
Abstract
From the Field
is a semi-regular column that explores what it means to be a local health professional on the front lines of an emergency. Typically, National Association of County and City Health Officials (NACCHO) members share their stories of preparing for and responding to disasters, epidemics, and other major health issues. This month's column features a submission from the New York City health department that describes their experience in setting up a radiological advisory committee. Through exploring the analysis of the challenges faced and the solutions developed, readers can learn how these public health champions keep their communities safe even in extreme situations. Readers may submit topics of interest to the column's editor, Meghan McGinty, PhD, MPH, MBA, at
A significant radiological emergency response in New York City would require scientific expertise beyond the routine capability of the New York City Department of Health and Mental Hygiene (DOHMH) and its partner agencies. Health physicists (radiological safety specialists) are chronically in short supply in the United States, which translates into a limited supply available to local health departments facing a radiological crisis. These professionals support medicine, industry, and the military in routine, nonemergency situations. In order to prearrange the availability of this expertise, a radiological advisory committee (RAC) was formed. The committee engages leading experts in the fields of radiation medicine and environmental radiation science in anticipation of the technical questions that arise from the clinical aspects of internalized radioactivity and the mitigation of the urban environment following a terrorist attack using radioactive materials. The creation of the RAC and its application in a nonemergency public policy forum is described, as are the problems foreseen in operationalizing the RAC during an emergency. Some conclusions are drawn about the effort and cost of maintaining the RAC and the benefits obtained by maintaining it. This information may be useful for other jurisdictions seeking to form a similar expert committee.
R
Not all health physicists are trained in emergency response nor in the incident command structure and its protocols, which exacerbates the shortage of expertise. In addition, a city agency responding to an incident needs a cadre of experts that can volunteer significant time and resources. A potential source are hospitals that maintain nuclear medicine and radiology departments, because they must have a designated radiation safety officer (RSO) for regulatory compliance purposes. Though they may want to assist in an emergency, they are committed first and foremost to the hospital. Any voluntary assistance they could render would be on an ad hoc basis.
The technical challenges of a radiological response also demand expertise beyond what local departments may possess or be expecting. These include:
Federal assistance such as the Federal Advisory Team, the Radiological Assistance Program, and other capabilities that may arrive on scene relatively quickly but only after a request through the state. Even after arrival, these assets may not have a direct communications tie to the local health department to provide the needed expertise. The environmental issues concerning the potential extent of the radioactive contamination and interpretation of the radiation readings for public health assessment will be unprecedented. The medical/clinical experience of local healthcare providers regarding radiation injury is almost universally nonexistent.
These restrictions limiting access to health physics experts compelled the formation of a standing committee that can be called on in times of crisis. These challenges are also reflected in the design of the radiological advisory committee (RAC), which requires experts in 2 broad areas: radiation injury and environmental radioactive contamination.
Other more general reasons for developing outside assistance have been mentioned previously in the literature. Expert committees are recognized to provide better, faster, and less biased decisions than those arising solely from individuals, and using a panel of experts allows expanded capacity to address novel problems or those that do not have a previous history to draw response planning from. 2 Previous research indicates that these panels perform best when participants are drawn from varied relevant disciplines. 3 Investigators have revealed other insights, such as mitigating the effects of professional status on committee dynamics 4 and counteracting “groupthink,” a recognized problem 5 that can suppress valuable dissenting viewpoints when competent facilitation is not provided.
In contrast to previous committees formed by the Department of Health and Mental Hygiene (DOHMH) in response to Zika (2016) and Ebola (2015), the formation of the RAC before an incident was a proactive move that satisfied a major radiological planning objective but that also resulted in significant commitments by DOHMH (discussed below).
Building the Radiological Advisory Committee
Populating the RAC was largely based on finding expertise to fill the 2 broad areas expected to dominate public health concerns after an event involving a radiological dispersion device: environmental radioactivity (essentially contamination issues) and clinical care for radiation injury (including the internalization of radioactivity). These technical concerns are summarized in Table 1. To further assist in choosing RAC personnel, a list of emergency response skills expected to be useful in a radiological crisis was created (Figure 1).
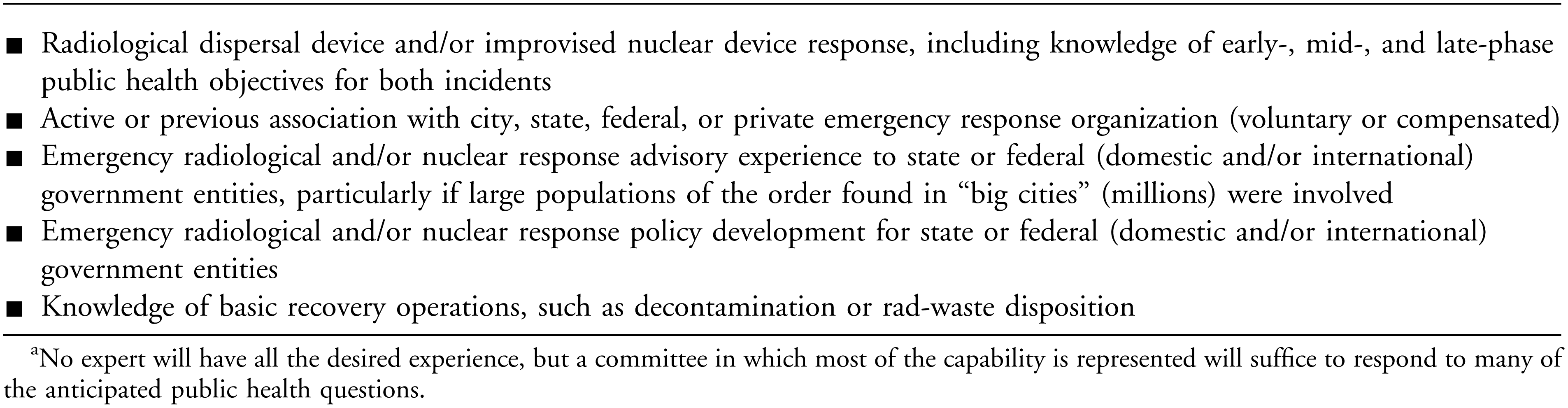
Emergency Response Experience Desirable for RAC Participationa
Technical Issues for RAC Consideration in a Radiological Crisis
For more information about radiological dispersion devices—also known as “dirty bombs”—see https://emergency.cdc.gov/radiation/dirtybombs.asp. Information about improvised nuclear devices can be found at https://emergency.cdc.gov/radiation/nuclearfaq.asp.
Community reception centers are facilities where the mass screening of the public for radioactive contamination and subsequent health-risk estimation can occur. In NYC, community reception centers would be set up in public buildings and run jointly by DOHMH and the fire department. For a general overview, see https://emergency.cdc.gov/radiation/crc/vcrc.asp.
To fulfill this objective, the DOHMH's 2 radiological principal scientific advisors contacted experts who they knew by reputation or from previous collaborations. This effort was supplemented by reviewing directories such as the Directory of Personnel Responsible for Radiological Health Programs 6 so that invitations could be sent to experts that the principal scientific advisors did not know. These personnel were employed by various response agencies such as the Environmental Protection Agency, the US Department of Energy, and New York State agencies such as the Division of Homeland Security and Emergency Services.
An important consideration affecting personnel choices was the magnitude of New York City's complex population (Table 2). People who have had experience working in large, complicated, and, in some cases, national radiological crises (eg, the 2011 Fukushima Nuclear Power Plant accident) bring a unique perspective to the committee, one that considers the implications of and protection actions for very large “big city” populations. For example, the Japanese Health Risk Management project, designed to track public health detriments as a result of the Fukushima accident, has contacted more than 2 million people. 11 Public health considerations of populations this large is common in New York City.
Relevant Characteristics of New York City Affecting Various Aspects of a Large-Scale Emergency Response Including a Radiological Dispersal Device
Based on values found in Moss and Qing. 7
Based on a calculation using data from Radiological Dispersal Device (RDD) Response Guidance. 8
The result of this solicitation effort was that we acquired personnel who fulfilled most of the environmental, medical response, and “big city” staffing objectives anticipated for the RAC (Table 3).
RAC Representation
Table does not include representatives from NYC response agencies (NYPD, FDNY, and DEP), which can send 1 subject matter expert each to the incident scene. Later, these subject matter experts can fold into the volunteer RAC indicated here. DOHMH principal scientific advisors (2) also are not included in the table.
Decontamination and decommissioning company.
Putting the RAC to Work
Once interest in participating was established, the first all-day workshop of the RAC was planned and executed within 4 months (May 2015) with approximately 30 participants, including RAC members and local emergency planning partners. The agenda included an overview of radiological emergency response in NYC, federal and state assets that would be expected to assist NYC in such an event, and an overview of the community reception center operation to be used to provide public monitoring and decontamination after a radiological dispersion device event. The committee was then divided into the 2 expert subgroups to discuss environmental remediation and clinical policies. Note takers captured the discussions, and a document that acted as the formal record of the outcomes was provided to all the participants within a few weeks of the workshop. Later, to formalize membership and operational capability, a RAC membership handbook was written and shared with members describing the committee's function and where it resided in the emergency response incident command structure.
Since the first meeting, RAC members have been further engaged in a policy and planning discussion. In December 2015, concern was raised about the accidental release of radioactive iodine from the Indian Point Nuclear Power Plant (IPNPP), located about 25 miles north of NYC. It was suggested that potassium iodide (KI) be purchased and predistributed to NYC residents—or at least to the most vulnerable subpopulation: some 2 million who are under the age of 18, combined with the current population of pregnant women (Table 2). The timing coincided with unfounded concerns about thyroid cancer in Japan that surfaced after the Fukushima nuclear power plant accident of March 2011. These concerns were accelerated by the publication of a questionable epidemiology article linking the apparent sudden appearance of thyroid cancers to the Fukushima radioactive releases. 12 Though the results of the article were quickly refuted by other epidemiologists, 13 DOHMH was still pressed to consider the purchase. The acquisition, storage, distribution, and ongoing public education campaign that would be needed to support the proper use of KI would be a community outreach, logistic, and financial challenge. However, before full consideration of these issues could be had, a very basic question required a response: Was the KI needed at all?
Policy Meeting
Formulating a policy for or against KI acquisition and distribution is a challenge well-suited to an expert committee. The members are not involved with DOHMH on a routine basis. As nonemployees, they are never involved with the day-to-day administrative, financial, and political concerns that could easily influence decision making. As envisioned, the RAC provides policy recommendations based on science alone. RAC recommendations would be folded into other considerations by DOHMH, such as developing related public messaging and community education on the policy, financial planning, and other factors that department staff are more familiar with than the RAC.
To determine whether predistribution of KI was a sound scientific strategy for NYC, a half-day policy deliberation meeting was conducted on March 16, 2016, with RAC participants, relevant stakeholders, and city representatives from DOHMH partner agencies. RAC members were told in advance about the purpose of the meeting as objectively as possible. It was understood by all that DOHMH was willing to formally integrate the recommendations of the RAC regarding the decision to purchase, store, distribute, and educate the public about KI into future radiological planning, whatever the outcome. The discussion focused on these key primary points:
The radiation doses necessary to significantly increase the probability of thyroid cancer induction in a population were reviewed. This drew on knowledge of previously reported effects—for example, thyroid cancer frequency after the Chernobyl incident and the estimated thyroid doses of the Japanese public after the Fukushima accident. Environmental factors of an event were explored including the meteorology of the Hudson River Valley and its potential effects on radioactive plumes. The concern was the meteorological conditions needed to maintain a coherent, concentrated plume over the 25-mile distance from the IPNPP to NYC that could lead to inhalation doses of radioiodine high enough to warrant use of KI. This discussion involved such issues as the frequency of winds blowing toward NYC from the north, where the reactor is located. A plume computer model shared by a RAC participant (a health physicist) demonstrated the magnitude of reactor meltdown (unrealistically high) to create radiation doses sufficient to trigger use of KI.
14
The engineering of the IPNPP with emphasis on the capability to mitigate catastrophes was explained. The very low probability of catastrophic mechanical events leading to the release of significant amounts of radioactivity provided a deeper understanding about how to prioritize a potential nuclear power plant crisis. The low probabilities of an accidental release and the rare conditions necessary to bring radioiodine concentrations to NYC requiring KI to be used were one of the results of this discussion.
A key component of the success of the meeting was its facilitation. Any politicization of the decision whether to purchase, store, and distribute KI without rigorous scientific merit was of concern. Therefore, the facilitator, a DOHMH deputy director, firmly established at the start of the meeting that the objective of the discussion was to formulate a KI policy based solidly and solely on science.
To maintain this desired science-based discussion, a radiological principal scientific advisor discussed the technical issues during an opening presentation that provided an overview of the IPNPP concerns: meteorology, proximity to NYC, nuclear industry plans to respond to a crisis, and a review of other state-run KI distribution plans. This presentation culminated in 4 questions that served as the focus of the KI policy meeting agenda:
1. What are the probabilities of an event at Indian Point that can lead to a prolonged release of radioactivity, as happened at Fukushima? 2. Does the science (eg, from Fukushima) inform us to predistribute, or does it support the current emergency planning zone recommendations
*
from the Nuclear Regulatory Commission (NRC)? 3. What is the most effective predistribution model for KI in large urban settings like NYC? 4. If KI is not predistributed, are there alternatives, such as public notification, shelter in place, and/or evacuation?
The facilitator maintained focus on the agenda while assuring that each question received the time needed for a thorough exploration. Meeting notes and conclusions were documented by 2 scribes. The advocate for KI predistribution posed questions and concerns that were discussed within this established framework (the advocate also agreed to abide by the recommendations proposed by the RAC). The RAC endorsed a shelter-in-place strategy over a policy of acquisition, storage, or distribution of KI based on the environmental, engineering, and health implications of past nuclear power plant incidents. The combination of nuclear engineering, environmental science, radiation medical expertise, and mass-population radiation dose assessment that the RAC brought to the discussion allowed the decision-making process to be informed, comprehensive, and, most important, fact based. This proved to be a successful strategy, allowing for a collegial and informative discussion.
The RAC Matures
A third RAC meeting, intended to investigate how to properly incorporate the advisory group into the DOHMH incident command structure, was held on May 15, 2017. The agenda explored some very basic mechanisms for operationalizing the RAC, including the following:
Establishing an efficient way to alert the RAC for a first meeting post-incident. ○ Result: Use phone and e-mail messaging. Exploring the various forms of communication between DOHMH and the RAC during the incident—for example, some RAC participants can be present at DOHMH's agency emergency operations center; others will only be available by phone. Coordination of teleconferencing resources will be required to assure communication success. ○ Result: Establish a bridge line, transmit the phone and access code numbers to the RAC, and specify the local time of the first and subsequent meetings. Determining the availability of RAC participants with existing emergency response duties; though many of the RAC participants must prioritize their employment-based emergency functions, after hours or in later phases of the emergency, it was agreed that their availability to the RAC would increase as the response continued. ○ Result: Full RAC participation will not be possible perhaps until several days after incident inception. Assessing whether RAC participants can volunteer significant amounts of time during the recovery phase of a radiological incident that may last weeks, months, and possibly years after the incident has been mitigated. ○ Result: RAC members who can continue voluntary long-term participation in the event will do so; others will not. Compensation for long-term participation was not discussed. Determining the RAC's access to environmental data obtained from first responder radiation detection equipment is crucial for determining situational awareness. In NYC, one electronic data-sharing site where these data are collected and displayed on a map of the incident area is the FEMA-sponsored Rad-Responder
15
data platform. This site is accessible for setting up agency accounts and can be viewed by multiple personnel belonging to the agency or can be shared between agencies. Some training is required to efficiently use the platform.
○ Result: Requiring RAC members to learn how to use Rad-Responder was considered impractical; DOHMH will summarize the data map and transmit that to the RAC. • How to best use medical experts on the RAC who cannot practice medicine on patients because they are out-of-state doctors who are not licensed to practice in New York State. This presents a liability issue that requires a work-around so that their medical expertise can still be accessed. ○ Result: RAC medical experts will consult only, not treat. DOHMH can facilitate consultation by connecting local treating physicians with RAC physicians and the Radiation Emergency Assistance Center/Training Site (REACT/S).
DOHMH held a functional exercise on November 14 and 15, 2017, to test its incident command structure response to a radiological dispersion device event in Manhattan. Although the RAC was notionalized in the exercise, it was a much-used component that planning section chiefs called on through the principal scientific advisor. The following were some of the conclusions from the exercise:
The RAC should be contacted early in the incident to prepare them for consultation. The call is best performed by assistants because of the quickly accelerating work load for the principal scientific advisor. Contacting the RAC is not a straightforward procedure for the following reasons: ○ Some RAC participants will be engaged in a NYC response by virtue of their responsibilities to their home organizations and will not be able to respond individually. ○ Because of this, only some RAC participants may be available for consultation in the first hours postincident. ○ RAC participants will need to be tracked down by phone messaging and e-mail. They are not committed to a “stand-by” status. A communications bridge should be set up for the RAC immediately. Bridge lines will be in short supply. The RAC should be given a communications priority. The RAC will need data primarily from 2 broad categories: (1) environmental radiation exposure rate values attributable to the contamination with the associated geo-locations of the measurements, and (2) clinical data for those patients admitted with injuries and potential internal exposures. ○ Rad-Responder data could be sent to RAC participants as a summary map using screen shots sent by e-mail. ○ Sharing clinical data can be arranged by DOHMH by connecting treating physicians with the RAC members and REACT/S.
Potential Concerns
Although DOHMH did not experience problems in using the RAC for the KI policy meeting or other planning and response discussions, it is predicted that certain difficulties could arise that are probably common issues for those using expert panels:
Opposing Views
It is entirely possible that polarized viewpoints exist among experts or can arise among panel members during the course of deliberations. In our brief experience with the RAC, this has not occurred—at least not in a manner that is detrimental to the functioning of the RAC. In fact, as indicated earlier, there is a danger in having a like-minded group, since a lack of dissenting opinions may result in decisions that do not fully consider all public health aspects of an issue.
Conflicting Expertise
Experts who are recognized as such are even more valued if they consider the views and experience of dissenting scientists. To harvest the expertise of a committee, it is important to let all voices have a platform as otherwise healthy competition between experts could result in domination by only one or a few voices. Rarely should egos rise to such a level as to be detrimental to group decisions. If they do, it can be countered by a facilitator who rigorously maintains open-forum ground rules.
Longevity
The RAC is different from most expert panels in that it is expected to be a long-standing voluntary panel awaiting a particular type of incident to occur before being activated. The problem of longevity is twofold: (1) panel members may remove themselves for a variety of reasons, including employment changes, retirement, or even lack of interest; and (2) the failure of DOHMH to maintain the cohesiveness and motivation of the committee.
Maintaining a group like the RAC requires at minimum periodic communication and annual or biennial meetings on topics that will interest and motivate the participants to make a further effort to participate. A related issue is to explore back-up personnel for the RAC participants. We have encouraged this not only as a means to mitigate the unavailability of RAC members in an emergency but also to encourage succession should a participant decide to end his or her association.
Politicizing the RAC
The purpose of the RAC is to respond to technical questions and ideally avoid the political ramifications of its conclusions by firmly grounding all discussions in science alone. In practice, it may be extremely difficult to parse the scientific from the political, especially for decisions with implications for “big city” public health.
Placement in Incident Command Structure
DOHMH will be the voice of the RAC after considering the RAC recommendations. In the DOHMH incident command structure, the RAC reports its findings to the principal scientific advisor, who reports out to appropriate section chiefs or the incident commander as needed. An argument can be made for placing the RAC in the planning section of a citywide incident command structure that includes local health department participation. Under this framework, the planning section will be tasked with formulating future, later-stage assessment and mitigation of the radiological contamination and will require RAC technical advice concerning the public health aspects of radiation dose to do so. The local health department can remain the voice of the RAC, but under this structure, other agencies, such as emergency management or environmental protection, may have easier, higher-priority access to the RAC. Such availability may require that the local health department screen, summarize, and combine questions when feasible to prevent the RAC from being overwhelmed.
Duplication of Effort
The RAC is not meant to replace other assets such as the federal Advisory Team for Environment, Food and Health 16 or other related capabilities that are expected to eventually become available to local responders and city government in a response to a radiological dispersal device. In the first hours of a response to a radiological dispersal device, the RAC may be the only advisory group at least partly available, primarily because time is required for the federal government to respond. As the response unfolds and federal assets appear, the RAC would maintain its incident command structure position, providing help with environmental and medical issues, but the RAC could evaluate the contributions from other assets, providing another level of assurance to DOHMH. This would be especially helpful when recommendations are unsure or require trade-offs with implications for public health. Ultimately, the final arbiter of all advice, no matter its origin, is the DOHMH, which must weigh considerations from several sources including the RAC before recommending a policy.
Evaluating the RAC Model
At this time there is no formal evaluation of the efficacy of the RAC because there has been no response to a radiological dispersal device event in NYC. However, the second annual meeting of the RAC, structured around the viability of protecting NYC residents from airborne radioactive iodine, can be used to measure its effectiveness. This use of the RAC for policy formation illustrated several advantages to having a standing committee that can be called on to rapidly advise on a radiological problem.
Specifically, although initial policy inquiries were addressed by DOHMH staff regarding predistribution of KI, further questions requiring specialized knowledge—for example, nuclear power plant accident probabilities and thyroid dose assessment—motivated DOHMH to convene the RAC. It was able to form quickly because of the success of the initial meeting and partly because the issue of KI was very familiar to many of the participants. Some of the members had advised the US government during the Fukushima nuclear power plant incident of 2011, and others had deployed to Japan to analyze data or make measurements of radiation levels and/or had expertise in the use of KI as a countermeasure.
DOHMH was additionally able to recruit, via an original RAC member, a nuclear engineer who was familiar with the risk of catastrophic accidents at nuclear facilities. He was able to articulate clearly the extremely low risks of a nuclear power plant disaster coupled with the rare environmental conditions needed to bring about the low probability scenario where NYC would need a KI distribution plan. This information and the expertise to accurately convey it would have been a challenge for existing DOHMH staff.
While a formal cost/benefit analysis has not been conducted, it can be stated that the cost of supporting annual meetings of the RAC (primarily used to cover travel, hotel, and food costs for out-of-town committee members) has been minimal. The rapid planning turnaround needed for the annual meetings means that between January, when the funding is released, and June, when the funds must be spent, DOHMH was able to fully spend down the amount requested and allocated while providing a low-cost, high-impact benefit for both DOHMH and citywide emergency management.
Therefore, we believe that a RAC or similar technical advisory committee can be sustained on a relatively small budget. This benefit is amplified if some experts can be found locally. Several medical and environmental radiation professionals on the current NYC RAC work in the city or nearby on Long Island at Brookhaven National Laboratory. Similarly, other local health departments can consider their local expert assets as a way to develop depth of expertise. If these are in short supply or the assets are too far flung to make a RAC feasible, expertise may be shared regionally. This may be formalized through a mutual aid agreement. The Emergency Management Assistance Compact (EMAC) 17 may be such a mechanism. Although New York City has not explored this concept for the RAC, the recent response of the city to the official EMAC requests for assistance from the governments of Puerto Rico and the US Virgin Islands in the aftermath of Hurricanes Irma and Maria illustrated that aid to other jurisdictions can be rendered effectively in this manner. With this experience, it is quite conceivable that RAC assistance could be extended to affected areas in the wider NYC metropolitan area. By analogy, regional governments could explore sharing a RAC from a larger nearby municipality or creating one of their own.
Conclusion
Our experience thus far with the RAC, although encouraging, is only in its beginning stages. Prior to the creation of the RAC, radiological emergency planning and responses to inquiries about complex radiological issues were addressed by agency staff or by informally speaking to local or national experts on an ad hoc basis. In a full-scale emergency, this is likely to be problematic if only because the pool of radiological experts is relatively small. Experts may not always be available to respond to spontaneous inquiries from local health departments. Furthermore, radiological issues can be diverse, spanning many professional fields. Thus, without the necessary expertise, a local health department will likely be unable to deliver an adequate and comprehensive planning or policy response. This was demonstrated when the RAC was able to bring together in one room the nuclear engineering, environmental, and radiation dosimetry modeling and expertise needed to formulate a local KI policy.
Like any association intended to be a long-term entity, the RAC will require periodic attention to maintain participant interest and a sense of allegiance to the NYC DOHMH. This is difficult, as the participants are volunteers with, in many cases, full-time positions, or they are retired with all the associated personal priorities that entails. Fostering commitment to DOHMH is necessary because ongoing response planning in the agency and between NYC agencies involved in radiological emergencies assumes that the RAC will be a key component.
In addition to experts with professional ties to local health department scientists, it is recommended that the initial committee outreach include recognized experts who are not as well acquainted in order to create a panel with a broad viewpoint. Experts with credible opposing views to the majority should be welcome despite (and even because of) the possible dissenting debate it can inspire in the group. To accommodate this wider ranging view, an experienced facilitator who can maintain the ground rules of the discussion and does not veer from a well-considered agenda is an absolute requirement. However, in a real emergency, facilitation must encourage and allow all viewpoints to be heard to allow for the best decision possible. In the end, the health department (or other sponsoring agency of the RAC) makes the final decision on the debated policy questions.
The RAC program is being considered as a model at DOHMH for the creation of similar pre-staged technical advisory groups as a low-cost way to expand access to expertise during the planning and response phases of an emergency. Local health departments can consider this proactive model to help formulate radiological incident policy and to provide advice before and during emergency responses.
Note: New York City's Radiological Advisory Committee was recognized on March 27, 2017, by the National Association of County and City Health Officials (NACCHO) Model Practices Program as a Promising Practice.