
Abstract
This integrative review examines extant literature assessing the burden and management of noncommunicable diseases 6 months or more after earthquakes and tsunamis. We conducted an integrative review to identify and characterize the strength of published studies about noncommunicable disease–specific outcomes and interventions at least 6 months after an earthquake and/or tsunami. We included disasters that occurred from 2004 to 2016. We focused primarily on the World Health Organization noncommunicable disease designations to define chronic disease, but we also included chronic renal disease, risk factors for noncommunicable diseases, and other chronic diseases or symptoms. After removing duplicates, our search yielded 6,188 articles. Twenty-five articles met our inclusion criteria, some discussing multiple noncommunicable diseases. Results demonstrate that existing medical conditions may worsen and subsequently improve, new diseases may develop, and risk factors, such as weight and cholesterol levels, may increase for several years after an earthquake and/or tsunami. We make 3 recommendations for practitioners and researchers: (1) plan for noncommunicable disease management further into the recovery period of disaster; (2) increase research on the burden of noncommunicable diseases, the treatment modalities employed, resulting population-level outcomes in the postdisaster setting, and existing models to improve stakeholder coordination and action regarding noncommunicable diseases after disasters; and (3) coordinate with preexisting provision networks, especially primary care.
This integrative review examines extant literature assessing the burden and management of noncommunicable diseases 6 months or more after earthquakes and tsunamis that occurred from 2004 to 2016. Results demonstrate that existing medical conditions may worsen and subsequently improve, new diseases may develop, and risk factors, such as weight and cholesterol levels, may increase for several years after an earthquake and=or tsunami.
D
The impact of natural disasters on chronic disease has been increasingly discussed in the literature.14-17 Medication shortages, interruptions in care, displacement, and destruction of critical infrastructure have been identified as key barriers to care in the postdisaster phase.18-23 Regardless of the progress in this field, a recent review examining recommendations for chronic illness management in disasters concluded that more evidence-based recommendations are needed, and the shortage of evidence on noncommunicable disease interventions in humanitarian settings has also recently been highlighted.24,25 Existing approaches to address these issues focus primarily on prevention of acute exacerbations of existing noncommunicable diseases and interruptions in treatment, while recognizing that, ideally, these efforts would synergize with existing efforts to improve noncommunicable disease care outside of disaster settings.15,26,27
Much of the extant research examines noncommunicable disease–specific outcomes and interventions immediately or soon after a disaster.28-34 For example, acute health impacts of earthquakes 3 months postdisaster have been characterized elsewhere and focus primarily on traumatic injury and its sequelae. 2 However, it was recently suggested that acute and long-term complications related to noncommunicable diseases postdisaster need to be better characterized in terms of their morbidity and mortality.14,24
In this integrative review, we address these gaps by examining the research literature on noncommunicable disease–specific outcomes and interventions in the more protracted phase after a disaster. Because noncommunicable diseases are chronic illnesses that develop, stabilize, and evolve over longer periods, we focus on outcomes that manifested 6 months or more after a disaster. We focus on earthquakes and tsunamis because of their tremendous potential for human impact and physiological and emotional stress, all of which are thought to mediate worsening outcomes for those with existing disease and the development of new disease.2,35-37 Although they manifest differently, both tsunamis and earthquakes are caused by the abrupt shifting of tectonic plates. Studies have examined how individuals and health systems might respond to noncommunicable diseases in a disaster setting, but to our knowledge this is the first effort to rigorously review both the content and quality of literature and characterize how noncommunicable diseases develop or deteriorate in the non-acute phase after a specific type of disaster. In addressing this gap, we aim to contribute to the formation of specific, evidence-based plans and recommendations for noncommunicable disease management in postdisaster settings beyond the immediate disaster phase.
Methods
Prior to conducting this integrative review, we identified reviews focused on: (1) existing disaster preparedness recommendations and guidelines for chronically ill patients; (2) noncommunicable disease outcomes after cyclone-, storm-, and flood-related disasters; and (3) select impacts of natural disasters on cardiac, renal, and diabetic patients. This review proceeded given that a different type of disaster was being considered, as well as the fact that one of the identified reviews, and several other publications, have called for more evidence to inform postdisaster, noncommunicable disease–related recommendations.14,24,25,38,39
We adapted our methodology from that of several published integrative reviews that focused on different aspects of emergency preparedness.40,41 We sought to identify and characterize the strength of published studies about noncommunicable disease–specific outcomes and interventions at least 6 months following an earthquake or tsunami.
Search Strategy
We searched the following health-oriented databases: PubMed, EMBase, CINAHL, SCOPUS, and Web of Science. We initially developed our search terms using a priori knowledge and experience with prior research in this area. 36 To refine our search terms, we consulted an informationist. *
The search was performed on February 15, 2017. The date range for the search was January 1, 1970, to February 15, 2017.
Inclusion Criteria
Articles were included if they were original peer-reviewed quantitative or qualitative studies published in English that considered diagnosis, management, and/or outcomes of noncommunicable diseases at least 6 months after an earthquake or tsunami. Abstracts, conference proceedings, and grey literature in the form of reports or anecdotes were not included. We defined noncommunicable diseases in accordance with the World Health Organization (WHO) as cardiovascular disease, respiratory disease, cancer, and diabetes, although we also recognized that noncommunicable diseases refer broadly to nontransmissible conditions. 42 We included various forms of renal disease, given that its 2 most common causes are hypertension and diabetes, both considered noncommunicable diseases under the WHO designation. 43
Compared to communicable disease, a distinction of noncommunicable diseases is the inability to biologically transmit these illnesses, although data have shown that familial patterns of behavior can contribute to risk, incidence, and prevalence of noncommunicable disease risk factors, such as smoking and dietary patterns.44-46 Therefore, studies addressing clear and known risk factors for noncommunicable diseases (eg, smoking, body weight) were included, as were studies that highlighted chronic, nonspecific, nontransmissible symptoms present at least 6 months postdisaster. Although high body mass index (BMI) and smoking are considered risk factors, they are also medical conditions (eg, obesity, addiction) with a long history of causal association with several of the WHO's noncommunicable disease designations.47-49
Because much of the literature in this area is anecdotal, commentary, or experience-driven, or based on small studies or case reports, we adopted a 50-subject minimum for study inclusion, previously used in literature addressing a similar topic.2,50-57 If a notable finding existed in a study that addressed noncommunicable diseases and other outcomes (eg, those not involving noncommunicable diseases), only the relevant information was included in this review.
Exclusion Criteria
Our primary exclusion criterion was literature focused on evaluating mental health outcomes postdisaster. In contrast, we included literature in which psychiatric, psychosocial, or psychological variables were assessed as predictors of or having relationships with other noncommunicable diseases being assessed as outcomes. During our title review phase, we excluded studies in which the primary focus was the short- or long-term burden of wounds, injuries, and surgical conditions, as this has recently been explored. 2
During our abstract review phase, we applied the following additional exclusions: literature evaluating earthquakes and tsunamis that occurred before 2004; addressing nonspecific quality of life measures; chronic pain; long-term injury-related disability and rehabilitation burden, outcomes, and interventions; obstetric and/or gynecological outcomes; and nutritional status or interventions. We selected 2004 as the cutoff event year because of the concentration of literature around major disasters that occurred in and after that year, including the 2004 Indian Ocean Earthquake, the 2010 Haiti Earthquake, and the 2011 Great East Japan Earthquake. The various content areas were excluded either because existing reviews were identified or the area was determined to be a separate and distinct field of study and research beyond the scope of noncommunicable diseases. 58 We excluded studies related to the Great East Japan Earthquake that primarily examined the effects of the subsequent radiologic disaster (eg, radioactive environmental exposure or impact of evacuation associated primarily with residence in the evacuation zone) rather than evacuation or displacement associated with the earthquake or tsunami itself.
During abstract review, we selected 6 months as the postdisaster outcome threshold, given previous research examining the impact of earthquakes within 3 months and given our previous rationale that assessing impact on this time horizon would more accurately characterize longer-term noncommunicable disease outcomes once the burden of wounds, injuries, communicable disease, and acute exacerbations of chronic illness had lessened. 2 Given the paucity of this literature, if noncommunicable disease outcomes were assessed both prior to and after 6 months postdisaster in the same study, articles were included, and our synthesis and discussion of them focused primarily on results occurring at least 6 months postdisaster. If studies collected data up to, but not past, 6 months, data from the 6-month mark were included.
Article Review Protocol
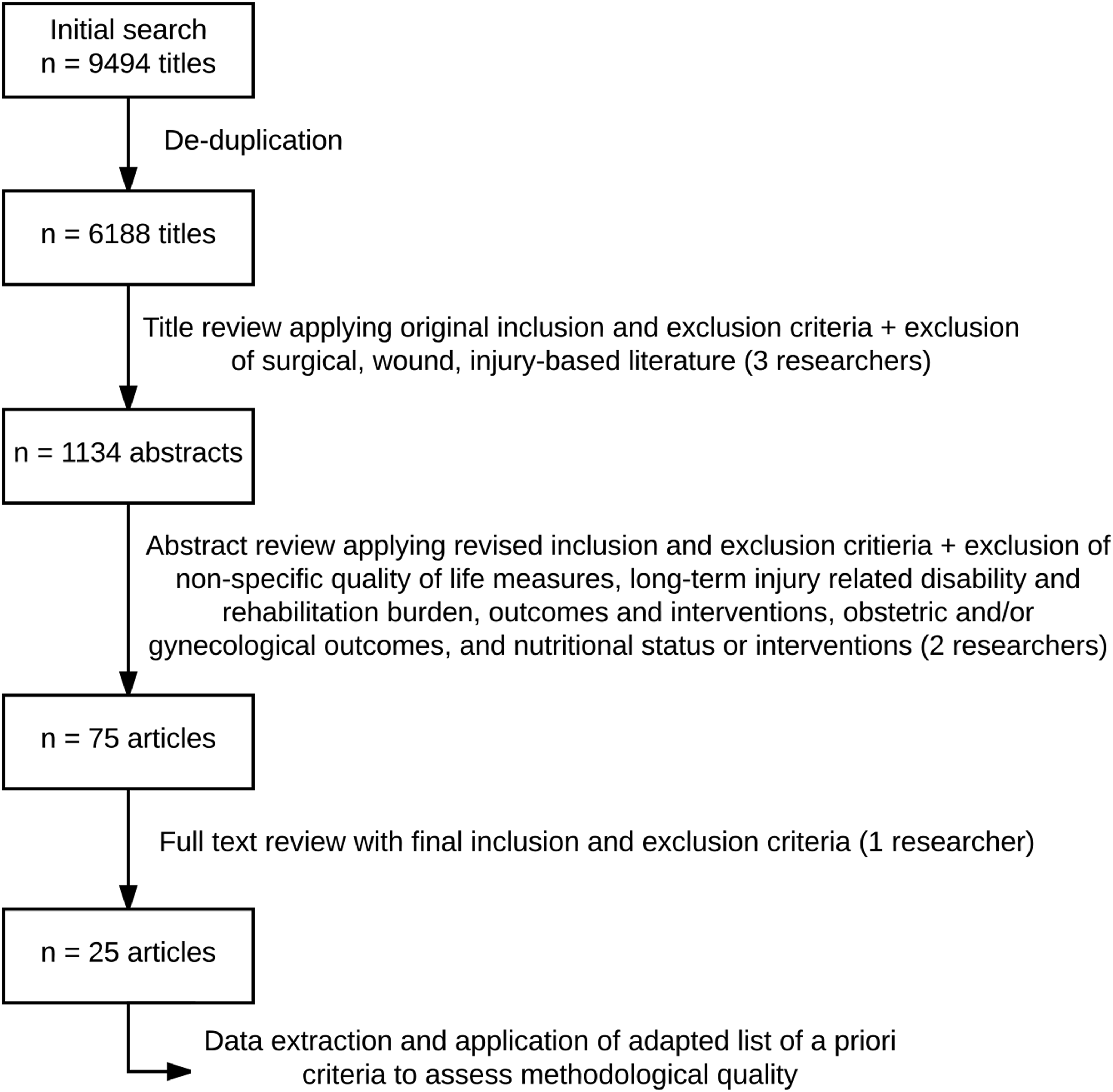
Our initial search yielded 9,494 results. After removing duplicates, 6,188 results remained (Figure 1). All titles were screened for relevance by one co-author (AS) and concurrently reviewed by a second co-author (LR or MG). Differences in recommendation for title inclusion were reconciled via discussion and consensus among co-authors. After title review, 1,134 articles remained for abstract review. Two co-authors (AS and LR) reviewed all abstracts, with differences in recommendation for abstract inclusion reconciled via discussion and consensus among co-authors. After abstract review, 75 articles remained for full text review. After full text review, 25 articles remained. The most common reasons for exclusion after full text review were: (1) on further examination, the item was an abstract or poster (n = 21); (2) the article examined the impact of the nuclear disaster resulting from the Great East Japan Earthquake rather than the earthquake or tsunami itself (n = 10); and (3) data were collected less than 6 months postdisaster (n = 8).
Review Protocol
Each of the 25 final articles was evaluated with an adapted version of criteria used in previous disaster preparedness research as well as other fields (see Figure 1).40,41,59,60 Drawing on these criteria, our assessment of methodological rigor focused on sampling, reliability, validity, and bias. We assessed pretesting as part of our measure of reliability and evaluation of instrument development as part of our measure of validity.
Although qualitative data are not often included in such reviews, they were included here to deepen the nature of our results by including subjectively experienced and/or non–formally diagnosed noncommunicable diseases (eg, chronic physical symptoms).
Results
A total of 25 peer-reviewed articles met inclusion criteria for this review. The distribution of disaster events was: 2011 Great East Japan Earthquake and tsunami (n = 13); 2008 Sichuan Earthquake (n = 3); 2004 Mid Niigata Prefecture Earthquake (n = 3); 2010-11 Christchurch earthquakes (n = 2); 2004 Indian Ocean tsunami (n = 2); other events (n = 2). The articles were published between 2006 and 2016. Data were collected from 6 months to 6 years postdisaster (Table 1).
Overview of Studies by Disaster, Purpose, Methods, Sample and Population Characteristics, Timeframe, and Key Findings
Note: * p < 0.01, ** p < 0.05.
Abbreviations: GEJE, Greater East Japan Earthquake; BMI, body mass index; HbA1c, Hemoglobin A1C; AMI, acute myocardial infarction; REL, relocation group; NCD, noncommunicable disease; OR, odds ratio; RR, risk ratio; CEA, carotid endarterectomy; HDL, high density lipoprotein; SDQ, Strengths and Difficulties Questionnaire; RBCs, red blood cell count; Hb, hemoglobin; Ht, hematocrit
Quality of Research Methodology
Control Group and Predisaster Data
Sixteen studies made pre- and postdisaster data comparisons.61-76 Eight studies used control groups.68,69,71,76,78,79,81,83 Four studies included both of these elements68,69,71,76 (Table 2).
Review of Studies by Design, Control Group, Use of Predisaster Data, Sampling, Validity, and Bias
Abbreviations: a(+) use of control group, (-) no control group; b(+) use of predisaster data, (-) no predisaster data; HbA1c, Hemoglobin A1C; RR, response rate; BMI, body mass index; LDL, low density lipoprotein; HDL, high density lipoprotein; ICD-10, International Classification of Disease-10th revision; WHO, World Health Organization; ISH, International Society of Hypertension; DBP, diastolic blood pressure; SBP, systolic blood pressure; ISAAC, International Study of Asthma and Allergies in Childhood; PTSD, post-traumatic stress disorder; JIS, Japanese Industrial Standards; CK, creatine kinase; CK-MB, creatine kinase-MB; AMI, acute myocardial infarction; RBCs, red blood cell count; Hb, hemoglobin.
Reliability
One study reported a formal measure of reliability (Cronbach's alpha). 79 No other studies explicitly reported measures of reliability.
Validity
The following forms of face validity were addressed. Eight studies provided details regarding collection methodology and technology used for laboratory and anthropometric measures.64,65,68,74,76,77,81,82 Eleven studies used a previously referenced or validated tool for exposure or outcome measurement.64,65,67,68,70,72,76,78,79,81,85 Eleven studies used national or international guidelines for exposure or outcome measurement.63,65,69,71,72-76,80,82 One study used cross-validation with other methods of measurement of the same outcome or exposure. 85 Two studies pre-piloted use of a tool for exposure or outcome measurement.83,84 Two studies used multiple databases or other sources to ensure inclusion of all cases.66,72 Content validity was addressed via explicit mention of expert convening or consensus to decide on diagnostic criteria or measurement methodology for exposure or outcome in 7 studies.62-65,74,79,84 Overall, only 1 study did not address measures of content or face validity. 61 In 8 studies, there was at least 1 outcome or exposure metric for which there was no assessment of either face or content validity.61,62,64,65,73,78,80,84 Only 1 study performed a confirmative factor analysis to assess construct validity, and no studies referenced or assessed criterion validity. 79
Sampling Strategy and Response Rate
Fifteen studies employed convenience sampling, 7 were retrospective data collection efforts using databases or hospital records, and 3 employed random sampling. Four studies had response rates above 50%, and 4 studies had response rates below 25%.68,73,76,78,81,83–85
Bias
Fourteen studies addressed the presence or mitigation of some type of bias, including nonresponse, loss to follow up, missing data, self-selection, reporting, and recall bias.61-63,67-70,72,76,79,81–84 Four studies explained how they attempted to minimize biases, including self-selection, nonresponse, and recall bias, via sampling or study structure.62,63,83,84 Of the 3 studies that addressed nonresponse bias, 1 evaluated characteristics of nonresponders, and of the 3 studies that addressed loss to follow up, 1 evaluated characteristics of those who were lost to follow up.69,79
Power Analyses
Three studies explicitly mentioned power and/or the impact of loss of data or loss to follow up on this measure.69,73,81 One study included a formal power analysis. 83
Disease-Specific Findings
Articles addressed the following diseases, with some addressing more than 1: cardiovascular disease (n = 9), diabetes (n = 6), risk factors for noncommunicable diseases (eg, BMI, cholesterol levels) (n = 6), other chronic diseases or symptoms (eg, back pain, anemia) (n = 6), pediatric illness (n = 3), allergic symptoms (n = 2), and general chronic disease burden (n = 2). Two studies addressed interventions in a postdisaster setting, with the remainder focusing on evaluating burden of disease and its predictors.66,73 No studies evaluated cancer or respiratory disease, 2 of the 4 categories designated as primary noncommunicable diseases by WHO. 42 Two studies addressed development of renal disease as a complication of diabetes postdisaster, and none substantially addressed outcomes in patients with preexisting renal disease.64,65 Twelve studies examined housing, displacement, or housing damage as primary or secondary predictors of noncommunicable disease outcomes.64,65,69,70,74,78,80-85 (Table 1).
Cardiovascular Disease
Studies addressed the long-term impact of earthquakes and tsunamis both on acute cardiovascular events (eg, myocardial infarction) and chronic conditions (eg, heart failure).63,71,72,75 In multiple studies, risk factors for hypertension were identified, with public employment, age, family history of hypertension, diabetes, BMI, waist-hip ratio, sleep quality, and blood glucose identified as risk factors for the development of hypertension or increases in blood pressure.68,80 In one study, morning home blood pressure measurements were lower than clinic blood pressure measurements throughout the study, including predisaster. 65 After the same disaster, acute myocardial infarction increased 4 to 12 months postdisaster in some geographic areas and not others; acute decompensated heart failure increased for 3 years postdisaster in high-impact areas but remained at predisaster levels in low-impact areas.72,75 Hospitalizations for ischemic heart disease, defined in 1 study as inclusive of both acute and chronic cardiac conditions and/or complications, increased for 5 years postdisaster but decreased to predisaster levels after 6 and 7 years. 63 Of the 2 studies examining the impact of noncommunicable disease management postdisaster, 1 observational study determined that a protocol established predisaster for carotid endarterectomy could be regularly and increasingly administered in a postdisaster setting. 66 One study evaluated prevalence of hypertension in postdisaster communities but provided no predisaster baseline for comparison. 77
Diabetes
The potential for disasters to lead to poorer glycemic control, both as a result of environmental factors and stress, has been previously explored. 36 In this review, 4 studies found increased HbA1c values postdisaster, although 3 were <0.5%.64,65,69,82 One study found that the proportion of patients with HbA1c >7.0% increased by 9.5% comparing pre- and postdisaster levels. 69 In the same study, age, female gender, and rural residency were associated with lower HbA1c values. 69 One study evaluated the prevalence of diabetes in postdisaster communities but provided no predisaster baseline for comparison. 77 Of the 2 studies examining the impact of management on noncommunicable diseases postdisaster, 1 found that patients who attended periodic visits for 12 months postdisaster did not experience deterioration of HbA1c values, although this study did not explicitly define the periodic visit measure. 73 Of the articles examining changes in HbA1c values, the postdisaster timeframe was 6 to 12 months.64,65,69,82
Allergic Symptoms
Two studies, both after the Great East Japan Earthquake, addressed the impact of the disaster on allergic symptoms and provided different analyses from the same data collection effort.67,70 In 1 study of schoolchildren in grades 1 to 8, younger age, history of hospitalization, and worse scores on a social difficulties questionnaire were associated with increased allergic symptoms, including current wheeze or asthma and severe wheeze or asthma with few exceptions among grades. 70 Both studies determined that prevalence of eczema symptoms was higher than the Japanese average, although the results were statistically significant only for those in 2nd and 8th grades.67,70
Noncommunicable Disease Risk Factors
Several studies addressed changes in risk factors for noncommunicable diseases, including: (1) weight-related measures (eg, BMI, waist circumference); (2) serum lipid levels (eg, total cholesterol, triglycerides); (3) physical activity; and (4) smoking. Comparing pre- and postdisaster levels, results generally indicated increases in BMI among both children and adults.76,81,82 Among adults specifically, BMI increased by 0.2 kg/m2, body weight by 0.31 kg, and waist circumference by 0.58 cm.81,82 Results were more variable among children, with 1 study reporting increases in BMI among boys and girls (0.137 kg/m2 and 0.200 kg/m2, respectively) in the Fukushima Prefecture 19 months postdisaster and decreases in BMI among boys and girls (0.218 kg/m2 and 0.082 kg/m2, respectively) in the Miyagi Prefecture 19 months postdisaster. 76 Two studies reported significant changes in serum lipid levels, including decreased high-density lipoprotein cholesterol levels (0.96 mg/dL) and increased triglycerides (0.17 mmol/L).81,82 Other important risk factors were also addressed, including physical activity and smoking. In Christchurch, 24% of ex-smokers had resumed smoking, and 34.1% of current smokers had increased consumption 15 months postdisaster. 61 After the Great East Japan Earthquake, elderly patients who had been displaced, lacked social connections, and/or were not working had lower rates of physical activity. 85
Other Diseases and General Burden
Several other chronic diseases outside the WHO noncommunicable disease designations were addressed by studies included in this review, including increases in neuro-otologic diseases and low back pain.62,78 More generally, chronic disease prevalence and morbidity comparing harder-hit areas to less-hit areas was higher 3 years after disaster, and 2 studies demonstrated increases in chronic nonspecific symptoms more than 1 year postdisaster.79,83,84
Discussion
The articles examined in this review represent a broad array of noncommunicable diseases that progress and often develop over several months to years after an earthquake or tsunami and focus primarily on evaluating the burden of disease.
While cardiovascular disease was the most well represented noncommunicable disease, results were variable in demonstrating a clinically significant, protracted impact of disaster. Existing evidence strongly supports the hypothesis that acute physiological or psychological stress after disaster leads to increases in negative cardiovascular events such as myocardial infarction and arrhythmias.35,37 The results of our review suggest that the protracted effects on some cardiovascular disease outcomes—myocardial infarction and acute heart failure exacerbations—may persist for several years after a disaster.71,72 Studies of hypertension rarely compared pre- and postdisaster data, and in the instances where comparisons were made, data were not collected beyond 8 months postdisaster.65,68 Data from 1 study on carotid endarterectomy protocol execution suggests that interventions can be reliably administered postdisaster. 64
Results also supported increases in nonspecific chronic physical symptoms following a disaster. This finding is unique compared to previous studies, which have focused primarily on the WHO noncommunicable disease designations.24,38,39 Given recent data on the global impact of low back pain as the main cause of disability worldwide, the impact of chronic nonspecific symptoms cannot be ignored. 86
According to the studies in our review, more psychologically mediated noncommunicable disease risk factors like smoking and physical activity worsened following an earthquake or tsunami.61,85 These results suggest that postdisaster deteriorations in mental health outcomes may have an overflow effect on noncommunicable disease outcomes.
No articles addressed respiratory disease or cancer, or substantially addressed renal disease, which have unique and intensive resource and personnel requirements that necessitate specific consideration in preparedness efforts (eg, respiratory failure and the need for supplemental oxygen, medications for long-term chemotherapy or radiation treatment, and resources and personnel to administer dialysis). Few articles addressed the benefit of various treatment modalities postdisaster.66,73 Because disasters can result in variable levels of resource limitation depending on several factors (eg, preexisting stock, severity of disaster, level of preparation, geographic distribution of various healthcare and administrative personnel), it is important to understand whether existing patterns of care are feasible and effective in postdisaster settings or if new standards can be an effective bridge to reestablishing predisaster resource levels. Although issues with the medication supply chain and the impact of disaster on critical medical infrastructure have been identified as relevant to noncommunicable disease outcomes, no literature was identified that linked these issues to noncommunicable disease outcomes in the earthquake or tsunami setting.19,22,87
This review builds on existing literature by examining noncommunicable disease outcomes in the form of exacerbation, deterioration, or development of new disease. Literature examining the impact of other types of disasters, such as Hurricane Katrina, has supported the prevalence and severity of chronic disease needs in the postdisaster setting and led to the proposal of a network-based model to ensure continuity of care after natural disasters.18,19,21,30,53,55,88,89 Overall, our results demonstrate the following when considering noncommunicable disease diagnosis and management post-earthquake or -tsunami: (1) existing conditions may worsen and potentially improve or normalize over time; (2) new conditions may increase in prevalence or incidence or may follow the same pattern; (3) changes demonstrated in the literature may not be clinically significant; and (4) there are often specific variables that place populations at higher risk of experiencing negative noncommunicable disease–related outcomes. Our study is unique in its focus on chronic disease outcomes extending into the recovery period.
While some studies suggest mechanisms underlying the types of longer-term postdisaster changes in physiologic parameters and disease outcomes explored in this review, they are not completely understood.35,37 It has been suggested that psychological stress from the event itself, personal loss, and displacement contribute to an array of worsening health outcomes. 77 Indeed, of the articles we reviewed, almost half measured displacement, relocation, or property damage as a primary or secondary predictor of noncommunicable disease outcomes, suggesting that this is an important factor to consider to understand how resulting psychosocial outcomes may modulate, or spill over, to noncommunicable diseases.64,65,69,70,74,78,80-85
Recommendations
Our findings demonstrate that postdisaster noncommunicable disease considerations extend beyond acute exacerbations and include the development of new disease and complex, disease-specific temporal patterns of clinical and laboratory-based deterioration and improvement. In light of these findings, we make the following recommendations for practitioners and researchers:
• Plan for noncommunicable disease exacerbations and shifting disease burden postdisaster: Noncommunicable diseases should be considered well into the recovery phase postdisaster. We recommend that planning and responding agencies account for the longer-term impacts of disaster on noncommunicable diseases demonstrated here. One way to achieve this may be through pre- and postdisaster chronic disease surveillance, which would allow better understanding of local disease burdens in order to inform the most appropriate and efficient responses.
15
• Increase research on postdisaster noncommunicable disease burden, treatment modalities, outcomes, and the effectiveness of existing models for managing noncommunicable diseases after disasters: This review demonstrates that disasters may temporarily alter disease burden compared to projected trajectories. However, data are not robust or generalizable enough to know how long such an increased burden will last or what its magnitude will be. Thus, we recommend that more research be conducted to determine postdisaster noncommunicable disease burden, treatment modalities, and outcomes to aid in planning for changes in noncommunicable disease burden and resource availability postdisaster. We call for this research especially around noncommunicable diseases without any studies identified in this review: cancer, respiratory disease, and kidney disease, a gap that other authors have also recently identified.
90
This is likely to necessitate establishing long-term postdisaster surveillance of noncommunicable diseases, much like the Fukushima Health Management Survey launched after the Fukushima Dai-ichi Nuclear Power Plant disaster or the formation of the Disaster Cardiovascular Prevention Network.54,91 Although we call for increased research in this area, we also recognize that several authors have proposed models to address chronic diseases after natural disasters, including a network-based model for institutional coordination and another examining the role for improved public health infrastructure resilience in reducing chronic disease exacerbations after disaster.21,92 We call for increased implementation and evaluation of these methodologies as well. • Coordinate response planning regarding noncommunicable disease management with existing healthcare systems: Postdisaster efforts to address noncommunicable diseases will hopefully strengthen healthcare system response to these diseases overall, but predisaster preparation should also include coordination with existing healthcare infrastructure, especially primary health care.
93
We recommend coordinated response planning to accommodate changes in postdisaster noncommunicable disease burden and management with existing healthcare systems, especially in the area of primary care, so that redundant efforts are not undertaken and agencies can continue to employ and distribute their resources most efficiently.
Limitations
Our study has several limitations. First, we included only articles originally published in English. As a result, relevant literature may not have been included in this review. Because many noncommunicable diseases take time to develop or worsen over years, literature examining the impact of events from earlier decades may highlight and demonstrate different findings, even though we excluded this literature. In addition, the majority of articles address disasters that occurred in developed countries, with half of the articles addressing 1 disaster specifically: the Great East Japan Earthquake. This may affect the generalizability of our findings, since the disease burden, baseline, and postdisaster resource availability, as well as level and nature of disaster preparedness and response, are likely to be very different between developed countries like Japan and developing countries. Furthermore, due to the varied nature of the included studies, we were unable to categorize studies as occurring in primarily urban or rural areas, even though important differences may exist between these settings. Similarly, given the nature of the studies, we were unable to assess any possible impact of events on older populations, which may face different noncommunicable disease challenges after disasters. Finally, we recognize that some regions remain concerned with earthquake risk only and others are at greater risk for tsunamis. Thus, we separate our presentation of the literature into disaster types (ie, earthquake only, tsunami only, combined earthquake and tsunami). However, we maintain an aggregated approach to analyzing the overall findings, given the small number of studies for each disaster type and absence of clear trends within the literature confined to a single disaster type. Despite the noted limitations, we submit that the overall trends we identify in this study support research on other types of disasters and provide valuable insights in adopting an all-hazards approach to addressing this issue.
Conclusion
This review has demonstrated that earthquakes and tsunamis can have prolonged effects on noncommunicable disease outcomes. Our findings contribute to existing calls for increased research on noncommunicable diseases postdisaster and demonstrate the continued need for additional research to determine the burden of noncommunicable diseases and the effectiveness of various treatment modalities postdisaster, especially in developing countries, and on several important noncommunicable diseases, including cancer, respiratory disease, and renal disease. Varied patterns of postdisaster disease progression make deep, local understanding of predisaster disease burden—via surveillance and coordination with existing primary care providers and systems—essential in conducting preparedness activities to respond to noncommunicable diseases after a disaster.
Footnotes
*
The following search string was used in PubMed and adjusted to the search query syntax required by the other databases: (tsunamis[mesh] OR earthquakes[mesh] OR tsunami*[tiab] OR earthquake*[tiab]) AND (chronic disease[mesh] OR multiple chronic conditions[mesh] OR chronic disease*[tiab] OR multiple chronic condition*[tiab] OR multiple chronic illness*[tiab] OR chronic illness*[tiab] OR post disaster*[tiab] OR non communicable[tiab] OR cardiovascular disease[mesh] OR neoplasms[mesh] OR respiratory tract diseases[mesh] OR diabetes[mesh] OR cardiovascular disease*[tiab] OR neoplasm*[tiab] OR respiratory tract disease*[tiab] OR diabetes[tiab] OR chronic kidney disease-mineral and bone disorder [mesh] OR chronic kidney disease-mineral and bone disorder [tiab] OR renal insufficiency [mesh] OR renal insufficiency [tiab] OR cerebrovascular disorders [mesh] OR cerebrovascular disorder*[tiab] OR wound*[tiab] OR chronic pain [mesh] OR chronic pain [tiab] OR nutrition disorders [mesh] OR nutrition disorder*[tiab] OR renal dialysis[mesh] OR renal dialysis [tiab]).