
Abstract
The Johns Hopkins Hospital created a biocontainment unit (BCU) to care for patients with highly infectious diseases while assuring healthcare worker safety. Research to date for BCU protocols and practices are based on case reports and lessons learned from patient care and exercises. This study seeks to be the first to explore the influences of healthcare worker movement and personal protective equipment (PPE) doffing on the transport of simulant pathogen particles in a BCU. A cough device released 1 μm fluorescent polystyrene beads (PSLs) in the patient room. PSL transport was then examined under 2 scenarios: (1) PSL release only, no healthcare workers; and (2) PSL release during 5-minute simulated activity by healthcare workers. Airborne PSL concentrations were quantified every second for 30 minutes per scenario by 7 optical particle sensors located throughout the BCU. PSLs were not detected in the donning room at any time nor in the doffing room during the first test scenario where no healthcare worker was present. The main difference detected between the tested scenarios was the presence of PSLs in the doffing room when healthcare workers were removing PPE, potentially due to re-aerosolization of PSLs off the exterior PPE surface or opening of the patient room door. Future work will further explore the potential for re-aerosolization of particles off of PPE during doffing. The present study provides the groundwork for a systematic method for evaluating the BCU and doffing procedures for their respective safety, and it also pilots a systematic method for evaluating potential pathogen exposure pathways for BCU healthcare workers.
This study explores the influences of healthcare worker movement and personal protective equipment doffing on the transport of simulant pathogen particles in a biocontainment unit. It provides the groundwork for a systematic method for evaluating the safety of the biocontainment unit and of the doffing procedures.
I
Professionals in the global health security community have previously highlighted the need for standardized planning, design, construction, and operations of clinical biocontainment units (BCUs) across the United States.9,10 BCUs are one critical component of a multifaceted preparedness approach to isolating and effectively caring for patients infected with special pathogens while minimizing the risk of secondary transmission and protecting broader healthcare infrastructure.9,11 While hospitals routinely treat infectious disease patients, there is a need to develop capacity to care for patients with special pathogens. Special considerations include potential failure points, including infrastructure malfunction, PPE failure, healthcare worker error, and the related issue of healthcare worker anxiety when treating patients infected with special pathogens. 9 Thus far, most clinical BCU-related research has been limited to case studies and recommendations from lessons learned based on observations during patient care in the BCU environment.11,12 Observed challenges include disposal of BCU-generated medical waste, 13 patient discharge, unit decontamination, 14 and patient transport by emergency medical services. 15 There is an extensive body of research regarding PPE use and decontamination in biosafety level 4 (BSL-4) laboratories; however, the mandated use of positive-pressure personal containment suits changes the landscape of the doffing procedures significantly.16,17 These suits are physically connected to the infrastructure of the laboratory and are reusable, allowing for standardized shower-in/shower-out decontamination procedures. The mostly disposable PPE of the clinical BCU limits the utility of this body of evidence in informing practice. Therefore, the selection of PPE and the associated donning and doffing procedures (ie, putting on and removing) vary widely based on the availability of PPE and the specifications of individual BCU facilities.11,18,19 While guidelines exist, PPE protocols are not standardized, nor are they consistently validated. 11
In response to the Ebola epidemic, the Assistant Secretary for Preparedness and Response (ASPR) funded the creation of 10 Regional Ebola and other Special Pathogen Treatment Centers (RESPTCs) in the United States to provide care for patients infected with high-consequence pathogens, such as EVD, MERS, and H7N9 influenza. 20 The Johns Hopkins Hospital is the Region 3 RESPTC. 21 In addition to the technological and environmental safeguards of the Johns Hopkins BCU's built environment, extensive healthcare worker training is required to work on the BCU, including the proper donning and doffing of PPE. 9 However, there are no formal guidelines for constructing BCUs, specific capabilities are not mandated and vary among the different facilities, and there are few data examining the safety of any BCU environment, including protocols for patient care.9,11,21,22 In light of the 2014-15 EVD epidemic, and considering the increased number of BCUs established as a result, the need for systematic research on the safety of BCU facilities and their protocols is apparent.
A cough simulator 23 that was designed to mimic coughs from a patient with a respiratory virus such as influenza, to disperse simulant pathogen particles (fluorescent polystyrene latex microspheres, or PSLs), was used in the Johns Hopkins Hospital BCU. The spatial distributions and airborne concentrations of the PSLs were examined before and after simulated patient care activities and during healthcare worker PPE doffing with a doffing partner. This research will inform the development of a method for identifying and analyzing critical points at which healthcare workers have the potential to be exposed to highly infectious pathogens while working in a BCU. While this research focuses on the protocols used at the Johns Hopkins BCU, future research will include validation of this method at additional BCUs and with different protocols for patient care and PPE use.
Materials and Methods
Biocontainment Unit Specifications
The Johns Hopkins Hospital BCU is a dedicated, stand-alone unit with 3 patient rooms that can treat up to 4 patients (eg, a pregnant mother and child, or 2 patients infected with the same pathogen in the large patient room). All tests for this study were conducted in the large patient room, the dedicated donning and doffing areas for that room, and the main hallway (Figure 1). A detailed description of the Johns Hopkins BCU, including a summary of its unique features compared to existing BCUs, has been reported previously. 21 Briefly, the entire BCU is under negative pressure relative to the rest of the hospital, with a negative pressure gradient from the clean areas to the contaminated areas of the unit. Contaminated areas are maintained at a pressure differential of at least −0.2 inches water gauge (wg) to adjacent areas. The patient care room pressures are negative to the donning and doffing rooms, which are, in turn, negative to the main hallway. Air from the patient rooms is exhausted through 2 high-efficiency particulate air (HEPA) filters on the roof. The negative pressure is maintained through 2 rooftop fans, each of which is capable of running the negative pressure for the entire unit. Supply air is 100% outside air and is filtered using a minimum efficiency reporting value 16 filter capturing 99% of 1-μm particles. The patient room undergoes a minimum of 12 air changes per hour, while the hallway and donning and doffing rooms undergo at least 10 air changes per hour.
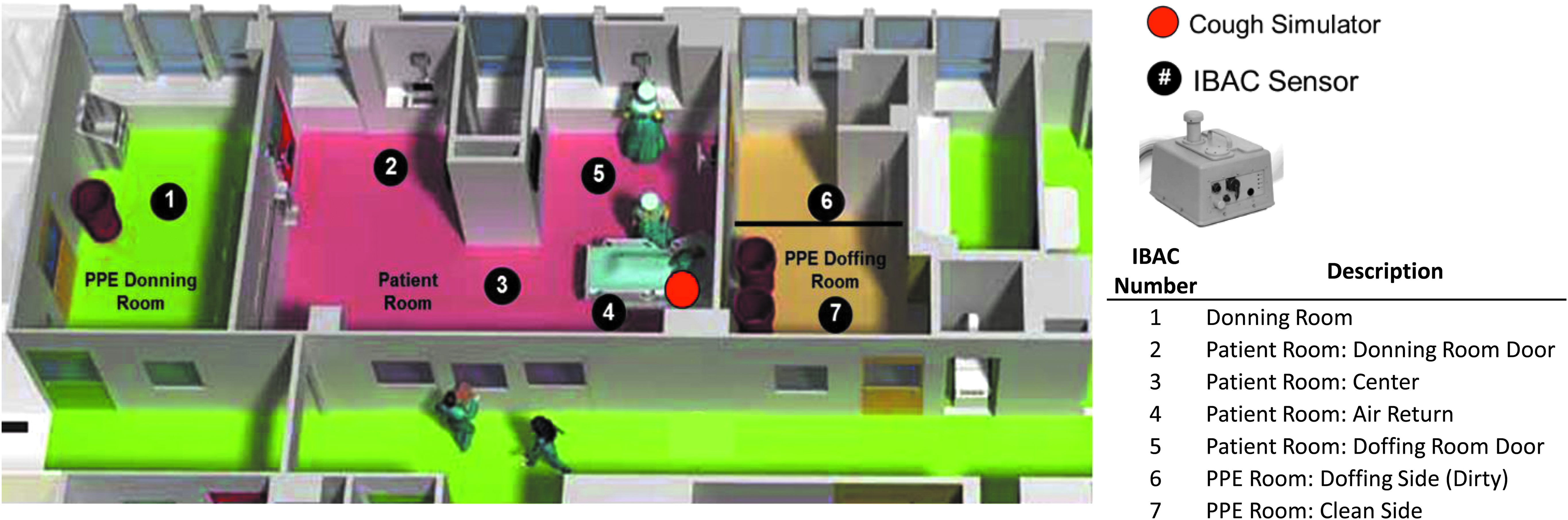
General Layout of the Biocontainment Unit (BCU). Each patient room has separate dedicated spaces for donning and doffing personal protective equipment (PPE). This allows unidirectional flow to reduce the risk of cross contamination. Green indicates clean space in the hallways and donning room. In the patient room, red indicates contaminated space. The doffing room is yellow and has a designated dirty side where the healthcare worker enters the doffing space to remove PPE. The other side of the doffing room is designated as the clean side because the healthcare worker steps into the clean side after removing all PPE (see the doffing procedures in the SupplementalMaterial). The actual designation of the clean and dirty sides of the doffing space is indicated by a marker on the floor. This figure used by permission from the Johns Hopkins Health System Corporation.
Cough Simulator
A biomimetic coughing device (cough simulator) developed by the National Institute for Occupational Safety and Health (NIOSH) was used to generate a reproducible artificial cough that mimics the typical flow rate, airflow profile, and aerosol particle size range of a cough from a patient infected with influenza virus. 23 The coughing device was placed near the patient bed in the patient room of the BCU (red circle in Figure 1). The device consisted of a lung-like bellows, a mouthpiece for particle exhaust, and an aerosol generator (3-jet Collison Nebulizer, Mesa Laboratories, Inc, Butler, NJ). The nebulizer was run for 1 minute at 5 L/min (20 psig) to nebulize a 40-mL suspension of 1-μm diameter PSL particles (Polysciences, Inc, Warrington, PA, Catalog No. 17154) diluted in sterile, deionized water at a ratio of 1:10. During PSL nebulization, the particles were drawn into the bellows by vacuum pressure. The airflow to the Collison nebulizer was then switched off, and the bellows were compressed upward in a linear motion to produce a cough with a total expelled air volume of 4.2 liters per cough. 23 The fluorescent PSLs were forced out of the mechanical lung bellows and entered the BCU through the mouth port of the device, forming a stream that widened as it dispersed. The chosen number of coughs for testing (1 or 2 back-to-back coughs) is described below.
Fluorescent PSL Test Particles and Aerosol Instrumentation
Fluorescent PSLs are commonly used as simulant particles for bioaerosol studies. 24 They are a safe, nontoxic material that is approved for release into public environments by the US Department of Homeland Security and the Environmental Protection Agency. 25 The intense fluorescence emission spectrum of PSLs permits quantification relative to background particles (eg, dust or other debris). The traceability of fluorescent PSLs is advantageous, as it provides a standard beyond traditional qualitative assessment approaches (eg, smoke testing).26,27 A PSL size of 1 μm was chosen as this is a typical aerodynamic diameter of airborne bacteria. 28 Additionally, the particle size falls within both the World Health Organization airborne transmission criteria of less than 5 μm 29 and the size range of viral pathogen transmission studies. 30
After release by the cough simulator, the fluorescent PSLs were detected and counted by an array of Instantaneous Bio-Analyzer and Collector (IBAC) sensors (FLIR Systems, Inc, Elkridge, MD). Operating at 3 to 4 L/min, the IBAC is a real-time optical particle counter that uses ultraviolet laser-induced fluorescence (UV-LIF) technology to count biological aerosols or other fluorescent particles based on elastic scattering and fluorescence emission.31,32 The locations of these sensors were selected by BCU-trained staff, BCU facility engineers, and aerosol subject matter experts to optimize the data collection for these experiments. Particles are excited by a continuous-wave laser beam, and elastic scatter is measured to determine particle size and concentration. Simultaneously, the wavelength of the light emitted from the particles is captured to measure fluorescence. For the following tests, the frequency of fluorescent particles in the size range of 0.7 to 10 μm detected over time were measured as cumulative particle counts (number of particles per liter of air over time).
In Figure 1, each black circle corresponds with the placement of IBACs throughout the BCU, with numbers and a table describing exact locations. To detect and characterize the spread of released PSLs, there were 4 IBACs in the patient room, 1 IBAC in the donning room, and 2 IBACs in the doffing room (1 on the clean side of the doffing room, and 1 on the dirty side). All IBACs were positioned on tables about 1 meter off the floor, with the exception of IBAC #4, which was located in front of an air return. IBAC #4 was positioned on a small stand about 0.3 meters off the floor and about 0.3 meters away from the air return to allow for sufficient airflow around it. Prior to PSL release and in between each test type, baseline measurements were collected in the BCU by the IBAC sensors for 10 to 20 minutes; this was done to ensure there were no residual PSLs in the BCU before conducting a new trial. Following each PSL release, the airborne concentration of PSLs was measured by the IBACs every second for 30 minutes. Thirty minutes permitted clearance of the aerosolized PSLs as observed by the IBAC sensors.
Simulated Cough Scenarios and Healthcare Worker Activities
After discussions with the faculty and staff of the BCU, 3 likely BCU scenarios were identified and run in the following order: (1) simulated patient care (5 minutes)—control run with no PSL; (2) static PSL release with no activity in patient room; (3) 5-minute healthcare worker patient care activity after standing in front of the coughing device to contaminate the healthcare worker with the PSL particles. Table 1 summarizes the test runs performed, the number of coughs performed for each test with the cough simulator, healthcare worker activities, and the total number of trials for each test type. A total of 15 test trial runs were performed across the 3 test types.
Summary of Tests Performed in the Biocontainment Unit (BCU)
Test type #3 represented a typical healthcare worker performing 5 minutes of patient care activities during and after a simulated 2-cough event during which the healthcare worker's PPE was directly contaminated by the released PSLs (ie, a simulation of the healthcare worker being coughed on by the patient). Since certain non-PSL particles, such as bioaerosols and clothing particles, may also be detected as fluorescent particles by the IBACs, test type #1 served as a control experiment. In test type #1, sterile, filtered, deionized water was aerosolized from the cough simulator without PSLs. The healthcare worker entered the patient room through the donning area, performed the same 5 minutes of simulated patient care activities as assessed in test type #3, including the entire PPE doffing procedure. The background level of fluorescent particles measured by each of the 7 IBACs during all trials of test type #1 were averaged together (ie, IBAC location specific averages) and then subtracted from each of the same IBAC's average cumulative particle counts for test type #3. This ensured that the cumulative counts of fluorescent particles measured by the IBACs during test type #3 would represent only the released PSLs. The full PPE doffing procedure can be found in the supplementary material (http://online.lie3bertpub.com/doi/suppl/10.1089/hs.2017.0064/suppl_file/Supp_Appendix1.pdf).
Test type #2 was a static test in which PSLs were released without any healthcare worker activities. This provided an assessment of the concentration of fluorescent particles directly attributable to the cough machine, as well as the aerosol dispersion characteristics inherent in the BCU patient room without human interference. The healthcare workers who participated in this study were fully trained BCU clinical staff who would normally provide patient care in the isolation unit. Donning and doffing of PPE was performed according to BCU protocols (see Supplementary Material). There were no fluorescent particles detected in the BCU by the IBACs prior to the beginning of this experiment, and the 30-minute duration of each test was found to be sufficient for clearance of PSLs from the BCU.
Results
Figure 2 shows the average cumulative fluorescent particle counts (mean ±1 SD) measured by each IBAC sensor throughout the BCU across the test types. For all tests, there were no PSLs detected by the IBACs in the donning room. During the static test runs in which PSLs were released without any healthcare worker activities (test type #2), there were no PSLs detected in the doffing room. In the absence of healthcare workers, these results indicate sufficient isolation as established by the airflows and door barriers of the contaminated patient room space from the donning and doffing rooms. For test type #2, the highest average cumulative PSL counts were recorded by the IBAC in the center of the patient room (IBAC #3), while the other IBACs throughout the patient room recorded similar PSL counts that were approximately half the value in the center of the room. This suggests quick and uniform mixing of the air in the patient room with some particle accumulation near the center of the room; this was likely caused by the expulsion of the PSLs from the coughing device into the area of the patient room near IBAC #3. If this is the case, then it should be noted that the PSLs were expelled into the center of the room and past the foot of the bed where an air return (intake) was located (at IBAC #4).
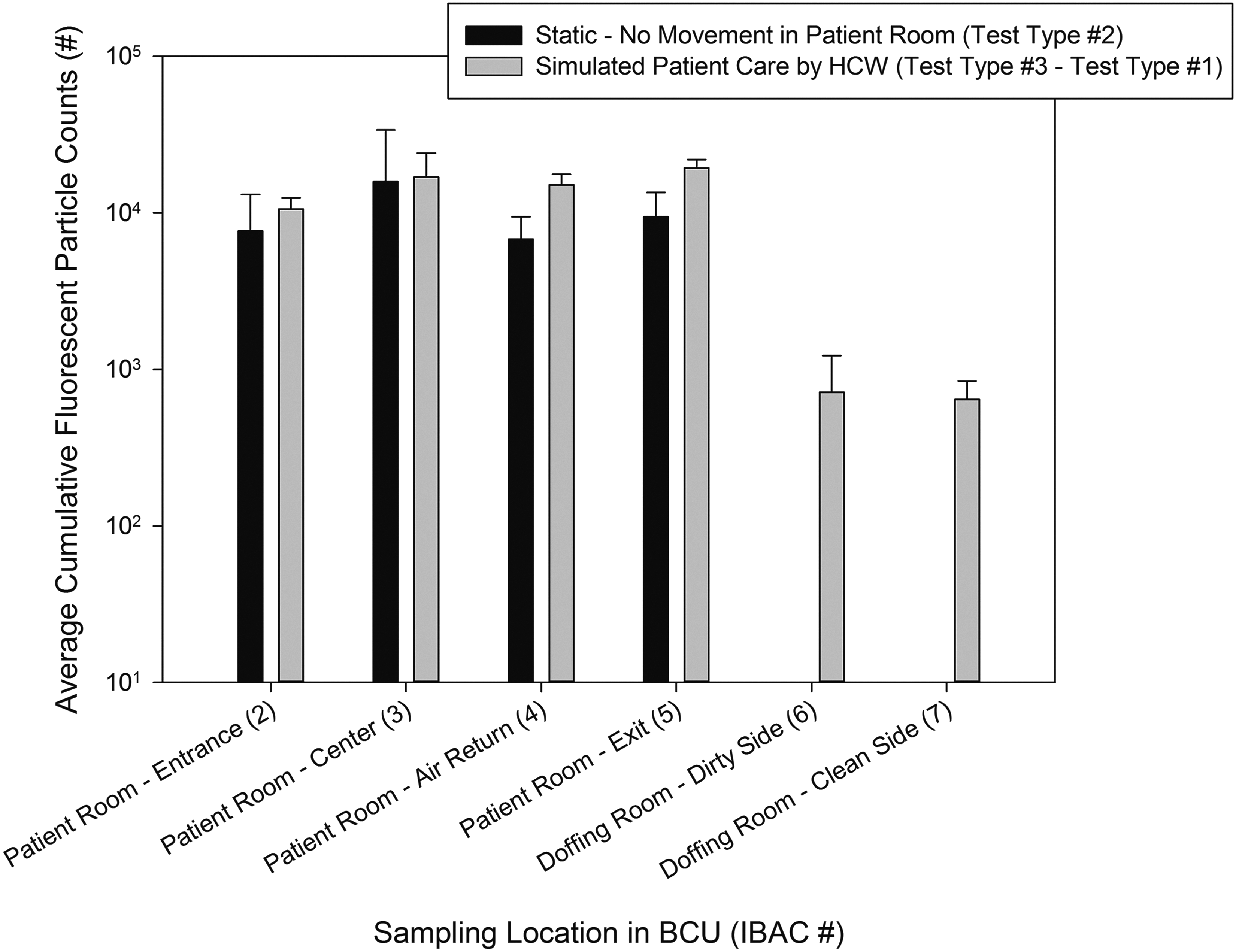
Cumulative Fluorescent Particle Counts (cumulative PSL number averaged across repeat trials of the same type ±1SD) measured by each IBAC across the test types. The IBAC numbers coordinate with their locations throughout the BCU as described in Figure 1. The black bars represent test type #2 (n = 8) for which PSLs were released into the patient room without any healthcare worker activity in the room. The grey bars represent test type #3 (n = 3) where PSLs were released into the patient room while the healthcare worker stood in front of the coughing device followed by 5 minutes of healthcare worker simulated patient care activities. Test type #3 was corrected for background fluorescent particles by subtracting the IBAC averages for test type #1 (n = 4, 5-min healthcare worker activity control run with no PSLs released). An IBAC sensor placed in the donning room detected no particles throughout our experiments.
For test type #3 (Figure 2), the average cumulative PSL counts recorded by the IBACs were more uniform throughout the patient room as compared to test type #2. This indicates that the addition of the healthcare worker's movement in the patient room increased mixing of the air, resulting in increased dispersion and mixing of the released PSL particles. As in test type #2, there were no PSLs detected in the donning room. However, in contrast to test type #2, there were PSLs detected on both the clean and dirty sides of the doffing room space. These PSLs may have been present in the doffing room because of the opening of the patient room door, resulting in transport of the PSLs from the patient room into the doffing room. However, this seems unlikely because of the airflow pattern of the BCU, which maintains the patient care rooms at negative pressure (at least −0.2 wg) compared to the donning and doffing rooms at an air exchange rate of 12-15 changes per hour. 21 It is possible that the movement of the healthcare worker from the room and/or the opening of the doffing room door overcame the negative pressure between the patient room and doffing room spaces. It is more likely that the PSLs observed in the doffing room were re-aerosolized while the healthcare worker doffed his or her PPE. Further research to differentiate the particle movement as a result of opening and closing doors from healthcare worker movement could provide additional evidence for protocol development and facility design.
The average cumulative particle counts detected by the IBACs during test type #1 were 5% or less of the values recorded during test type #3. Regardless, the average IBAC values of the control trials (test type #1) were subtracted from the IBAC values of test type #3 to ensure that any fluorescent particles detected were the PSLs. The average number of PSLs measured on the dirty and clean sides of the doffing room were similar, which suggests uniform mixing of the air in the doffing room space. This suggests that the “clean” side of the doffing room may not necessarily be clean, depending on the presence of airborne particles in the room.
Discussion
These results demonstrate the critical need to better understand the safety implications of protocols used in BCUs, including each step in PPE donning and doffing and patient care. Releasing PSLs and tracking their transport by fluorescent particle counters may identify potential pathogen exposures for healthcare workers and can inform recommendations to mitigate risk.
As expected, the air handling system of the BCU contains particles in the patient room under static conditions. However, during patient care, potentially infectious particles are introduced into the doffing area, possibly by re-aerosolization during the PPE doffing process or by opening of the patient room door. The number of particles and amount of re-aerosolization depends in part on the activities of the healthcare worker and the patient prior to doffing, and on the doffing procedures themselves. This information can inform changes in protocols that can be empirically tested to further minimize the risk of healthcare worker exposure. For example, in the Johns Hopkins doffing procedures, healthcare workers could undergo a wipe-down procedure in the patient care room prior to exiting to the doffing room to reduce the number of particles re-aerosolized during the doffing process. The powered air-purifying respirator (PAPR) hood could be left in place until the final step in the doffing process, or an N-95 respirator could be donned to maintain protection from aerosolized pathogens while removing shoe covers. Lessons learned are also applicable to other areas in the hospital where infection control is paramount, such as intensive care units (ICUs) and areas with possible transmission of antibiotic-resistant microorganisms.
Limitations and Future Research Directions
In this pilot study, there are some limitations to our findings. First, we used only 1 size particle, which affects generalizability to a broad spectrum of infectious agents and how they behave while airborne. Second, the use of the cough simulator may have improved the practicality and applicability of this research for studying simulant pathogen particles released from a patient with a respiratory disease. However, this method for particle aerosolization may not be applicable to nonrespiratory diseases, including EVD. Third, the increase in PSL counts in the patient room during test type #3 as compared to test type #2 requires further investigation, as this may have been caused by re-aerosolization of PSLs from the floor where the healthcare worker walked. Foot traffic has been previously identified as an important mechanism for resuspension of settled bioaerosol particles, including bacteria and fungi, from flooring materials. 33 While we did wait between trials for the air to be cleared of released PSLs as indicated by the IBACs, it is likely that any of the larger PSL agglomerates that were not removed by the air handling system were deposited onto the floor. A few trials of test type #3 were performed after wiping the floors in front of the coughing device and applying a floor covering. During these trials, a decrease in the measured cumulative number of PSLs was observed as compared to the other trials that included healthcare worker activities (data not shown). Additionally, other fluorescent particles from biological materials or clothing in the hospital setting may have been present during our studies.34,35 However, personnel on the unit were kept at a minimum (only study participants), and background fluorescent counts were subtracted from total counts.
Next steps will be to repeat experiments using a systematic approach required for validation and broader applicability of methods. Future research will perform the same series of experiments in the BCU using a range of particle sizes (1-10 μm) representing different viral, bacterial, and fungal pathogens, 33 labeled particles, 36 and several different particle nebulizers representing different pathogen dispersion methods, including the cough simulator, a Collison Nebulizer, and a PFA Concentric Nebulizer (C-Flow, Savillex Corporation, Eden Prairie, MN). These experiments will also be performed with a floor wiping and/or covering method included between trials to investigate PSL resuspension from the floor while the healthcare worker walks. This is an important factor to isolate since the gown of the healthcare worker's PPE is open on the bottom, potentially leaving the healthcare worker vulnerable to particles resuspended from the floor. As many patient stays in BCUs exceeded 2 weeks during the Ebola outbreak, it is important to understand the life cycle and fate of these particles, and potentially to address cleaning or other unit procedures appropriately. This methodology can be deployed during a live-action drill in the BCU to better understand particle dissemination and fate in an actual patient care environment. Also, while the IBACs provided cumulative particle counts for the fluorescent PSLs, future tests will also include aerosol instrumentation to measure particle size distributions produced by the nebulizers. Different particle nebulizers produce a range of particle sizes, including different size distributions of agglomerated liquid suspension. 37
Finally, it is important to note that PSL particle detection is not indicative of exposure or transmission. Follow-on experiments will further investigate the potential for re-aerosolization of particles from PPE during doffing by evaluating the number of resuspended particles observed under controlled laboratory conditions. These tests will include swabbing the inside of the healthcare worker's PPE and sampling for particles in the healthcare worker's breathing zone throughout the doffing procedure. Follow-on experiments will also include investigation of the BCU's isolation efficiency under different simulated scenarios of air handling unit failure, including evaluation of particle transport throughout the BCU in comparison to airflow and measured air pressures.
Conclusion
Overall, this study provides the foundation for developing a systematic method to evaluate potential airborne pathogen exposure pathways for healthcare workers in a BCU. The ultimate goal is to develop standardized BCU safety protocols and to identify areas of potential risk across different BCU facilities, PPE donning and doffing procedures, air handling systems, and patient care protocols. It may also provide a safe and effective method for identifying the areas of highest risk in complicated doffing procedures. It will also give healthcare workers valuable data about the safety provided by the built environment and infrastructure of the BCU. These preliminary data and this method will increase healthcare worker and healthcare system safety, mitigate healthcare worker fears about the risk of treating patients with highly infectious diseases, and raise the overall quality of care for patients in high-containment environments. 38
Footnotes
Acknowledgments
We would like to acknowledge Dr. Lisa Maragakis, Senior Director of Infection Prevention, Johns Hopkins Health System, and her Hospital Epidemiology and Infection Control team for their guidance and expertise; Gregory Bova, the lead engineer who designed the air handling system of the BCU; Mallory Reimers, the nurse educator for the BCU, who performed the healthcare worker walkthroughs and patient care simulations; and F. Connor Sage, who assisted in the aerosol experiments on the BCU. We would also like to thank the staff of the Johns Hopkins BCU who helped in the BCU design process and in the creation of patient care protocols. The National Health Mission Area at the Johns Hopkins University Applied Physics Laboratory provided funding for this study as part of an internal research and development project.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.