
Abstract
The objective of this work was to examine the spread of the Zika virus after the destructive impact of the earthquake of April 2016 along the coast of Ecuador. Using a difference-in-difference estimation method and a unique dataset to track Zika cases at the national level, we estimated the impact of the earthquake on the reported cases of Zika in the affected region. Our results suggest that the earthquake increased the reported cases of Zika by 0.509 per epidemiologic week (data per 10,000 population), and we argue that the destroyed built environment along with other factors created a disease focus, where the virus spread easily. Because of its potential complications and devastating long-term effects, Zika represents a national threat. After a natural disaster, the health authorities, together with a multidisciplinary team and the wider community, all have an urgent responsibility to collaborate to minimize the health risks to the population.
The authors examined the spread of the Zika virus after the destructive impact of the earthquake of April 2016 along the coast of Ecuador. Their results suggest that the earthquake increased the reported cases of Zika by 0.509 per epidemiologic week (data per 10,000 population). The destroyed built environment, along with other factors, created a disease focus, where the virus spread easily.
A
The concern about Zika virus goes beyond disease control. The potential correlation of the virus with other long-term health conditions has raised awareness of the need to manage the virus as a public health concern. In October 2015, the Brazilian Ministry of Health reported 26 cases of microcephaly in newborns, which had possibly been caused by Zika virus infection in the mothers while they were pregnant. This added to the large amount of evidence that implies a causal relationship between prenatal Zika virus and this type of genetic alteration, among other severe brain anomalies.3-5
Between April and November 2015, several cases of congenital malformations—including placental insufficiency, intrauterine growth retardation, and fetal death—were associated with Zika virus infections.4-6 In addition, there is growing evidence of a causal association between Zika virus and Guillain-Barré syndrome (GBS), which may require intensive care due to respiratory complications, cardiac arrhythmias, or arterial pressure changes.7-10 In this context, Zika virus infection creates an extra vulnerability for certain groups of the population—mainly pregnant women, but also for children and elderly people whose health conditions or the preexistence of other diseases, such as GBS, could present severe problems during a Zika virus infection. 10
The first imported cases of Zika virus in Ecuador were reported in December 2015. 11 The ministry of health warned the population about the possible health problems from the virus transmission, the routes of transmission, the potential adverse effects, and the recommended control measures. However, despite these efforts, several Zika virus cases were detected in the coastal, Amazonian, and interior regions of the country. These regions have specific meteorological and geographical conditions that are conducive to mosquitoes (Aedes aegypti) living and reproducing. 8
On April 16, 2016, an earthquake of magnitude 7.8 occurred along the coast of Ecuador, severely affecting many towns in the provinces of Esmeraldas, Manabí, and Guayas. Hundreds of people died and thousands suffered some type of injury. The most affected cities were located in the province of Manabí, which accounted for over 75% of total casualties. 12 During the earthquake, many buildings collapsed leaving no time for evacuation. Many cities remained blocked by road damage for several days. The built environment of the affected areas became chaotic, and the disaster zone had tons of debris, plastic, cans, pots, containers, and toilets remaining in the open. Although the health authorities activated disease surveillance and control actions, the area became the ideal scenario for breeding sites for Zika virus vectors. 13
After the earthquake, the authorities declared a state of emergency and began taking action to rescue people and provide shelter. Nevertheless, national and international aid was delayed. During the first days after the disaster, thousands of families remained outdoors, some because there were not enough places in the shelters, and many others because they felt safer in open spaces. In the following days, 20 extra shelters were installed in some cities, with capacity for 1,500 people. 14
The first services to be provided after the earthquake were food and running water. However, other urgent needs, such as garbage collection, were unavailable until much later because of road damage and the presence of debris. Over time, the accumulation of trash and plastic bottles was conducive to the accumulation of water, and, therefore, there were more breeding sites for Zika virus vectors. Once the authorities detected this problem, people in the area were warned about it through social media and newspapers. 15
We looked at the Zika virus outbreak in Ecuador after the earthquake of April 2016, and the conditions that we describe here show that, after a natural disaster, people are not only vulnerable to the direct effects caused by the destruction of the built environment but they are also in danger of indirect health threats, such as disease outbreaks, depending on their social, cultural, and economic conditions. This article addresses the global impact of the earthquake on the cases of Zika and the persistence of the earthquake's effects over time. In fact, given the climatic conditions of the affected areas, it is possible to isolate the effect of the earthquake and to estimate its impact on the number of diagnosed Zika virus cases.
From a risk management perspective, we are able to show that the Ecuadorian experience after the earthquake should remain a topic of special attention, especially because of the potential long-term health effects on people diagnosed with Zika virus. This situation reinforces the need for disaster risk management strategies to become more interdisciplinary, inclusive, and attached to the local circumstances of places where a natural phenomenon, such as an earthquake, takes place, preventing them from becoming real disasters.
Methods
Data
The data that we included in the analysis were taken from the Zika virus cases reported in 2016 to the epidemiological surveillance system SIVE-Alert of the Ministry of Public Health of Ecuador (MSP). The information was reported for each epidemiologic week by all health facilities of the MSP. In some districts, the information was also obtained from public and complementary network facilities. Some cases were diagnosed with a reverse transcriptase polymerase chain reaction (RT-qPCR) test that was run by the national reference laboratory, which is part of the National Institute of Public Health Research. Meanwhile, other cases were diagnosed by epidemiologic link, which we defined as cases that did not have laboratory tests but which met clinical criteria, with patients coming from geographical areas where viral circulation was verified by the presence of other cases diagnosed by laboratory tests.
Statistical Model
Zika virus is primarily transmitted through the bites of mosquitoes that live in tropical, subtropical, and in some temperate climates. Therefore, to estimate the effect of the earthquake, we focused on zones in the coastal part of Ecuador that had comparable weather and geographical conditions.
As compared to similar studies, which estimated the odds ratio and the cumulated incidence of Zika virus infection after the earthquake, 16 we quantified the global impact of the earthquake on the number of diagnosed cases and adjusted for population per epidemiological week and for the persistence of the effects over time. Given the geographical localization of the country, Ecuador is an interesting case for analysis because the weather within regions varies slightly over the year. From the perspective of the implemented methodology, the estimation of a causal impact is feasible if the exogenous conditions between comparison groups and over time (before and after the earthquake) are the same. The earthquake serves as a natural experiment, where the “event” happened at random, while other exogenous variables stayed constant.
For the analysis, we included information from 5 provinces located in the coastal region: El Oro, Esmeraldas, Guayas, Los Rios, and Manabí. The data were divided into 2 groups, one known as the “disaster zone” and the second known as the “control zone.” The epicenter of the earthquake was located in the city of Pedernales, in the province of Manabí. Thus, this province was categorized as the disaster zone, and the remaining provinces were included in the control zone. More than 97% of the reported casualties (number of deaths after the earthquake) were reported in the province of Manabí. 17 In contrast, in provinces such as Guayas and Esmeraldas that were also affected by the earthquake, the number of reported deaths and displaced people was rather small.
Using a difference-in-difference (DID) method, we estimated the effect of the earthquake on the number of diagnosed cases of Zika virus (Table 1). The equation computes the impact of the earthquake by comparing the situation between affected provinces (disaster zone) with provinces of similar characteristics (control zone) before and after the earthquake.
Difference-in-Difference (DID) Estimator
In formal terms:
where
The coefficient of interest in Equation 1 is given by
An important assumption of the DID estimation is the parallel trend between the comparison groups before the earthquake. More specifically, for the zones in analysis to be comparable, the disaster zones and the control zones should have had similar conditions before the earthquake. Therefore, to claim a causal relationship, the only difference between the 2 zones, ideally, should be the earthquake. To check this assumption, we use a weighted regression that estimates the average number of diagnosed cases (smoothed patterns) by epidemiologic week before and after the earthquake for both groups.
Nonlinear Impact
The DID equation estimates the average impact of the earthquake from mid-April 2016 to December 2016. Nevertheless, immediately after the earthquake in Ecuador, the risk of infection was at its highest due to the scarcity of public services—such as garbage collection and the provision of running water—which, combined with the large amounts of rubble from the collapsed buildings, created mosquito breeding sites. Over time, however, as the conditions improved—such as the opening of shelters, the provision of basic services, the availability of food and medicine, and access to medical assistance—it is expected that the number of people infected would decrease. More specifically, we would expect that the effect of the earthquake follows a nonlinear trajectory, initially showing an explosion of cases, but, over time, the effect would decrease, until it vanishes.
Therefore, to estimate the evolution of the impact of the earthquake, we use an alternative version of Equation 1, where the interaction term
where
Results
Descriptive Statistics
The data were divided between 2 comparison groups: the disaster zone and the control zone. Both zones are located in the coastal region of Ecuador, with similar weather and altitude. While the disaster zone corresponds to the earthquake epicenter (province of Manabí), the control zone is composed of 4 provinces (El Oro, Los Rios, Guayas, and Esmeraldas) (see Figure 1).

Ecuadorian Provinces Included in the Study
On average, during 2016, data show that the number of diagnosed Zika virus cases in Manabí was much higher than in all the other provinces (see Table 2). Compared to Esmeraldas, for example, Manabí had almost 9 times more diagnosed cases of Zika virus in a week, a result that holds even after adjusting for the population size. Furthermore, if we compare the situation before and after the earthquake, it is possible to see that before the earthquake the province of Manabí already had a higher incidence of Zika virus. However, this difference explodes after the earthquake. Because the population significantly varies from province to province, the statistical analysis adjusted the diagnosed cases by population size. Therefore, the reported numbers in the results section are per 10,000 people.
Diagnosed Cases of Zika in 2016. Summary Statistics
Note: Standard deviations in parentheses.
Diagnosed cases (mean) before and after the earthquake.
The population numbers were retrieved from the latest census available (2010).
Source: Ministerio de Salud Publica (MSP).
Figures 2 and 3 show the evolution of the frequency of Zika virus cases per month during 2016. When analyzing the data by subgroups, from the total diagnosed cases, the numbers show that most of them correspond to women, of whom few are pregnant (Figure 2). The graph by age group indicates that individuals between 18 and 35 years old were the most affected (Figure 3). If we put these 2 graphs together, it suggests that there is a potential bias in the sample toward young women. In fact, because pregnant women could have the worst consequences from Zika virus, women of fertile age are more likely to visit a health facility to get tested.
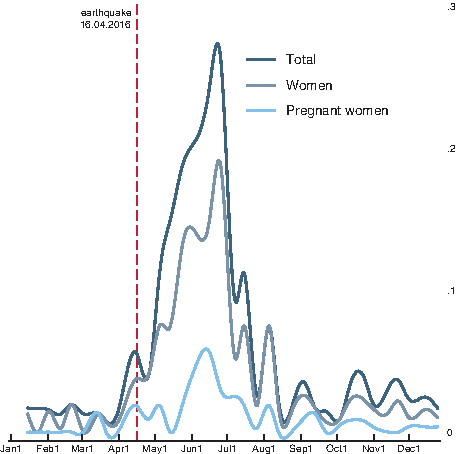
Diagnosed ZIKA Cases (per 10,000 people)
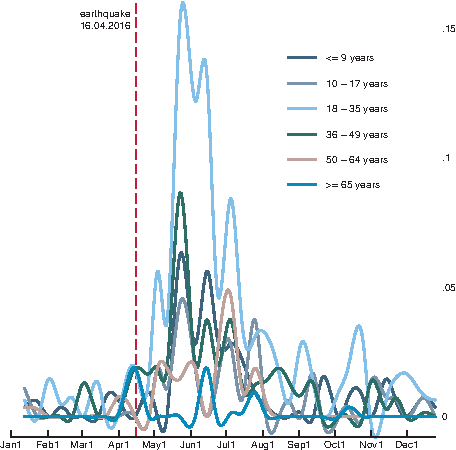
Diagnosed ZIKA Cases by Age Group (per 10,000 people)
Statistical Analysis
Table 3 reports the results for Equation 1. The dependent variable is the number of diagnosed Zika virus cases per 10,000 people by epi-week in the year 2016. Only the coefficients of interests are reported in this table. The first 2 variables in the model estimate (1) the differences between the disaster and control zones (
Estimation Results DID Regression (dependent variable: diagnosed cases of Zika by epi-week, per 10,000 people)
p < 0.05, **p < 0.01, ***p < 0.001. Robust standard errors in parentheses.
More specifically, the model estimates that the earthquake is responsible for an increase in the diagnosed cases of Zika virus by 0.509 in the total population, 0.352 among women, and 0.034 among pregnant women. Given the population size of Manabí (1,369,481 people), this estimate implies that the earthquake is responsible for nearly 70 new infected people per epi-week, of whom 48 are women and 5 are pregnant women.
This result should be taken with caution because it is an average estimate of the reported cases after the earthquake, which includes the period from April to December. From the descriptive statistics section (Figure 3), it is possible to see an explosion of Zika virus cases just after the earthquake. Over time, however, the number of cases decreases dramatically. This trajectory suggests that the earthquake had a nonlinear impact, where the strongest impact took place just after the earthquake, and it slowly vanished over time.
By desegregating the effect of the earthquake over time, it is possible to estimate the number of weeks until the earthquake had an effect on the number of diagnosed cases of Zika virus. Because the estimation uses data by epi-week, the results are reported month by month, starting from t + 0.5, which is 2 weeks after the earthquake.
As expected, the impact of the earthquake has a nonlinear pattern (Figure 4), where there is a significant increase in the cases of Zika virus from April until August (t + 4). The first 3 instances (2 weeks after, May, and June) after the earthquake had an increasing growth rate of Zika virus cases. From July until August, the growth rate, even when positive, decreased. From September, the effect of the earthquake on the cases of Zika virus seemed to have disappeared.
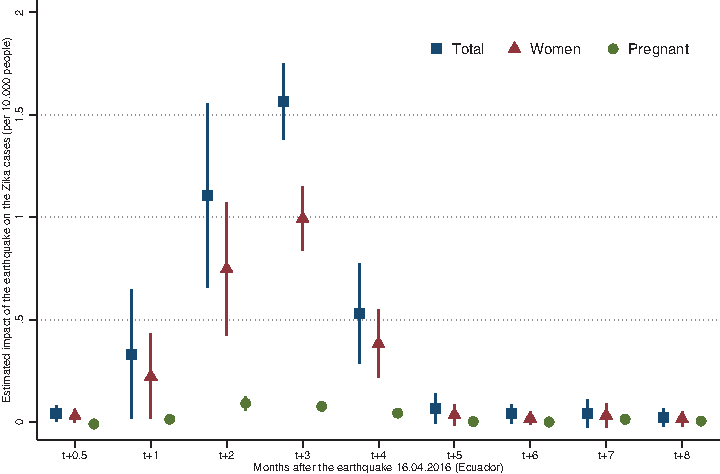
Impact of the Earthquake Over Time
Parallel Assumption
Finally, as detailed in the methodology section, the DID model assumes that the 2 comparison groups had similar trends before the earthquake. Figure 5 shows the diagnosed cases of Zika virus over time. The figure describes the evolution of the diagnosed Zika virus cases during 2016 for the disaster and control zones. The figure shows that the 2 zones had similar behavior before April 2016. Even when Manabí, or the disaster zone, consistently showed a higher number of diagnosed cases before the earthquake, the trend accords with the trend in the comparison zones. The diagnosed cases only exploded in the disaster zone after the earthquake.
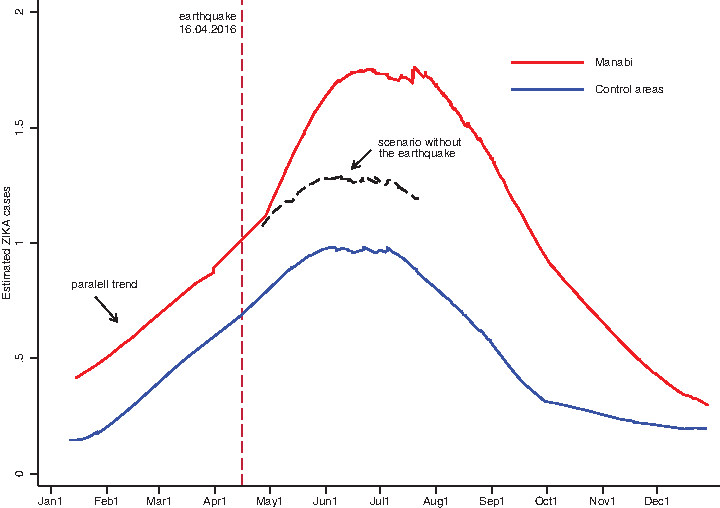
Difference-in-Difference (DID) Parallel Assumption Graphic Check
Discussion
We evaluated the aftereffects of the earthquake in Ecuador in April 2016, as measured by the diagnosed cases of Zika virus. Our estimates suggest that the earthquake is responsible for about 70 new cases per epi-week in the disaster zone and that women were affected the most. The effect was persistent up to 4 months after the earthquake.
In contrast with the related literature that focuses on developed countries, where most results show no danger of epidemics of infectious diseases after a natural phenomenon, 18 studies in developing countries estimate serious disease outbreaks—not only because of the direct destructive power of a disaster but also because of the negative spillover it generates in other infectious diseases. 19 Examples include the earthquake in Costa Rica in 1991, which was associated with a significant rise in malaria cases. 20 Following the 2005 earthquake, Pakistan had a significant increase in cases of tetanus, hepatitis E, and diarrhea. 21 Many studies in Asia have shown that disasters resulting from floods, earthquakes, or typhoons have a strong impact on the incidence of communicable diseases. 22
In the specific case of Zika virus, studies analyzing the effect of natural disasters have mainly focused on the case of Ecuador because there are not many other comparable events. More specifically, related articles show that, after the earthquake, there were many more people with Zika virus symptoms in the affected areas, with the most vulnerable people being between 40 and 64 years of age and people who had no place to sleep. 23 Some studies show that the earthquake, in fact, explains a significant increase in the cumulative incidence of Zika virus and in the odds-ratio of infection for people living in the affected areas. 16 An article that is closer to ours, 23 aside from the incidence, also analyzes the effect of the earthquake on the Zika virus trend. Even when the results are comparable to ours, the methodologies are different. Our article gives global estimates of the effect of the earthquake on the diagnosed cases of Zika virus, controlling for population size and province characteristics, and it also estimates the evolution of the impact over time.
Our perspective is that the Zika virus outbreak and the 2016 disaster in Ecuador can most plausibly be explained by the interactions among the earthquake, the ineffective risk reduction strategies, and the physical, social, and cultural conditions of the affected areas. The collapse of the built environment, which forced people to remain outside, exposed them to a chaotic urban space full of debris and industrial waste (eg, plastic bottles), it blocked garbage collection, and it left them without drinking water. In addition, as shown by some articles, access to medical treatment was significantly delayed because of the earthquake. Most people either were on long waiting lists or they had to travel to neighboring provinces to seek medical attention. 16 Traveling was also very complicated because of road damage, rubble blocking streets, and the closing off of the affected areas to prevent looting. This situation was made worse by the problem of waste accumulation and limited the entry of health practitioners to the disaster zone.
As discussed in the literature, disaster risk management should be addressed with a multidisciplinary approach, starting before an event like an earthquake happens. 24 A natural phenomenon needs to be understood as a moment that has a huge potential to affect the physical, social, economic, and health conditions of the population, where not only health professionals are required, but also many other sectors and actors from society need to work in coordination.
The absence of local capacity, and a lack of understanding of shared responsibility among public entities, private entities, and the community, decrease the options to reduce the risks associated with these events. Working directly with the community has been found to be an effective way of reducing risks.25,26 Successful experience has shown that aftereffects can be reduced when communities are involved. In Bangladesh, for example, a mixture of data collection and the knowledge of previous experiences that drew on existing social capital helped the community to develop its own protective measures according to its resources.27,28
After the lessons from the earthquake in Ecuador, the authorities, together with the community, should develop a deeper understanding of the relationship among natural phenomena, the built environment, and the local characteristics of the area where an event of this nature can take place.29,30 It is crucial to develop risk assessments within specific cultural, social, economic, and territorial contexts, identifying risks and the resources available to reduce them. 31
From a policymaking perspective, epidemics must remain a main topic of study after a disaster. The probabilities of disease outbreaks in certain contexts, such as those of the earthquake in Ecuador, should be calculated to establish risk management priorities and to allocate resources efficiently. 25 After a natural disaster, the very first steps to follow include improving sanitary conditions and providing shelter to reduce the time that the affected areas are a disease focus.
The time needed from the earthquake to providing assistance to the affected population is a key element to analyze, design, and implement public health policies. The results obtained by the estimate in this article show that the impact of the earthquake on the Zika virus outbreak lasted for about 4 months. Our conclusion is that this risk was not clearly identified in that time and that the interactions between the earthquake and the local conditions of the affected cities exceeded the community's capacity to adjust, protect, and provide fast health and emergency medical relief.1,2,32
To further assess the health risks associated with the earthquake, it is important to inquire into the different circumstances in which people stayed during the daytime and nighttime in unplanned shelters and in open spaces near the rubble. Understanding of temperature and humidity shifts during the day and night could also help to develop contingency strategies, especially for places with weather conditions like those of the Ecuadorian coast.
The health and risk management authorities should deepen their analysis of the specific needs of highly vulnerable groups (eg, children, pregnant women, elderly people, and people with disabilities), not only to prevent further complications of their health but also to prevent additional fatalities or lifelong long-term disabilities. For example, it would be necessary to understand the conditions that led to increased infections in women compared to men and for children and older individuals.33,34
Finally, it is very important to deepen the analysis of the epidemiologic changes in Ecuador after the earthquake, not only for Zika virus infection but also for other diseases such as dengue fever and chikungunya, which are transmitted by the same mosquito. 35 To prepare the population for similar situations, it is insufficient to work on a rapid disease risk assessment by public health responders right after the phenomenon. 19 We emphasize the needs described in this work, which encompass a multidisciplinary approach, the coordination among actors, and working more closely with the community in order to improve risk management efforts to reduce potential outbreaks and their effects over time.
Footnotes
Acknowledgments
We appreciate the data provided by the Ecuadorian Ministry of Public Health for this study.