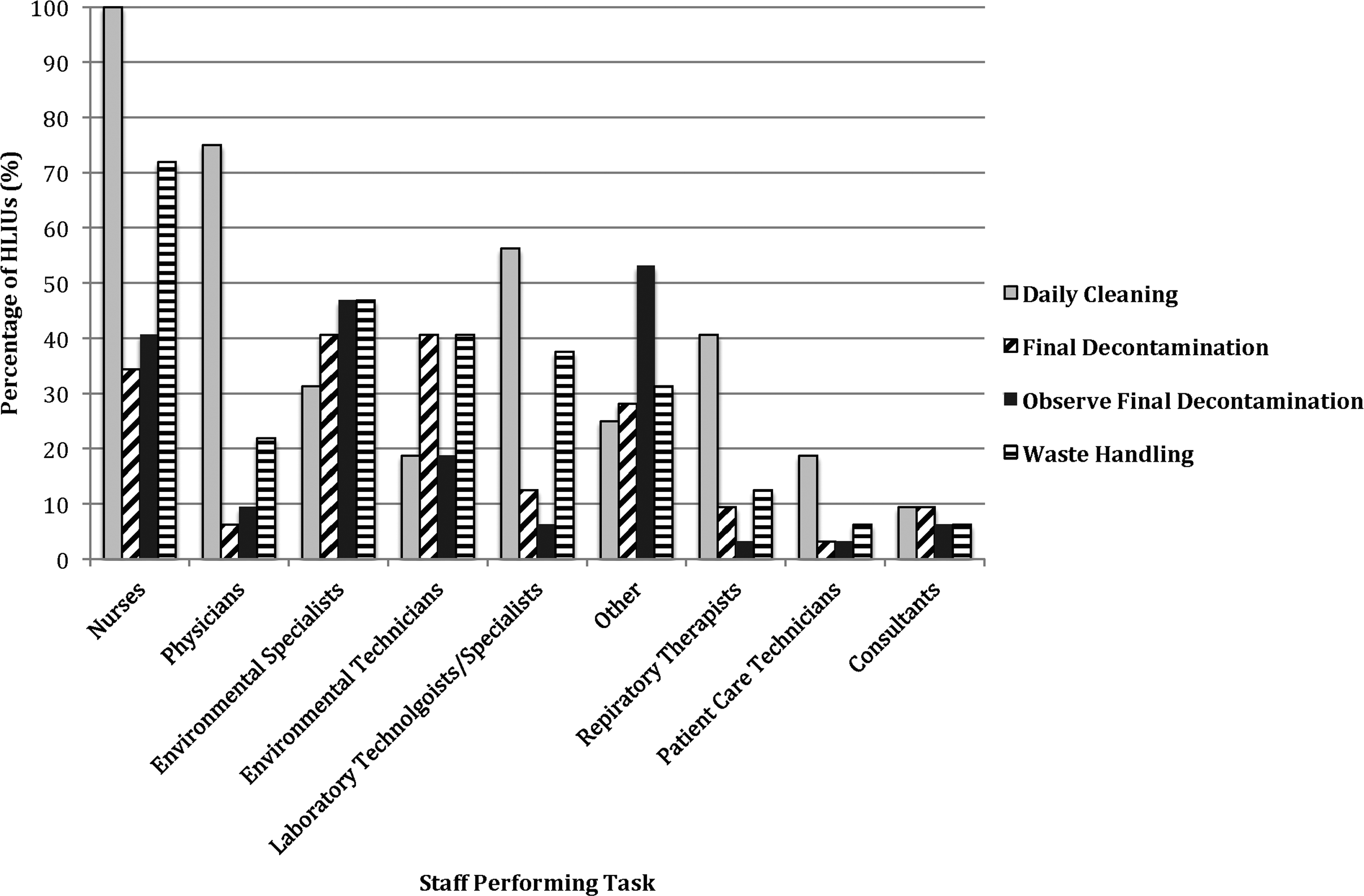
Infection control tasks performed by various staff in responding US high-level isolation units
Decontamination Procedures for US High-Level Isolation Units
For each high-level isolation unit, more than 1 selection was allowed.
All but 3 (91%) high-level isolation units do not intend to transport the patient outside of the isolation unit at any point of care (eg, operating room, MRI, x-rays). Two reported that patient movement would be performed after case-by-case evaluation, while the other high-level isolation unit would transport a patient to an operating room or for CT or MRI imaging. All 3 reported having final decontamination procedures for the areas to where the patient with a highly infectious disease would be transported.
In all, 32 high-level isolation units responded to questions on post-mortem management. Thirty of the 32 (94%) had procedures to manage human remains of a patient with a highly infectious disease, and 2 units (6%) had specific procedures to perform an autopsy (Table 1). In the area provided for additional information, 5 high-level isolation units reported no autopsies would be performed, while another stated that whether or not an autopsy would be offered would be contingent on the specific highly infectious disease. Plans for disposal of liquid waste (eg urine, vomit, feces) are presented in Table 1. Average reported disinfection contact time for the 25 (76%) units that planned to treat liquid waste with a disinfectant prior to disposal was 11.5 minutes (range 3-30 minutes).
PPE Use
Twenty-three (70%) high-level isolation units had protocols or procedures for the selection of differing kinds of PPE ensembles, depending on the specific patient acuity and also on the types of procedures to be performed during patient care (ie, routine care vs aerosol-generating procedures, such as sputum induction). Of the 10 units without variable PPE selection procedures, 9 (90%) plan to use complete suits, including powered air-purifying respirators (PAPRs), at all times during patient care. High-level isolation unit strategies for monitoring correct use of PPE and ensuring adequate PPE supplies, including procedures for PPE decontamination for re-use, are detailed in Table 3. Nearly all (n = 31, 94%) units reported protocols restricting maximum time allowed in full PPE, with a mean shift of 3.45 hours (median = 4.0; range 1.5 to 4.0).
Results of Personal Protective Equipment Use, Decontamination, and Selection for Responding US High-Level Isolation Units
For each high-level isolation unit, more than 1 selection was allowed.
Almost all (n = 32, 97%) high-level isolation units reported having procedures to ensure adequate quantities of PPE if there were a sudden demand. Of these, 31 (97%) used internal stockpiling and 23 (72%) were supplied from an external structure or institution. Thirty-one (94%) high-level isolation units had protocols for monitoring stockpiled PPE for expiration dates.
Discussion
Prior to the establishment of a national network of high-level isolation units, most regions in the United States lacked access to hospitals with the enhanced isolation capabilities, advanced staff training, and extensive infection control protocols necessary for safe and effective highly infectious disease care. High-level isolation units have developed policies, procedures, and operational measures to mitigate infection control challenges posed by highly infectious diseases and have used engineering controls to maximize healthcare worker safety. Results indicate that most high-level isolation units have specified procedures for infection control processes (eg, decontamination, liquid waste management, hand hygiene practices) and PPE management, but approaches vary. This may reflect the lack of formalized guidance and science-based evidence in these areas, in tandem with the rapid, unprecedented establishment of such units in the United States. Consensus recommendations, however, have been developed by the EuroNHID following their 2009 survey of European high-level isolation units and include guidance on PPE and infection control practices for high-level isolation units.10-12
The emergence of EVD, MERS, and novel influenza viruses pose occupational risks to healthcare workers treating patients with these diseases and to the public. As the final barrier, strict vigilance on proper PPE use is critical to preventing disease transmission to healthcare workers; yet, previous studies show poor compliance with donning and doffing behaviors can lead to self-contamination.13,14 Every surveyed high-level isolation unit reported implementing multiple strategies for monitoring correct PPE use, with all units using trained observers and donning and doffing partners. Fewer units reported having full-body mirrors and posted checklists with written instructions on donning and doffing orders (61% and 88%, respectively). While there is not one accepted “correct” sequence for donning and doffing PPE, doing so in a sequence that avoids exposure is critical. Checklists serve as a guide for trained observers and donning/doffing partners to confirm completion of each step recommended by the individual facility, while mirrors can be used for real-time self-assessment and ensuring the healthcare worker avoids touching the skin while doffing PPE. 15 Employing these strategies and requiring staff to frequently demonstrate competence in donning and doffing practice can minimize self-contamination during doffing.
Equally important to PPE behaviors is the selection of appropriate PPE for care of patients with highly infectious diseases. While securing the best possible protection, PPE should be comfortable and well tolerated by unit staff, as high-level isolation units reported staff spend an average of 3.45 hours per shift in full PPE, during which it can become cumbersome and warm. 16 Physical exhaustion and emotional fatigue due to extensive spells in PPE and intensive highly infectious disease care may further exasperation. Using a full PAPR suit, regardless of the highly infectious disease or the acuity of the patient, as 27% of high-level isolation units do, ensures a high level of protection and can provide temperature cooling for the healthcare workers by increasing airflow in the PPE. However, full suits may decrease healthcare workers' dexterity and hinder communication, given the excess motor blower noise that powers filtration in a PAPR. Tolerability and comfort of PPE should be assessed during competency demonstrations and through training and exercises. 16
The Environmental Protection Agency (EPA) has asserted that domestic wastewater treatment plants were designed to handle a multitude of microorganisms, including viruses, and the diseases present in waste systems. 17 EPA and CDC initially advised that liquid wastes from patients with highly infectious diseases could therefore be disposed of safely through normal means (toilets and drains).18,19 However, only 4 (12%) high-level isolation units reported they would flush waste without first treating it with disinfectant prior to disposal. A recent study showed that the Ebola virus could survive in sterilized wastewater for up to 8 days (albeit under laboratory conditions), which contributes to the decision and need to disinfect wastewater prior to discharge. 20 A subsequent study by the same group conducted a risk assessment that found the potential exists for the transmission of EVD to sewer workers through contaminated sewage. 21 Although no data exist specifically on the effectiveness of inactivating Ebola virus by treating liquid waste with disinfectant prior to discharge, it is likely the decision to disinfect wastewater eases public concern and provides assurance to municipal workers. Similarly, terminal decontamination best practices offered by the Nebraska Biocontainment Unit following EVD care include meticulous procedures that may go beyond requirements for Ebola virus inactivation but were completed, in part, to appease public concern. 22
Post-mortem handling of remains of patients with highly infectious disease is a known transmission route, 22 yet US high-level isolation units report insufficient levels of preparedness in this area. While nearly all reporting units have written procedures for managing human remains, a majority have not established a memorandum of understanding with a funeral home or crematorium, which may pose difficulties in disposing of human remains of patients with a highly infectious disease. Furthermore, just 6.3% have specific procedures for the safe performance of an autopsy, compared to nearly 60% in a 2009 survey of European high-level isolation units. 11 Both US and European consensus groups considered a lack of written and exercised safety protocols for performing an autopsy to be a high risk for workers, given the nature of the procedure and that autopsies may be necessary in patients with highly infectious diseases if a diagnosis has not been established.5,11
The majority of high-level isolation units surveyed have written protocols for the selection of PPE based on patient acuity and disease, monitoring and adherence to PPE use, liquid waste disposal, post-mortem management, unit decontamination, and hand hygiene promotion of unit staff. While written procedures are the foundation of high-level isolation unit operations and training programs, staff compliance and application of these procedures are the true indicators of the state of high-level isolation unit preparedness for a patient with a highly infectious disease. For example, healthcare workers have been shown to be inconsistent when performing hand hygiene and disinfection tasks. 23 Despite high-level isolation units reporting numerous hand hygiene promotion and monitoring strategies, staff that are noncompliant with written procedures increase exposure risks. Rigorous training of staff on hand hygiene, PPE use, decontamination, and other infection control protocols is therefore essential to healthcare worker safety, as is ensuring staff remain alert and vigilant in adhering to infection control practices in this high-risk environment.
This study had several limitations. Data were self-reported and were not validated by our group or by external sources. Furthermore, our study surveyed only the availability of procedures; as such, we are unable to report on the actual procedural application or staff compliance for those procedures. We also recognize that countless other US hospitals that were not captured in our study took measures to increase their facilities' capability to care for a patient with EVD. This survey and the initial survey were administered only to a list of hospitals released by the CDC in late 2014 and early 2015. 24 Lastly, the response rate decreased from the initial survey (85%) to this follow-up (64%). While the follow-up was more comprehensive and time-consuming to complete, the decreased response rate could reflect waning interest and current perceived importance of high-level isolation unit capabilities. As reflected in the decisions of 3 hospitals to no longer maintain their high-level isolation capabilities, US high-level isolation units face challenges in sustaining their preparedness for treating highly infectious diseases. Moreover, it is possible that the 64% of units that completed the survey may have more advanced capabilities and therefore are more willing to disclose their current state of preparedness than the more than one-third of units that did not complete the survey. As such, reported results may not be indicative of all high-level isolation units. It is also possible that the one-third of units that did not complete the survey are no longer maintaining their capabilities, which could negatively affect national readiness.
In conclusion, with little doubt that the future holds novel highly infectious disease threats, the combination of highly trained staff, technical equipment, infection control infrastructure, and updated procedures unique to high-level isolation units offer biocontainment facilities capable of handling the most dangerous pathogens. Despite the existence of advanced technical infrastructure, healthcare workers in high-level isolation units are frequently in close contact with patients with highly infectious diseases and must rely on correct PPE use, including removal processes, to reduce exposure. 5 Protocol recommendations for both infection control processes and PPE management were consistently revised throughout the EVD outbreak as new research and best practices were disseminated, and it can be expected that the same will occur with the next highly infectious disease outbreak. Having written, practiced protocols and procedures can facilitate adaptation of high-level isolation unit operations to diverse diseases and enhance overall domestic preparedness for highly infectious diseases.
Footnotes
Acknowledgments
The authors would like to thank Philip Smith, MD, former medical director for the Nebraska Biocontainment Unit, for his expertise and insight into the development of the survey. All authors report no conflicts of interest. There was no financial support.