
Abstract
Infectious disease response, particularly high-consequence acute infectious disease and special pathogen response, requires the coordination of numerous public and private entities to ensure the safety and appropriate care for patients, healthcare and EMS staff, and the public. The Northwest Healthcare Response Network, an independent 501(c)(3) healthcare coalition, has partnered with the local health departments in the Puget Sound area of Washington State to develop a communication and decision-making structure to support coordinated information sharing, patient care, patient transportation, laboratory testing, contact monitoring, and healthcare and EMS staff safety in events involving suspected or diagnosed acute infectious disease patients. The network has developed a comprehensive regional plan and associated tools outlining standard communication practices that include defining who will lead coordinated communications and decision making concerning patient care needs and how all partners will connect during an acute infectious disease response. Over the past 2 years, the network has tested and refined these communication and coordination processes through a facilitated tabletop exercise and a webinar-based functional exercise. These processes can serve as a model to inform the creation of coordinated communications structures for infectious disease response in communities around the country.
Infectious disease response requires coordination of numerous public and private entities to ensure the safety and appropriate care for patients, healthcare and EMS staff, and the public. The Northwest Healthcare Response Network partnered with local health departments in the Puget Sound area to develop a communication and decision-making structure to support coordinated information sharing, patient care, patient transportation, laboratory testing, contact monitoring, and healthcare in events involving suspected or diagnosed acute infectious diseases.
I
In a globalized society, emerging and acute infectious diseases are easily transported and transmitted around the world. 6 The Puget Sound region of Washington State is the Pacific Northwest's most populous region and an international hub for travel, commerce, and tourism, as well as home to numerous humanitarian organizations with staff that regularly travel overseas. Thus, the region may be more susceptible to infectious diseases transmitted locally or through introduction by international travelers. Regional healthcare organizations, healthcare preparedness coalitions, and public health agencies, however, have not planned for and responded to these threats in a collaborative and coordinated way, leaving a fragmented approach to acute infectious disease preparedness. This changed following the 2014 West African Ebola outbreak. All healthcare partners recognized the need to build a single coordinated response process capable of addressing Ebola or any other acute infectious disease response.
Following this unprecedented outbreak, the US Department of Health and Human Services (HHS) Assistant Secretary for Preparedness and Response (ASPR) provided local healthcare coalitions funding through the Hospital Preparedness Program (HPP) to help ensure that the nation's healthcare system is able to safely identify, isolate, assess, transport, and treat patients suspected of acquiring Ebola.4,7 Part A of the grant funding provides support for healthcare coalitions to plan with regional healthcare facilities for Ebola and other highly pathogenic disease responses and engage partners for regional planning, training, and exercises. 7
The Northwest Healthcare Response Network is an independent 501(c)(3) that serves as the healthcare coalition in King, Pierce, and Kitsap counties in Washington. A healthcare coalition is “a collaborative network of healthcare organizations and their respective public and private sector response partners within a defined region.” 8 The network, in collaboration with partners in Snohomish County, Washington, worked to create plans, training sessions, and exercises to sustain regional infectious disease response planning. King, Pierce, Kitsap, and Snohomish counties encompass more than 4 million residents 9 and more than half of the state's hospital beds, including 2 of 3 Ebola treatment centers (adult and pediatric) and 4 of 6 Ebola assessment hospitals in Washington State.
Consistent definitions and terminology for this work are important but have been difficult to come by. After the Ebola 2014 outbreak, many were struggling to find consensus on how to describe similar infectious diseases, including “special pathogens,” 7 “highly pathogenic diseases,” 7 and “high-consequence infectious disease.” 10 The network chose the term “acute infectious disease response,” which for this article is defined as a response to any new, emerging, or severe infectious disease incident that likely requires significant multi-agency and possibly multi-jurisdictional response beyond routine infectious disease investigation, coordination, and response. The word “acute” characterizes both the importance of the pathogen as well as its community impact, which requires coordination beyond the normal infectious disease work of healthcare and public health partners.
The network's goal was to develop 4 pillars of acute infectious disease preparedness: planning, training, exercising, and an advisory group. The network developed a regional, inclusive, and comprehensive plan to address all acute infectious disease response scenarios by expanding on lessons learned from the 2014 Ebola outbreak. Additionally, the network worked to identify planning and operational gaps and develop a regional acute infectious disease advisory group to support planning, training, and conducting exercises. Lastly, regional partners come together annually to identify gaps and to test and exercise streamlined coordination through tabletops and functional exercises to help ensure the sustainability of the region's acute infectious disease preparedness and response infrastructure.
Identification of Gaps
Recent US Ebola cases, and local Ebola rule-outs of persons under investigation, have identified regional gaps in planning for a potential acute infectious disease response. The Ebola cases in Dallas, Texas, in fall 2014 identified the need for (1) early identification of possible Ebola disease, (2) minimizing exposure of healthcare staff, (3) monitoring a large number of community and healthcare contacts, (4) large-scale healthcare staff training to support care, (5) protocols for safe patient transport, and (6) identifying designated facilities that can care for suspected Ebola patients. 11 In the response to the case of a humanitarian aid worker diagnosed with Ebola in New York City in October 2014, officials identified the importance of interagency collaboration to support response activities, including identification of potentially ill travelers, procedures for handling remains, clear and implementable monitoring procedures, and data management for monitoring. 12 New York City's Department of Health and Mental Hygiene also found that it was “challenging for health officials and health care providers to stay vigilant for high consequence but low-likelihood events and to maintain a high level of preparedness for managing such events safely.” 13 The Ohio Department of Health similarly identified the importance of creating plans for identifying potential screening facilities for Ebola, assessing emergency medical services (EMS) transport abilities, and monitoring a large number of contacts. 14
In Washington State, there were several cases of ruling out Ebola in persons under investigation while monitoring travelers and humanitarian aid workers returning from West Africa. During a meeting hosted by the network in fall 2015, healthcare and public health partners identified local lessons learned and gaps in: (1) communications among healthcare and public health partners concerning a patient's exposure history; (2) coordinated decision making to identify an Ebola assessment hospital or treatment center able to receive the patient; 15 (3) coordination of decision making concerning patient destination and transport; (4) communications on the timing and method for confirmatory laboratory testing and results reporting; and (5) point-of-care testing abilities at receiving facilities. Healthcare, healthcare coalition, and public health partners (local and state) identified the need for more detailed plans to support the coordination of these response activities. 16 Since many of the Ebola assessment hospitals and Ebola treatment centers are concentrated in a few regions in Washington State, coordinated communications and decision making is especially necessary if patients are moving across jurisdictions.
Though many of these 5 locally recognized gaps were specifically identified during the 2014-15 Ebola response, planning for these gaps is applicable to other acute infectious disease scenarios. In seeking to sustain the important advancements made from Ebola preparedness, the network identified the need to take an all-hazards approach to infectious disease planning and response by creating a flexible and scalable framework for coordinating decision making and communications in acute infectious disease responses. The network sought to address the following important sustainment questions: What communication structures are needed? Who should be included in coordination? How will information be shared? How will the range of infectious disease responses be addressed? How can engagement, training, and exercises be sustained?
Coordinating Communications and Decision Making
Beyond daily disease investigation pathways and prior to this regional planning effort, no regional protocols or processes were in place involving the full spectrum of key stakeholders to coordinate acute infectious disease communications and response. These daily processes would quickly become overwhelmed with the magnitude and complexity of an acute infectious disease response. To address coordination gaps in planning, decision making, and communications, the network created a regional acute infectious disease response plan to define healthcare organization roles and responsibilities (including hospitals, ambulatory care, long-term care, home health/home care, and support services). The plan also defines the relationship of these healthcare organizations with local health jurisdictions, emergency medical services, and other regional and state emergency preparedness partners. The plan includes a general concept of operations for responding to acute infectious disease patients and applies to:
An acute infectious disease response in the region or affecting it that likely requires a significant multi-agency response for any new, emerging, or severe infectious disease situation beyond routine investigation, coordination, and response. Healthcare organizations, the network, local health jurisdictions, and all partner agencies with whom there are established memoranda of agreement, procedures, or protocols for acute infectious disease incidents.
The plan identifies a process to inform regional partners, activate and coordinate response processes, and identify the healthcare and partner response needed. Additionally, the plan identifies processes required to triage patients (for healthcare and EMS), transport patients to and among healthcare facilities, test laboratory samples, dispose of potentially contaminated waste, and coordinate mortuary service. All hospitals and ambulatory care facilities are expected to maintain a baseline level of preparedness to identify, isolate, and notify partners of a possible acute infectious disease patient. The network worked with local public health partners to identify the lead and support agencies for monitoring healthcare patients and staff as well as the public (Table 1). A key part of the plan is to identify if and how to incorporate the Ebola 3-tiered hospital response model of treatment centers, assessment hospitals, and frontline facilities 15 into the broader acute infectious disease response. Adapting a tool created by the Mayo Clinic, the network identified infectious disease response categories based on the burden of operations required by healthcare partners (Table 2).17,18 Pathogens that fall into category 1 are those most appropriate to apply the 3-tiered hospital model.
Potential Monitoring Responsible Parties by Facility and Person Type
Category A: An infectious substance that is in a form capable of causing permanent disability or life-threatening or fatal disease in otherwise healthy humans or animals upon exposure to the substance. 18
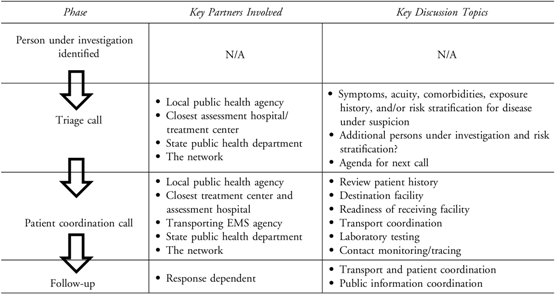
Along with the main regional response plan, a key attachment was created to provide practical and actionable steps to implement the planning concepts. Following several local Ebola rule-out cases in the Puget Sound region, partners identified specific gaps in a coordinated decision-making structure for the care, testing, and transportation of persons under investigation for an acute infectious disease. This attachment identifies a 2-tiered coordinated conference call approach for multiple partners to engage in collaborative decision making. These 2 conference calls (triage call and coordination call), defined in the decision-making and communications protocol, outline suggested participants as well as discussion agendas to guide appropriate decision making (Table 3). The conference calls address topics of patient care needs, infection prevention practices, patient transportation, laboratory testing requirements, healthcare and public information dissemination, and contact monitoring.
Acute Infectious Disease Decision Making and Communications Flow
The plan and the attachments were reviewed with key stakeholders through the acute infectious disease advisory group, local healthcare partners (including EMS), and local public health officials (epidemiology and preparedness) through meetings and written review. Edits and feedback were incorporated, and the plan was finalized and distributed to partners. Webinar-based training sessions were created for all regional healthcare, EMS, and public health partners on the resources in the plan and relevant attachments.
In April 2016, the network developed and hosted a tabletop exercise designed to test the regional plan as well as health and medical plans and response operations for an acute infectious disease scenario. The exercise also served as a gap analysis for advising the network on where to focus federal grant funding targeted for acute infectious disease preparedness and response readiness and sustainment. The exercise used a regional outbreak scenario to test objectives focusing on coordination and communication within and among healthcare organizations, public health agencies, and EMS providers. Exercise attendees included participants from 4 counties representing 4 public health planning regions and the Washington State Department of Health, as well as representatives from treatment, assessment, and frontline healthcare organizations; local health jurisdictions; EMS providers; and healthcare coalition partners.
Important regional gaps identified through the exercise included a lack of standardized screening guidelines for healthcare and EMS, coordination of patient transport, communication and coordination among healthcare and public health agencies for decision making, laboratory testing communications and procedures, healthcare staff monitoring, and sustained training for all partners and staff. To address these gaps, the network convened an acute infectious disease advisory group, consisting of healthcare, public health, EMS, and healthcare coalition experts to provide strategic direction to close gaps and sustain planning, training, and exercises. Participants represent a 4-county region and include infectious disease physicians, infection preventionists, employee health clinicians, epidemiologists, emergency managers, laboratorians, and partners from local, regional, and state government. The advisory group provides strategic input to identify regional training needs to support healthcare preparedness and response on topics such as laboratory testing and patient screening. The advisory group additionally serves as the planning committee for all regional acute infectious disease exercises and drills.
Testing Coordination
Building on the 2016 tabletop exercise and the engagement with the acute infectious disease advisory group, the network hosted a 3-county webinar-based functional exercise in August 2017. The exercise was designed to test the regional acute infectious disease plan's decision-making and communication protocol. It used a cross-regional outbreak scenario to test objectives focusing on the ability of healthcare organizations, public health agencies, and EMS to coordinate patient care decision making for acute infectious disease patients. Exercise participants were from King, Pierce, and Snohomish counties, representing local health jurisdictions; the Washington State Department of Health; representatives from treatment, assessment, and frontline (hospital and outpatient) healthcare organizations; and EMS.
The webinar-based format of the exercise simulated the actual coordination method (conference call) that would occur for this type of response. The scenario focused on 4 mock patients from the 3 counties who had contracted an unknown acute infectious disease. The patients were purposefully identified as adult, pediatric, and pregnant patients, further pushing the need to focus on specialty care. There were 6 primary objectives: regional/partner coordination, patient distribution, patient transport, laboratory testing, healthcare and public information, and staff/provider safety. Players participated from their home facilities since the exercise was conducted remotely. The exercise scenario and resulting discussion explored a variety of existing plans, continued challenges, and several improvement opportunities regarding the coordination, communication, and transport of patients suspected of having contracted an acute infectious disease.
Overall, the exercise achieved the outlined objectives. Participants were knowledgeable about organizational and regional plans to appropriately respond to the scenario. Participants made decisions about the appropriate patient treatment facilities as well as transportation assets to move them there. Additionally, partners discussed topics concerning laboratory testing, public information, and provider safety. Participants particularly enjoyed the webinar-based format for both the ease of participation and the realistic setting for this type of discussion.
Several key lessons were identified from the August 2017 functional exercise. Participants thought additional partners (particularly the Washington State Department of Health) should be present on an initial triage call in a multi-jurisdictional event. Participants also identified the need for 2 additional follow-up calls: one to confirm patient arrival at a destination facility, and an additional call to discuss public information needs and strategies. Partners requested draft agenda templates and an outline of goals for each of the conference calls. Additionally, more discussion would be needed concerning laboratory testing in a real incident, as this topic was curtailed due to exercise artificialities. More discussion is also required to determine how local/regional planning for acute infectious disease coordination is aligned with Washington state-level planning and the support of the Health and Human Services (HHS) Region X treatment center.
Discussion and Conclusions
Through the implementation of the 4 pillars of acute infectious disease preparedness—planning, training, exercises, and the advisory group—the network, along with regional partners, has built on planning begun during the Ebola response in 2014 to develop a sustainable collection of tools and resources for regional acute infectious disease preparedness. The network has followed regional planning efforts with strategic training and exercises to complete the full preparedness planning cycle. 19 Involving multi-jurisdictional and multidisciplinary partners allows the region to identify who, how, and when partners must come together for collaborative communications and decision making to prepare for or respond to a possible acute infectious disease incident. Involving multiple counties throughout the Puget Sound area allows the most populous region in the state to have a standard approach and set of expectations for all partners across the footprint of healthcare systems and public health jurisdictions.
A major strength of the network's acute infectious disease project is gaining the involvement, trust, and interest from regional partners to create standard protocols and expectations for better coordinated incident response. Healthcare partners see the value in coordinating with their local and state public health department and EMS counterparts to best serve patient needs. Public health partners in turn found benefit in consistent communication pathways to expedite response operations. Finally, EMS agencies provided vital insight into the dual challenges of transporting an acute infectious disease patient and coordinating information flow with staff and partners. This collaborative planning cycle allowed for the creation of strategic planning frameworks, training, and exercise programs that support the needs of all regional partners and test vital aspects of regional response capabilities.
There are limitations, however, to this novel approach to acute infectious disease planning sustainment. This in-depth and multi-jurisdictional approach to planning, training, and exercises can be labor intensive for healthcare coalitions that may not have adequate staff resources to execute it. To mitigate any additional burden, coalitions can consider scaling back the number of participants in an advisory group to fit regional needs, partnering with neighboring coalitions, and identifying a community champion (in infectious disease) to help support planning, training, and exercise needs. In multi-jurisdiction planning, it is also often difficult to engage geographically distant partners. Using webinar and conference call–based tools has allowed the network to engage a larger number, and a more diverse group, of expert partners to support this work.
Challenges to regional acute infectious disease preparedness and response include narrowing outstanding gaps, refining plans, and continuing to test updated plans through regular exercises. The acute infectious disease response plan and attachments must be continually updated to provide actionable and response-ready templates to streamline communications and coordination processes. More discussion is needed to identify best practices to coordinate public messaging and communicate laboratory testing results between regional partners. To our knowledge, there were no unintended consequences through this planning effort, and all partners have fully embraced the new processes. However, the plan and its protocols have only been tested in a simulated environment and not in a full-scale exercise or during an actual or suspected acute infectious disease incident. Additionally, through the Ebola grant funding, Part A, the network must continue providing planning, training (at least 1 a year), and exercise (1 a year) opportunities to coalition partners on acute infectious disease topics.
The network has created a comprehensive framework to develop, train, and exercise all-hazards infectious disease planning that incorporates processes developed during the 2014 Ebola response. This framework solidifies a sustainable process to address any new or emerging infectious disease incident response. Through continued planning refinement, partners work together to tackle outstanding gaps and prioritize training needs for healthcare, public health, and the broader response sector. This flexible planning framework can be used by other healthcare coalitions and collaborative healthcare and public health organizations to develop and/or strengthen regional acute infectious disease response capabilities in this post-Ebola planning atmosphere.
Footnotes
Acknowledgments
Funding for this project was provided through support from the US Department of Health & Human Services, Assistant Secretary for Preparedness and Response, Hospital Preparedness Program, through contracts with the Washington State Department of Health.