
Abstract
Anthrax, caused by Bacillus anthracis, is considered a severe bioterrorism threat because of its high mortality rate. The Chicago Healthcare System Coalition for Preparedness and Response (CHSCPR) aims to pre-position antibiotic medical countermeasures (MCMs) at healthcare facilities in order to provide on-site anthrax post-exposure prophylaxis. Pharmacists proposed moving toward a new process that involved the development of a standardized calculation methodology for acquiring supply drugs. This was an interventional quality improvement project aimed at optimizing inventory, acquisition, and distribution of antibiotic MCMs for anthrax post-exposure prophylaxis at Chicago hospitals for hospital personnel, associated first responders, and their families. The primary goal of the project was to pre-position a sufficient quantity of pharmaceuticals to allow Chicago hospitals to function as closed points of dispensing (PODs) for 72 hours; a secondary goal was to provide a 96-hour supply of anthrax post-exposure prophylaxis. A total of 35 Chicago hospitals were invited to participate in this intervention study, and 30 hospitals agreed to participate. Based on our calculation tool, we initially identified 6 (20%) hospitals with adequate oral doxycycline and ciprofloxacin inventory to last 72 hours and 3 (10%) hospitals with inventory to last 96 hours as a closed POD for anthrax post-exposure prophylaxis. The necessary quantities of medication needed to establish 72 and 96 hours of anthrax post-exposure prophylaxis were calculated by the CHSCPR and negotiated with a drug wholesaler to obtain product with maximum shelf-life and discounted pricing. Acting as a group purchaser, the CHSCPR organized drop shipment of medication directly to facilities from a wholesaler. This systematically calculated, pre-deployed pharmaceutical cache enhanced availability of antibiotic MCMs for anthrax post-exposure prophylaxis in 30 Chicago hospitals, allowing them to function as closed PODs for 96 hours during an incident.
The Chicago Healthcare System Coalition for Preparedness and Response wanted to pre-position antibiotic medical countermeasures (MCMs) at healthcare facilities to provide on-site anthrax post-exposure prophylaxis. This project aimed at optimizing inventory, acquisition, and distribution of antibiotic MCMs for anthrax post-exposure prophylaxis at Chicago hospitals for hospital personnel, associated first responders, and their families. The primary goal was to pre-position a sufficient quantity of pharmaceuticals to allow Chicago hospitals to function as closed points of dispensing (PODs) for 72 hours.
T
Anthrax, caused by Bacillus anthracis, is considered a severe bioterrorism threat because it may cause infection through multiple routes, including contact with skin, ingestion, and inhalation; inhalation can carry a mortality rate in the range of 75% to 85% when antibiotic treatment is delayed more than 4.7 days or is untreated.2-6 Expert guidance on selection of antibiotic MCMs for anthrax has been published for adult, pediatric, pregnant, and postpartum patients, with recommendations given for doxycycline and ciprofloxacin as drugs of choice for post-exposure prophylaxis.7-9 While levofloxacin is approved by the Food and Drug Administration (FDA) for anthrax post-exposure prophylaxis, no safety data are available for use beyond 30 days. 7 Rapid access to antibiotics following an anthrax incident is considered the most effective strategy to prevent illness. 10
Pre-positioning MCMs promotes rapid access to antibiotics. An incident may go undetected for hours or even days, and waiting for confirmatory testing may further delay post-exposure prophylaxis. 11 Therefore, a working clinical diagnosis warrants the distribution of post-exposure prophylaxis and activation of points of dispensing (PODs). Pre-positioning cached antibiotic MCMs at hospitals allows prompt activation of closed PODs and timely post-exposure prophylaxis administration to hospital staff and their households. Immediate availability of post-exposure prophylaxis allows vital hospital operations to continue during a public health emergency and decreases the burden of public antibiotic distribution campaigns at open PODs. For these reasons, pre-positioning cached antibiotic MCMs, namely at healthcare facilities, has been a goal of the Chicago Healthcare System Coalition for Preparedness and Response (CHSCPR) and the Chicago Department of Public Health (CDPH).
Historically, Chicago hospitals determined their individual needs for cached antibiotic MCMs and submitted requests to the CHSCPR annually for replenishment of pharmaceuticals, but the process was inconsistent. For example, some Chicago hospitals did not participate in obtaining and storing cached antibiotic MCMs due to a lack of institutional resources. Furthermore, some participating hospitals purchased antibiotics that were not considered first-line for anthrax post-exposure prophylaxis according to expert guidance. In addition, national drug shortages increased the cost burden and led to inconsistent supplies of preferred antibiotics for anthrax post-exposure prophylaxis.
The CHSCPR was faced with optimizing how Chicago hospitals acquire and maintain cached antibiotic MCMs and determining necessary quantities of antibiotics. This prompted the CHSCPR to investigate pre-positioning pharmaceuticals in hospitals for anthrax post-exposure prophylaxis. This report describes how the CHSCPR enhanced availability of antibiotic MCMs for anthrax post-exposure prophylaxis for Chicago hospitals. Enhancements included the development of a standardized calculation methodology for inventory and acquisition as well as the centralization of purchased supply drugs to allow each facility to function as a closed POD.
Methods
This was an interventional quality improvement project aimed at optimizing inventory, acquisition, and distribution of antibiotic MCMs for anthrax post-exposure prophylaxis at Chicago hospitals. The initiative, under the CHSCPR, was led by the Responder Safety and Health Committee Pharmaceutical co-chairs and guided by the executive committee, with pharmacist representation from the Centers for Disease Control and Prevention (CDC). The initial intervention took place between July 2014 and June 2015, with further refinement between July 2015 and June 2016. CDPH provided funding for this through a cooperative agreement from HHS (ASPR HPP). The CHSCPR invited all acute care and specialty Chicago hospitals to participate.
The quality improvement project consisted of multiple steps between July 2014 and June 2015. First, the CHSCPR developed a calculation tool to account for the number of employees in each hospital and the average daily census of both adult and pediatric patients (Table 1). The tool includes a factor of 1.8 for coverage of employee households based on data from the US Census Bureau, the addition of 1 caregiver per pediatric in-patient, and a 20% surge calculation. 12 The calculation tool determines each healthcare facility's needed number of doses of doxycycline or ciprofloxacin for 24 hours for anthrax post-exposure prophylaxis. Second, hospitals received in-person classroom education, with webinar capability for those unable to attend in person, about appropriate medications for anthrax post-exposure prophylaxis. Hospitals were made aware of the developed calculation tool and plans for the CHSCPR to execute a centrally purchased supply of oral doxycycline and ciprofloxacin for all participating institutions. Third, the CHSCPR organized on-site visits at hospitals to account for medications purchased through the HPP prior to July 2014. An electronic database of drug inventory was compiled to account for baseline quantities of medication at each hospital.
Calculation Tool for Determining Pharmaceutical Cache Size
Between July 2015 and June 2016, the CHSCPR repeated the methodology, with additional recommendations for managing expired pharmaceuticals. The CHSCPR replaced expired pharmaceuticals at hospitals if resources were available, with an added instruction to continue storing expired product. The CHSCPR recommended continued storage of expired pharmaceuticals in the event that adequate funding was not available to provide desired inventory at each hospital and in case a regulatory mechanism was available for the ability to use the expired medications at a later date. No pharmaceuticals were to be destroyed.
The primary goal of the project was to pre-position pharmaceuticals, specifically doxycycline and ciprofloxacin, in Chicago hospitals for anthrax post-exposure prophylaxis, allowing each facility to function as a closed POD for 72 hours. If funding were available under the HPP to meet the primary goal, then the secondary goal was to pre-position pharmaceuticals for 96 hours of anthrax post-exposure prophylaxis. Our calculation tool (Table 1) determined the number of doses needed for 24 hours of anthrax post-exposure prophylaxis, which was extrapolated to determine quantities for 72 and 96 hours of anthrax post-exposure prophylaxis for each facility. Descriptive analyses were performed to process all data. Analyses were performed on Statistical Package for the Social Sciences version 22.0 (IBM Corporation, Armonk, New York).
Results
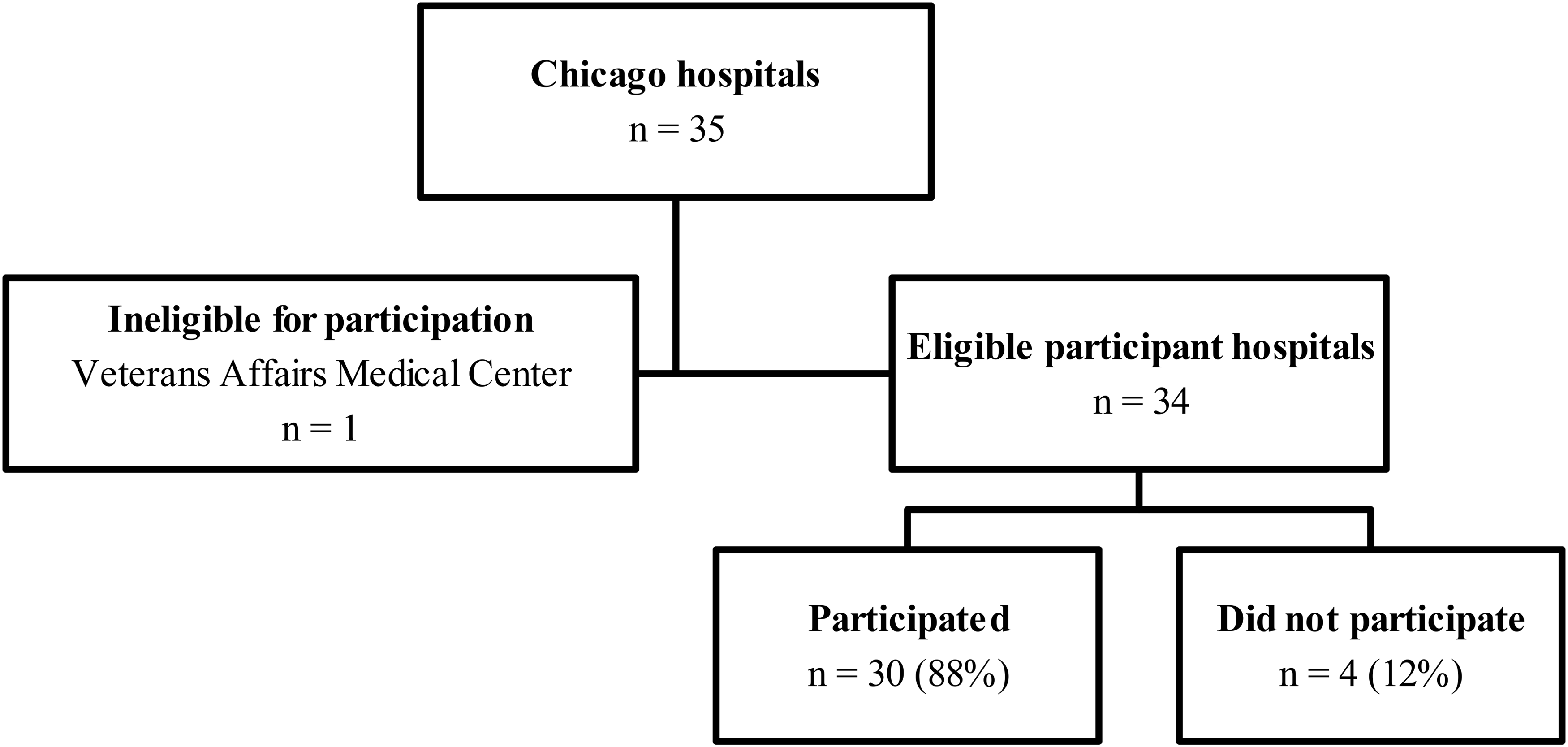
A total of 35 Chicago hospitals were identified, assessed, and invited to participate in this intervention study (Figure 1). Of the 35 hospitals, 1 Veterans Affairs medical center was excluded because of restrictions in receiving grant funding through the HPP. In all, 33 participants representing 18 hospitals received in-person classroom or webinar education regarding appropriate medications for anthrax post-exposure prophylaxis and details outlining our proposed quality improvement project. The CHSCPR contacted hospitals' emergency management and pharmacy directors and emergency medicine pharmacists via email or telephone to encourage participation. Most acute care hospitals and 5 specialty hospitals participated, which included all hospitals with 400 or more inpatient beds (Table 2). Ultimately, 30 (88%) hospitals participated in the transition to a centrally purchased, pre-deployed pharmaceutical cache.
Hospital Participation
Number of Participating Hospitals by Size and Type
Participating hospitals reported a median number of 1,167 hospital employees or staff (interquartile range [IQR] 554 to 2,512). Three hospitals reported no adult inpatient beds, and 8 reported no pediatric inpatient beds. For the 27 hospitals reporting an adult inpatient census, the median number of patients was 120 (IQR 70 to 316). For the 22 hospitals reporting a pediatric inpatient census, 11 reported a census of 10 patients or fewer. The 11 institutions with a pediatric inpatient census of 11 or more reported a median inpatient census of 53 (IQR 17 to 155).
With respect to oral doxycycline and ciprofloxacin, and based on our calculation tool, we identified 17 (57%) hospitals that did not have adequate inventory for all of their employees and patients to receive 24 hours of anthrax post-exposure prophylaxis, and 23 (77%) hospitals that did not have on-site drug inventory for 48 hours of anthrax post-exposure prophylaxis. The compiled inventory database further identified 6 (20%) hospitals that had 72 hours of adequate drug inventory and 3 (10%) hospitals that had 96 hours of adequate drug inventory to operate as a closed POD for anthrax post-exposure prophylaxis.
The necessary quantities of medication needed to establish 72 and 96 hours of anthrax post-exposure prophylaxis were calculated by the CHSCPR, acting as a group purchaser, and negotiated with drug wholesalers to obtain product with maximum shelf-life and discounted pricing. Purchased antibiotics had manufacturer-labeled expiration dates from 24 to 28 months. The 27 hospitals identified without adequate drug inventory received drop shipment medication delivery. The CHSCPR instructed hospitals to continue storing expired pharmaceuticals; however, some hospitals did not have storage space available. For these hospitals, unexpired storage took priority, and CDPH collected expired pharmaceuticals for offsite storage. All 30 participating hospitals received suitable amounts of pre-positioned pharmaceuticals for anthrax post-exposure prophylaxis, as determined by the calculation methodology in Table 1, allowing each facility to function as a closed POD for 96 hours.
Discussion
The CHSCPR enhanced antibiotic MCMs for anthrax post-exposure prophylaxis for Chicago hospitals, with the objective of allowing each facility to function as a closed POD. Through our quality improvement project, the number of Chicago hospitals able to function as a closed POD with onsite medication cache for 72 and 96 hours of anthrax post-exposure prophylaxis increased from 6 and 3 hospitals, respectively, to 30 hospitals.
The HPP historically required awardees to develop pharmaceutical caches for hospital personnel and their families; however, onsite storage at hospitals was not a criterion. 13 In 2008, a report by the US Government Accountability Office identified 20 of 50 states that reported their participating hospitals had access to pharmaceutical caches to provide medication coverage to hospital personnel, associated first responders, and their families. 14 Published data regarding the number of institutions nationwide that have a pharmaceutical cache specifically located on-site is lacking. A sophisticated modeling tool forecasting the effects of an anthrax incident identified taking post-exposure prophylaxis (uptake) as being most influential in averting anthrax cases. 15 These findings further support the CHSCPR's goal of on-site antibiotic MCMs, which increases access and allows rapid initiation of anthrax post-exposure prophylaxis.
Our pre-positioning of anthrax post-exposure prophylaxis at the hospital level accommodates closed POD operations during an incident and reduces the dispensing load at open PODs, because the personnel from 30 hospitals would not need to report to open PODs. Furthermore, our pre-positioning ensures adequate antibiotic supply, which may not be available to hospitals through traditional drug wholesalers as demand rises during an incident. Following closed POD operations, the CDPH's MCM plan provides completion of the remaining 56 days of post-exposure prophylaxis via a central supply depot and the Strategic National Stockpile (SNS). Our pre-positioning of anthrax post-exposure prophylaxis supplements the CDPH's MCM plan, which combines efforts of the HPP and the Cities Readiness Initiative to improve MCMs. To execute the MCM plan, healthcare workers receive, dispense, and administer SNS material to the public as the unfolding of an epidemiologic incident may dictate. This critical protection of workers may enhance the overall SNS response. Through careful planning, training and exercising, and supporting city departments and hospitals, the CHSCPR and the CDPH ensure a seamless supply of anthrax post-exposure prophylaxis to hospital and other affected populations.
Our findings are important because they outline a streamlined supply process for hospitals by developing and using a uniform calculation methodology. The CHSCPR hypothesized minimizing the required information from hospitals would increase participation, and, ultimately, 88% of Chicago hospitals participated with on-site cache storage for anthrax post-exposure prophylaxis. Hospitals not participating still maintain access to off-site pharmaceuticals stored by the CDPH. Of note, we used a factor of 1.8 specific to Chicago data from the US Census Bureau, but that number would require modification for another city or state. 12 A previously published guide recommends a family household factor of 3 to 5 when planning for mass prophylaxis. 16
The investigators' primary goal was met by optimizing costs and simplifying the drug formulary. We considered cost in our purchase of doxycycline versus ciprofloxacin and requested maximum shelf-life from the drug wholesaler prior to executing a single purchase for all hospitals. Lee and colleagues previously reported a useful formula for incorporating cost and shelf-life in determining a cost-effective purchase. 16 By limiting our purchase to tablets in bulk bottles, we minimized storage space requirements for hospitals, and our bulk purchase minimized drug lot numbers. A low variability in drug lot numbers is strategic, because it may be eligible for use after the manufacturer-labeled expiration date if reviewed by the FDA and assigned a new expiration date under the jointly supported FDA/Department of Defense Shelf Life Extension Program, or via another mechanism available to the FDA to extend the dating. The CHSCPR makes no assumption that state and locally purchased pharmaceutical caches will be reviewed but recognizes that uniform lot numbers lessen the burden of testing. On-site storage of unexpired pharmaceuticals took priority, and expired pharmaceuticals were collected for offsite storage by CDPH as needed.
Prior to our intervention, Chicago hospitals self-managed purchasing of antibiotic MCMs with guidance from the CHSCPR to rotate on-site inventory annually in an effort to minimize quantities of expired antibiotics. Most hospitals stored tens of thousands of antibiotic doses in their pharmaceutical cache while using only hundreds of antibiotic doses annually. Furthermore, formularies differed between hospitals, and some did not stock ciprofloxacin. The ability to rotate stock was limited and resulted in minimal benefit. The bulk purchase made by the CHSCPR supplemented the baseline inventory of antibiotic MCMs purchased by hospitals prior to our intervention. Based on baseline inventory, portions of each hospital's pharmaceutical cache expire at different times, thus spreading out the financial burden of sustainment across HPP budget periods. Similarly, the bulk purchase made by the CHSCPR contained manufacturer-labeled expiration dates that also span 2 HPP budget periods. Our streamlined process did not definitively solve the issue of managing expired pharmaceuticals, but it made the financial burden manageable for the CHSCPR.
Our streamlined process is not without limitations. First, our purchase focused solely on doxycycline and ciprofloxacin, but other bioterrorism threats exist. Fortunately, doxycycline and ciprofloxacin are broad spectrum oral antibiotics that cover additional threats, including tularemia and plague.17,18 We focused on optimizing financial costs and minimizing storage space requirements at facilities by purchasing bulk bottles. However, bulk bottles require resources for repackaging and dispensing in a disaster scenario, and pediatric doses may require personnel to compound liquid formulations. To facilitate compounding, instructions may be available for parents to create liquid doxycycline from tablet formulations for infants and children in a disaster scenario. 19 Lastly, the calculation tool is based on consensus from the authors and has not been validated in a prospective disaster scenario.
Future directions for the CHSCPR are focused on sustaining the established process, such as maintaining a central database to appropriately replenish inventory annually. While all hospitals still maintain access to off-site medication MCMs, the CHSCPR will continue to encourage all Chicago hospitals to participate in the storage of on-site MCMs for immediately available anthrax post-exposure prophylaxis. Cost savings from the bulk purchase associated with this project will allow further purchases of medications for additional threats—for example, cyanide antidote kits.
In conclusion, this systematically calculated, predeployed pharmaceutical disaster cache enhanced availability of antibiotic MCMs for anthrax post-exposure prophylaxis in 30 Chicago hospitals. Hospitals received adequate stock for 96 hours of anthrax post-exposure prophylaxis, thus allowing each facility to safely and securely function as a closed POD.
Footnotes
Acknowledgments
Funding for this project was provided by the Chicago Department of Public Health through a cooperative agreement from the US Department of Health and Human Services, Office of the Assistant Secretary for Preparedness and Response, Office of Emergency Management, Division of National Healthcare Preparedness Programs, Hospital Preparedness Program.