
Abstract
Emerging disease threats like Zika pose a risk to naïve populations. In comparison to chronic diseases, there is scientific uncertainty surrounding emerging diseases because of the lack of medical and public health information available as the threat emerges. Further complicating this are the multiple, diverse channels through which people get information. This article used bivariate and multivariate analysis to first describe the breadth of information sources individuals accessed about the Zika virus, and then describe individuals' primary sources of information for Zika using a nationally representative pooled cross-sectional data set collected at 3 time points in 2016 (N = 3,698). The analysis also highlights how 3 subgroups—high-education, high-income adults; Hispanic women of childbearing age; and retirees over the age of 65 with less than a high school education—varied in their use of information. Results suggest individuals accessed multiple sources, but TV and radio were the primary sources of Zika information for the public, followed by print news. Demographic variation in primary source of information means public health officials should consider alternative channels to reach target groups in an emerging event. Without an understanding of how information has reached people, and who individuals engaged with regarding that information, public health practitioners are missing a key piece of the puzzle to improving public health campaigns during a future event like Zika. This analysis aims to inform the public health community about the message channels the US population uses during an emerging disease event and the most prevalent channels for different demographic groups, who can be targeted with particular messaging.
This article describes the breadth of information sources individuals accessed about the Zika virus and their primary sources of information for Zika using a nationally representative pooled cross-sectional data set collected at 3 time points in 2016 (N = 3,698). The analysis also highlights how 3 subgroups—high-education, high-income adults; Hispanic women of childbearing age; and retirees over the age of 65 with less than a high school education—varied in their use of information. Results suggest individuals accessed multiple sources, but TV and radio were the primary sources of Zika information for the public, followed by print news.
P
Communicating in public health emergencies presents unique challenges. Compared to chronic health issues, the scientific uncertainty during emerging diseases, attributable to the lack of medical and public health information available as the threat emerges, makes message content vary.6,7 Emerging disease communication typically must convey the best public health information available at the time, in a fluid situation.4,5,8 This is especially a concern when the information being communicated is time sensitive, such as the need to take preventive measures before an outbreak becomes localized.
Further complicating communication in a public health emergency is the speed with which the public can get access to information. While mass media have historically played a role in the distribution of health information, the rise of social media has added a channel for rapid message distribution.9-11 The percent of the population using social media has expanded exponentially in the past decade and is continuing to grow, especially among older adults.3,12 Social media have particularly grown as a means of health communication, doubling as a vehicle for health information from 2001 to 2011. 12 While social media allow for quicker distribution during an emerging threat, this speed, in conjunction with a lack of content monitoring, can also compromise the accuracy of health information. 13
There are a multitude of channels individuals can turn to for information during an emerging disease event, 14 including government websites; traditional media, such as print news, television, and radio; in-person resources (eg, physicians, family, friends); and digital media that can be searched and redistributed through online news portals and social media. 15 The advent of social media means the public is constantly able to access information during rapidly evolving events. Factors commonly found to influence where individuals turn for information include credibility, trust, and familiarity with the channel.16-18 Recognizing the communication challenges that develop during an emerging disease event, and the diversity of message channels used, it is important to understand how diverse populations, especially those most at risk, access information during an emerging disease outbreak, so public health officials can communicate most effectively with those most vulnerable to the emerging threat.
The Zika virus provides the latest example of a need for public health information to be distributed to the public about an emerging disease. In the current outbreak, which began in late 2015, Zika has been associated with microcephaly and other neurological defects among newborns in more than 20 countries.19-21 Limiting the spread and impact of Zika became a priority for many nations and sparked a variety of mitigation strategies in the United States, especially for women of childbearing age and those who were pregnant or trying to become pregnant (and their partners).20,22 Messages delivered through a variety of channels focused on mitigation strategies, such as delay of pregnancy, avoiding travel to Zika-affected areas, and a variety of vector control approaches including but not limited to aerial spraying or introduction of genetically modified mosquitoes.23-25 Public health officials in the United States also particularly encouraged at-risk individuals to speak with their physician for further information. 26 The people at highest risk were pregnant women, women of childbearing age, and their partners.22,27 In some areas, such as New York City, there was a particular focus on Hispanic women as a vulnerable group, because of the endemic areas in which Zika spread and the connection local communities have with places like Puerto Rico, the Dominican Republic, and parts of Central and South America.1,20,28
Existing work on communication during the Zika virus event has focused on the role of social media in distributing information and misinformation to the public.29,30 Despite the current research focus on this particular channel of information for communication about Zika, research on the utility and efficacy of social media in emergency scenarios is inconclusive.31,32 Traditional channels of communication are still prominent and frequently used for official public health communication. Individuals have never been faced with so many channels of information—TV, radio, print news, their social network, social media, physicians, and other websites—during an emerging disease like Zika.
Thus, since people have multiple ways to access information, it is important for public health officials to understand the primary avenues different subgroups turn to for emerging health information. Understanding these factors can assist public health officials in designing more effective public information campaigns and targeting these campaigns through the most effective channels to specific groups. Using a repeat cross-sectional study representative of the US population over the course of 2016, this article identifies the channels of information the public used to gather information about Zika and explores the channels particular subsets of the population accessed for information.
In this article, we highlight how the use of particular sources of information varied based on different demographics, in particular age, income, race, and gender. We selected highly varying subgroups to illustrate differences in preferences for sources of information: Hispanic women of childbearing age, who were at particularly high risk for Zika; retired adults over 65 with less than a high school education; and highly educated working adults. These groups reflect possible market segments for communication purposes or key sources to target for risk communication. Hispanic women reflect those directly at risk, while the other 2 demographics reflect people who may serve as secondary influencers or information filters for those at risk, such as parents or partners. Identifying these channels, along with an exploration of how information sources for Zika are segmented, will allow public health professionals to better understand how to reach the public, especially particular at-risk populations, during an emerging disease threat.
Methods
Data Collection
Social Science Research Services (SSRS) collected nationally representative data using fully replicated, single-stage, random-digit-dialing sample households supplemented by a list of randomly generated cellphone numbers. Data were collected at 3 time points: spring (April/May), summer (July/August), and fall (October/November) of 2016. Surveys were conducted before local transmission of Zika in the United States (spring), following local transmission in early July 2016 (summer), and following the conclusion of US mosquito season (fall). The first structured telephone survey was of 1,233 US residents, and the subsequent surveys sampled 1,231 residents and 1,234 residents, respectively. The American Association for Public Opinion Research (AAPOR) response rate was approximately 4% at each wave, with an average number of 7 calls for completes, consistent with trends in representative survey research.33,34 The sample frame included an oversampling of women of childbearing age between the ages of 18 and 45 living in the southern tier states of Florida, Alabama, Mississippi, Louisiana, and Texas. Samples were weighted to be representative of the US population based on the March 2016 census supplement. Post-stratification iterative proportional fitting was used to balance the sample to known adult population parameters. Weighting procedures took into account the disproportionate probabilities of household and respondent selection due to the number of separate telephone landlines and cellphones answered by respondents and their households. Further details on sampling and weighting procedures have been previously described. 35
Measures
Dependent Variable
Respondents were asked to identify all information sources they accessed for information on Zika in the prior 2 weeks. Those who used any source of information were asked to identify their primary source of information, or they could indicate “don't know” or “not applicable.” The sources of information included: print news (publication accessed online or in hard copy); TV or radio news; social media, such as Facebook; a doctor; the government, such as the Centers for Disease Control and Prevention (CDC); or friends, family, or co-workers. Respondents could select only 1 primary source.
Independent Variables
Predictor variables included in this analysis were categorical variables for age (18-29, 30-45, 46-64 (ref), 65+), gender (male (ref), female), region (Gulf Coast (ref), mid-US, North), race (non-Hispanic white (ref), non-Hispanic black, Hispanic, other), household income (less than $25,000 (ref), $25,000-$49,999, $50,000-$99,999, more than $100,000), education (less than high school (ref), HS/GED, some college, 4-year college), political views (Republican (ref), Democrat, independent), health insurance status (does not have health insurance (ref), has health insurance), employment status (employed full or part-time (ref), retired, homemaker, currently unemployed), and point of data collection (April/May 2016 (ref), July/August 2016, October/November 2016). Variables were selected based on the author's interest in the way demographics relate to information sources accessed and to control for potential confounding.
Analysis Plan
This analysis explored the factors associated with the population's primary source of information about the Zika virus. Analyses were conducted by treating data as a pooled cross-sectional sample, with time included as a control variable, and therefore combined all 3 time points. Because there were not significant changes in the outcome variable over time, we elected to pool the cross-sectional data and control for time. This also allowed for an increased sample size, giving the sample more power. Independent variables were tested for concordance using correlation tests prior to bivariate analyses.
The research team first identified the average number of information sources and bivariable associations between demographics and number of sources used. We then conducted both bivariable analyses on demographics and each source of information and primary source of information. We also tested a multinomial logistic regression (mlogit, rrr) of predictors of primary source of information with the reference category as TV/radio or conventional broadcast media. TV/radio was selected as the reference category as it was the most common primary source, and we were interested in particular factors that would drive other sources to be primary.
The adjusted regression included all covariates in the model that were tested in bivariable analyses, based on bivariable results. While the bivariate analysis allowed us to examine each source independently for its relationship with covariates of interest, the purpose of the regression analysis was to control for confounders that cannot be examined in bivariate analysis. Because the dependent variable was a categorical, multinomial logistic regression was necessary.
Based on the results of the bivariable and multivariable analysis, in particular the relationship between demographic characteristics and primary source of information, and because of the relevance of understanding how to reach particular parts of the population, we examined particular demographic market segments of interest to risk communicators for the Zika virus, typically, and a common demographic group, which vary in their use of particular sources of information. Bivariable analyses were conducted on these demographic profiles using chi-squared tests.
Results
The US population gathered information about the Zika virus from multiple sources (Figure 1). An average of 2.4 sources were used by the US population for information about Zika; 7% of the population did not use any source for Zika information. Approximately 20.5% of the population used 1 source for Zika information; 28.8% used 2 sources; 21.5% used 3 sources; 13.1% used 4 sources; 6.1% used 5 sources; and 2.9% used 6 sources. Certain groups were significantly more likely to use multiple sources of information (data not shown), including young adults, those with incomes below $25,000, political independents, individuals living in the Gulf Coast region, and those with less than a high school education.
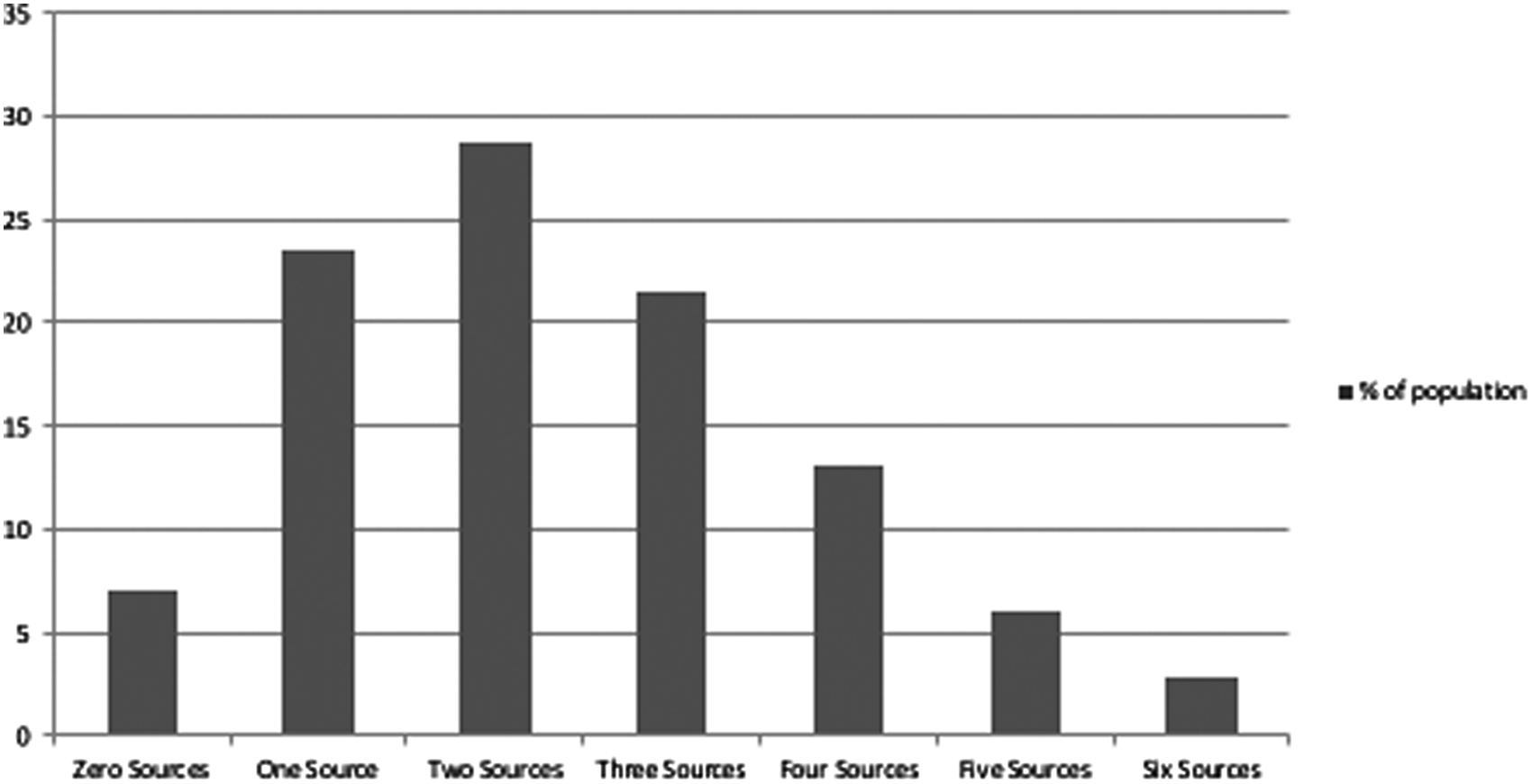
Distribution of Number of Sources Used for Zika Information Among the US Population
To identify the prevalence of using a source of information, regardless of whether it was the primary source, for various demographic groups, Table 1 presents the weighted bivariate associations between sociodemographic predictors and the use of each source for Zika information; it shows there are statistically significant differences in multiple demographics and sources of information.
Weighted Bivariate Associations Between Zika Source of Information and Demographics Among Those Aware of Zika (+/− 3 percentage points at the 95% confidence interval)
p < 0.05, **p < .01, ***p < .001
Table 2 presents bivariate associations between sociodemographic predictors and primary source of information. TV was the most likely primary source of information, while government sources were the least likely to be a primary source of information. There are statistically significant differences among all demographic predictors for primary source of information except for gender and region. The majority of older adults used TV or radio as their primary source of information (66.3%), while younger adults were more evenly distributed among print news, TV, and social media. Examining racial differences, the most notable differences are in print news, TV, and social media. Nearly 20% of Hispanics used social media as their primary source of information, compared to less than 10% of non-Hispanic whites, and there are similar discrepancies among various racial groups with other sources.
Weighted Bivariate Associations Between Zika Primary Source and Demographics
p < 0.05, **p < .01, ***p < .001
There is nearly a 30% difference among those in the highest income group (44.3%) and the lowest income group (16.9%) in the use of print or online news as a primary source of information. However, those in the lowest income group and with the lowest level of educational attainment were most likely to identify their doctor as a primary source of Zika information. A similar pattern emerged when comparing those in the lowest and the highest levels of educational attainment (15.4% vs 42.0%) with the lowest and highest income levels. Those with a 4-year college degree or more were least likely to identify TV as their primary source of information, compared to those in other categories of educational attainment.
Individuals without health insurance were more likely to use social media or friends as a primary source of information compared to those with health insurance. By employment status, retirees were most likely to use TV as their primary source of information (66.6%), as were homemakers (49.3%), while those who were currently employed were more evenly split between print news (27.5%) and TV (39.3%). Looking across time points, print news as a primary source of Zika information declined, while use of TV increased slightly, and there was little variation among other sources.
Table 3 examines the characteristics that increased the relative risk of a source being an individual's primary source of information compared to TV and radio in a multinomial logistic regression. Factors associated with an increased likelihood of using print news were younger age (RRR 3.93 [2.59, 5.96]; 1.53 [1.10, 2.14]), higher household income (1.77 [1.26, 2.58]; 1.96 [1.33, 2.90]; 2.69 [1.72, 4.25]), and having a 4-year college degree or more (3.60 [2.09, 6.21]). The variable looking at the role of time showed that at time points 2 and 3, the likelihood of relying on print news as a primary source of information decreased. Factors associated with an increased likelihood of using social media were younger age (17.27 [9.74, 30.63]; 5.37 [3.10, 9.30]) and higher levels of educational attainment (2.04 [1.02, 4.11]; 2.17 [1.02, 4.60]). Retiree status decreased the likelihood of relying on print news as a primary source of information (0.29 [0.13, 0.65]). Age below 30 (4.01 [1.97, 8.17]) was associated with an increased likelihood of relying on the doctor. Factors associated with an increased likelihood of primarily using government sources were age below 30 (4.54 [1.81, 11.37]) and having health insurance (11.06 [2.30, 53.24]). Living in the mid-US decreased the likelihood of relying on government as a primary source of information (0.42 [0.19, 0.91]). The factor associated with an increased likelihood of using social media was younger age (8.66 [4.64, 16.14]; 3.34 [1.81, 6.19]).
Weighted Multivariable Multinomial Logistic Regressions for the Association Between Zika Primary Source of Information and Demographics
The results of Tables 2 and 3 support the hypothesis that there are demographic segments of the population more prone to use particular sources. Based on these results, and the particular relevance of reaching Hispanic women regarding the Zika virus, Figure 2 identifies the results of demographic profiles that were found, in comparison to the entire population. Due to a limited statistical power in assessing interaction terms in a multinomial regression, we tested these potential segments in a bivariable fashion. Three profiles in particular are presented: high-education high-income adults, Hispanic women of childbearing age, and retirees over the age of 65 with less than a high school education (Figure 2).
Profile 1: High-education high-income adults were most likely to use print news (50.1%) and less likely to use TV and radio (29.6%) or social media (7.5%).
Profile 2: Hispanic women of childbearing age (18-45) were more likely than the overall population to use social media (21.6%) and the most likely of the groups to rely on family, friends, or coworkers (9.9%).
Profile 3: Retirees over the age of 65 with less than a high school education were dramatically more likely to use TV or radio as their primary source of information (78.6%) and less likely to use most other sources compared to the overall population.
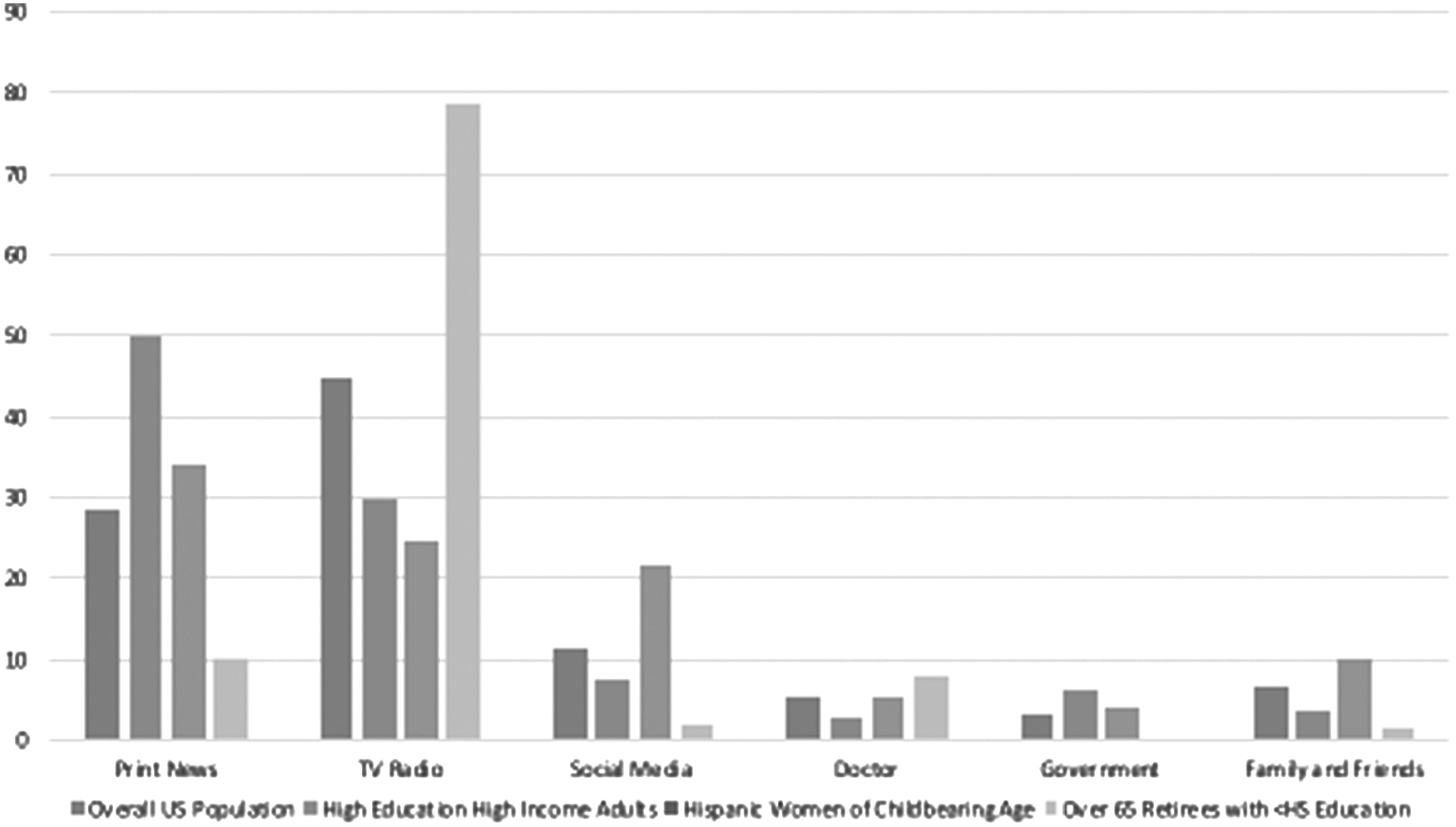
Demographic Segments' Source of Information Use
Discussion
This article explores the breadth of information sources the public accessed for Zika information, the most salient demographic factors that predicted use of a particular source of information, and how particular vulnerable, high-risk, or common population segments vary in the sources of information they rely on. There are 3 key points to highlight: the distribution of sources among the population, the role of social media and physicians, and the utility of examining demographic profiles.
The analyses demonstrate the variety of sources accessed by the US population and highlight how different demographic groups primarily access information during an emerging disease epidemic. This is the first analysis to examine how individuals access and prioritize sources of information in such an event, and it reflects not only the breadth of sources the population relies on, but also the variation in where different groups turn for information. The majority of the population relies on more than 1 source of information (72%), and most commonly get information from TV and radio (74.1%), followed by print news (65.6%).
Responding and communicating about an emerging threat requires resources. The most and least used channels of information are important for risk communicators because they suggest how to reach the majority of the population and how to reach particular demographic groups most effectively. Recent threats have drawn attention to the role of social media in risk communication. Past research has focused on the role of social media as an important channel for emergency information to reach the public and has shown the most active group on social media is currently middle-aged women. 30 Prior work has also suggested that the advent of social media has enabled public health officials to communicate directly with the public, eliminating a temporal barrier for emergency information to go through traditional communication channels.36,37 The results of this analysis suggest that far more individuals still use print news and TV or radio as their primary source of information. Further, among those who do list social media as their primary source of information, only education—not gender—increased the relative risk of using social media in comparison to TV or radio (Table 3).
In the Zika epidemic in particular, public health officials encouraged pregnant women and women of childbearing age to speak with their physicians in regard to any Zika concerns. While a physician might not be a primary source of information regarding general information, he or she could be a primary, authoritative, or supplementary source of Zika information. Despite the directed messaging, only 16.6% overall got information from their doctor, which was the lowest proportion of all sources. Though this may be attributable to a large portion of the sample not being at high risk, there was no statistically significant difference in speaking to a doctor by gender, though there was by age. In fact, a higher proportion of individuals went to government websites than to their physician (Table 1).
This analysis showed demographic profiles of high-education high-income adults, Hispanic women of childbearing age, and retirees over the age of 65 with less than a high school education relied on different sources for Zika information. These are intended to be illustrative examples of subsets of the population that exist and could be targeted, depending on the emerging threat. In conjunction with Table 2, which shows variation among demographic groups, and Table 3, which highlights some of the most salient characteristics that predict variation in primary source, these profiles offer a level of specificity that public health officials can use to reach particular groups. Because of the rapidly evolving threat of an emerging disease, public health officials may not be able to consider the most desirable channels in real time.
The information in this analysis is therefore useful, as it may be applied to future emerging disease threats to understand how factors such as employment status, income, education, and age interact to shape the sources of information particular groups rely on for emerging information. While women of childbearing age, especially those who were pregnant, were considered the highest risk group in this threat, public health interventions for emerging threats are dependent on the support of adults of many different demographics, so it is important to consider the salience of media channels in multiple demographic segments, as presented here, for each emerging threat.
In the Zika epidemic, women of childbearing age, and, in particular, Hispanic women of childbearing age, were at high risk.21,25,38 Much of CDC's messaging was targeted at this demographic group. 25 These results suggest that social media would be a more effective channel to reach this group than other groups. In addition, because this group was most likely to rely on family and friends as their primary source of information, inundating local community settings to share information could aid in targeted messaging. In contrast, public health officials aiming to target retirees with lower levels of education would most likely want to communicate through TV to reach them.
There are limitations to this study. Individuals were not limited to the information sources asked about in the survey and were not asked about frequency of information access, particularly stories of interest about Zika. This means there may be additional sources and factors that relate to information salience that are not captured in this analysis. Rather than focus on the particular publication a story came from, we have grouped sources based on the type of delivery, such that online and print news were grouped together, as they require reading and thereby a level of literacy, while TV and radio were grouped together, as they require listening. These results still demonstrate that there are meaningful differences in the sources and the primary source of information for subsets of the population, and identifying channels that are more prevalent with one group versus another can help promote emergency health communication. Data in this study were collected at 3 time points and therefore did not cover the entirety of 2016. Results capture population use of sources for the approximately 6-week time frames when data were collected. We were not able to test the demographic profiles in a multivariable analysis due to lack of statistical power. Further analyses should use more advanced statistical methods to examine if there are latent characteristics that predict a primary source of information.
Despite these limitations, results reflect important variation in sources of information for Zika virus and demonstrate 2 key considerations for public health officials in an emerging threat situation. There are many ways the US population gets information. Public health officials need to target these channels to reach intended segments of the population. To reach the greatest portion of the population, conventional broadcast media, TV and radio, are still the most effective media. The highest proportion of the US population got information about the Zika virus from conventional broadcast media, and there were a limited number of predictors in the multinomial analysis that statistically significantly increased the likelihood of primarily relying on another source (Table 3).
However, in many emerging disease threats, there are segments of the population that public officials must reach because they are at high risk for the threat or they need to make a health behavior change to control the threat. These particular demographic groups can be targeted by understanding their primary sources of information and communicating through these channels, such as social media or print news for the demographics presented here. Given the challenges to communication in emerging threats due to the evolving nature of the message and abundance of information, this analysis highlights how risk communicators can reach the public, or subsets of the public, in an emerging disease event.
Footnotes
Acknowledgments
This work was supported by National Science Foundation RAPID grant 1638545, principal investigator David M. Abramson.