
Abstract
As ecologic, social, and economic conditions continue to facilitate the emergence and transmission of infectious diseases, local health department workers' willingness to respond will remain vital to the United States' ability to recognize and respond to new and emerging disease threats. As demonstrated by heavy occupational morbidity and mortality associated with the 2014 Ebola outbreak, infectious disease response can pose serious risks to the health workforce and presents many ethical and logistical challenges. To explore willingness to respond to an infectious disease outbreak among local health departments—the hub of the public health emergency preparedness system—we conducted focus groups with 46 local health department staff attending 2 national conferences. We examined perspectives from our participants on how local health department employees learn about and articulate their professional commitment to the department, the ways in which local health department leaders support local health department employees in responding to an outbreak, and how local health department staff articulate their responsibilities to their families. We conclude with a proposal for how a web of ethical commitments likely influences willingness to respond. These commitments and their relationship to willingness to respond should be explored further.
Responding to an infectious disease outbreak can pose serious risks to the health workforce and presents many ethical and logistical challenges. To explore willingness to respond to such an outbreak among local health departments, the authors conducted focus groups with 46 local health department staff. They examined perspectives on how local health department employees learn about and articulate their professional commitment, the ways in which local health department leaders support employees in responding to an outbreak, and how local health department staff articulate their responsibilities to their families.
A
A key component of employees' willingness to respond to an infectious disease outbreak is their ability to respond. Ability in this context refers to whether the local health department employee has the capability—the necessary knowledge, skills, and instrumental support—to respond to an event. 1 For example, whether an employee has access to childcare may influence his or her ability to respond to an infectious disease outbreak. 2 Available childcare may facilitate an employee's decision to respond—that is, their willingness to respond.
Previous research has pointed to a gap in local health department workers' willingness to respond to emergent infectious disease risks, including pandemics and the threat of bioterrorism events.6-8 Among a relatively small sample of local health workers, Balicer et al found that clinically trained local health department workers were more willing to respond than were nonclinical staff. 6 In a larger sample, Barnett et al found that public health professionals who understand their role as important to the response are the most willing; within this group, those with clinical training were most willing. 7 In later work, Barnett et al found that local health department workers with first responder training and no family members to care for had higher levels of willingness to respond to a variety of disasters, and those from rural areas had higher levels of self-reported willingness to respond to an infectious disease outbreak compared to their urban counterparts. 8
To balance public interests with those of individual health workers contributing to infectious disease response, several authors have advocated for the inclusion of ethics in pandemic preparedness.9-11 Healthcare professionals (ie, those with clinical training) are subject to a professional duty to treat. A core ethical question related to duty to treat cited in the literature is: Under what circumstances does a healthcare professional have an obligation to treat when doing so places the professional at risk?12,13 A recent survey of urban hospital-based healthcare workers in New York City found that one-quarter believed it was ethical to refuse to provide care to a patient with Ebola. 14 The study also found that 90% of the healthcare workers were concerned about transmitting Ebola to family and friends. 14 Whether local health department employees—who may not have advanced healthcare training—have a comparable duty to respond is under-explored. No previous work explicitly addresses whether local health department employees consider a duty to respond, nor what trade-offs may be in the balance when making a decision to respond. If there is evidence that a duty to respond is a duty that resonates with local health employees, promoting such a duty may enhance willingness to respond.
As part of a larger project to identify and consider competing ethical commitments and their relationship to the willingness of local health department staff to respond to an infectious disease outbreak, we conducted focus groups to explore concerns and values of local health department workers if they were asked to respond to an infectious disease emergency.
Methods
We conducted focus groups with senior and frontline local health department staff to gather descriptive information about their concerns and values if asked to respond to an infectious disease emergency. Our analytic goal was to identify competing commitments staff may encounter in making a choice to respond. We used the focus group method to collect information about a range of topics and take advantage of the fact that sharing of information in a group setting sparks additional thoughts from participants. Our work was reviewed by the Institutional Review Board (IRB) of the Johns Hopkins Bloomberg School of Public Health and determined to be exempt from IRB review.
Recruitment
We conducted 2 sets of focus groups in 2014. We worked with the National Association of County and City Health Officials (NACCHO) to identify eligible participants. Our goal was to conduct 2 focus groups with local health department administrators and 2 with frontline local health department staff. The first 2 focus groups were conducted in conjunction with the NACCHO Preparedness Summit held in April 2014. In advance of the summit, the NACCHO chief of preparedness sent an email on our behalf to 260 registrants, announcing our plans to conduct 2 focus groups during the summit and asking interested individuals to contact our study team. Our goal was to create 2 focus groups of 10 to 12 participants each. We received 129 responses and scheduled 10 participants and 2 alternates for each group.
The second set of focus groups was conducted in conjunction with the NACCHO Annual Meeting in July 2014. We used an alternative recruitment method, posting and distributing flyers on site and listing a phone number at which we could receive calls or texts regarding interest in participation. In this manner, we were able to accrue our sample.
Focus Group Guide
The focus group guide was developed based on a review of the literature, past work of the study team, and the study team's knowledge of the relevant issues. The guide was reviewed by an expert advisory committee we established to provide feedback to the study team during the life of the project. The committee included local (Baltimore City and state of Maryland) and national experts in: public health practice, pandemic preparedness, law, ethics, and organizational management. The focus group guide was semi-structured. We had questions under each of our key domains but did not repeat questions verbatim or follow the order in which they appeared in the guide, but rather brought up questions and probes as the focus group progressed. 15 The focus group guide had 2 key domains of interest: (1) concerns and values related to willingness to respond, and (2) barriers and facilitators to willingness to respond (see supplementary material for focus group guide: https://www.liebertpub.com/10.1089/hs.2018.0046).
Key questions in the concerns and values domain included:
What commitments do people have that might lead them to come to work during an infectious disease outbreak? How do people make a decision about whether to go to work during an infectious disease outbreak?
Key questions in the barriers and facilitators domain included:
Why might someone decide to come to work during an infectious disease outbreak? What types of commitments, if any, should local health departments have to their employees' families during an infectious disease outbreak?
Data Collection
Two members of the study team (HAT and LR) served as moderator and note-taker, respectively, for each focus group. In advance of the focus groups, a disclosure form was reviewed with the participants, and their agreement to participate was confirmed. At the end of each focus group, each participant was asked to complete a simple set of professional and personal demographic questions. The focus groups lasted approximately 70 minutes (51 to 89). Each participant was given a $50 Amazon gift card as a thank you. All focus groups were digitally recorded and transcribed by the study team. Transcriptions were verified, and all potentially identifying information redacted.
Data Analysis
Transcripts were open coded and key themes identified. A thematic summary was produced for each focus group. These 4 summaries were then combined to create a master summary on which the coding scheme was based. The coding scheme was created by one author (HAT) and reviewed by a second (LR). A matrix was created in Microsoft Word to facilitate the coding and organization of relevant narrative text. The left column of the matrix listed primary codes from the coding scheme. The right column included text excerpts and sub-codes applied to the text.
One author created the matrix (HAT) and it was reviewed by a second (LR). Discrepancies in domain classification and sub-codes were discussed and resolved. Below we first describe findings relevant to the type virus responsible for the outbreak to which a department may have to respond. The rest of the findings focus on the description and relationship among the competing ethical commitments local health department staff encounter when making a decision about whether to respond to an infectious disease outbreak. In what follows we use the term “staff” to refer to all individuals employed by a local health department. When relevant, we use the term “employee” to distinguish from leaders of the department (ie, senior staff, directors).
Findings
We present below perspectives from our participants on how the type of virus responsible for the outbreak may affect their willingness to respond, how local health department employees learn about and articulate their professional commitment to the department, the ways in which local health department leaders support local health department employees' ability to respond to an outbreak, and how local health department staff articulate their responsibilities to their families.
Demographics
We collected key demographic information from focus group participants. We had 46 participants, more than half of whom were women (n = 28; 61%); 13% were nonwhite (n = 6), and 63% had advanced degrees (Table 1). Thirty-six participants (78%) self-identified as having leadership positions in their respective departments as either directors or senior staff, and 10 (22%) self-identified as local health department employees (Table 2). One focus group included only department leaders, 1 group was employees only, and the other 2 included both department leaders and employees.
Demographics
Among the nonwhite participants were 2 black/African Americans, 2 Asian Pacific Islanders, 1 American Indian/Alaska Native, and 1 other.
Professional Category of Participants
Type of Virus
Across the 4 focus groups, a few participants reported they were veterans of post-9/11 efforts to vaccinate healthcare workers for smallpox, and many had responded to the H1N1 epidemic in 2009-10.16,17 While we were interested in and documented their experiences with these efforts, we pushed the participants to consider how they might respond (or how staff from their health department might respond) to an active infectious disease outbreak in which the viral agent was likely to result in high rates of morbidity and mortality (more like smallpox than H1N1). That is, we asked them to imagine what their own response might be as well as that of their colleagues.
In response, group members identified the amount of uncertainty about the infectious agent (and whether a vaccine or treatment is available) (n = 13), transmissibility (n = 10), and severity of disease (n = 9) as key factors that would affect their willingness to respond. Specifically, the greater the uncertainty, likelihood of transmissibility, and severity of disease, the less likely local health department staff would be to respond. This phenomenon was well described by a supervisor:
You know, I think we all have the plans and the training and the staff and all of that stuff in place. But to me we're kind of talking about 2 different situations. One I'm just going to define as the typical relatively low-risk situation that you're in 99% of the time. Where you know, you might catch the measles and get sick or something, but the probability of dying or having serious disability or somebody in your family dying or having serious disability from that or the flu or something is pretty low. And then you've got your other scenario, which frankly most health departments have never experienced, which is an entirely different conversation, and so, I think we can guess about how people are going to respond when there's a disease in the community that's 80% fatal and we're asking people to go out and take care of that on the front lines.
While many indicated their departments were ready to respond to an outbreak of a common disease for which there is a vaccine, responding to a novel virus with a high fatality rate would be a different story. Respondents imagined willingness to respond to decline with the level of uncertainty, high rates of transmissibility, and severity of disease. Given the timing of our focus groups, the topic of the Ebola outbreak in West Africa came up as an example of such a virus, but the Ebola epidemic was only in its early stages.
Response Expectation
Almost half of the participants indicated that all local health department employees in their jurisdiction would be expected to respond to an infectious disease outbreak (n = 19). Table 3 presents the variety of ways an employee may learn of the expectation to respond.
Ways in Which Expectation to Respond Relayed
Participants noted that, in some cases, employees might learn about the expectation of response in more than one of the ways listed in Table 3. A couple of participants noted that there might be a discrepancy between the percentage of staff local health department leaders believe are ready to respond compared to the percentage of staff that believe they are ready to respond. In other words, while employees are notified about the expectation to respond, they may not appreciate exactly what they are expected to do and/or what their role might be during a response.
Two participants noted that local health department leaders are responsible for supporting the ability of the employee to respond. Adequate education and training are needed for employees to have the ability to respond. Relatedly, participants recounted instances when employees refused to participate in training and drilling activities. Failure to participate in these activities impairs the ability of employees to respond during an actual outbreak. Of note, 3 participants mentioned that an employee who fails to show up for a response might be fired. One participant indicated that this had happened to a nurse who failed to respond during a norovirus outbreak.
Finally, participants referred to 2 sources that would predict the likelihood of some employees being more likely than others to respond to an infectious disease outbreak. The first was a reference to a commitment to public health (n = 18). Half of the participants who mentioned commitment to public health referred to it as a positive attribute (ie, why someone would respond), while the other half referred to it as a reason why some staff members may not respond to an infectious disease outbreak (ie, they lack a commitment to public health). On the former, a senior staff member commented:
We draw a certain set of standards for folks. You don't go into public health if you don't want to help. I don't see that. I see most of the public health folks, it's not just a job, it's something they want to do. And that's where, this can't be a job. It has to be something that you live for and do. Because it [infectious disease outbreak response] doesn't happen on a regular basis. … Public health is 24/7. When the things happen, you just have to have that mindset to you. You know, it's like having to walk away from home to go spend 2 days in a response or it could be weeks at a response.
Second, 5 participants referred to the fact that some employees belong to professions that have a professional code. Both physicians and nurses, for example, have professional codes that would support their commitment to the welfare of individual patients, if not to a population of patients.
Supporting Ability
Participants described a variety of methods by which department leaders attend to the ability of local health department employees before, during, and after an outbreak. Providing and supporting education (n = 4), training (n = 6), and drills (n = 7) in advance of an outbreak are examples of how leaders can prepare employees for their role and responsiveness during an outbreak. Investments in these abilities happen as a component of preparedness and planning activities supported by the local departments. The delivery of these opportunities can build confidence among those who will be asked to respond. Of the latter, 1 participant said about drills:
I think just the set up that we have in place in general. Because we have drilled it and we talk about it all the time. So, there is a “comfortability” with … how we would proceed if anything ever happens. Just being familiar with the process that, although we had to use it during H1N1, but outside of that we've never really had to use any large scale. But just knowing that if we need to do this, we absolutely can do this. I mean you can't anticipate the fear in the situation, but aside from that, having plans in place that you are comfortable with. … So, just having all those things in place. Making sure everybody knows what their job description is and what is expected of them and everyone else is comfortable with it.
A few participants (n = 3) noted that they believed that having responded to an actual disaster (of any sort) made it more likely that an employee would respond to the next disaster.
As described by our participants, the actual planning and delivery of education was often the responsibility of the designated preparedness staff at the local health department. Preparedness staff can range from 1 individual who has preparedness as a component of his or her everyday responsibilities to a division within the local health department dedicated to this activity. The number of employees dedicated to preparedness at a given local health department was described as relative to the size of the department and/or the size of the population served by the department (likely also a function of funding available to support these activities). While local health department leaders have a role in allocating the necessary funds to support these activities, a number of participants highlighted the advantage of the leaders of the department conveying their personal support for preparedness efforts (n = 7). One staff member noted:
I think that's been the first key to us has been, getting our director's support. So, the 2 things mainly that we've had is training, whether that be previously or on the job. Whatever it may be, it's got to be good. And secondly, it's got to be fully supported by the director. And if it's not via job description, via y'all listening, because if it's not, then you're barking at the wind is what you're doing. So, I mean it really doesn't set in well without that upper management support, and I think that some agencies that don't have that, they struggle. They can write a whole lot of plans that get nowhere.
Our participants also described the ways in which leaders can support the ability of employees to respond during an infectious disease outbreak. The most common method mentioned by participants was attention to “spelling” employees (n = 6)—that is, providing breaks during and between shifts. Attending to the length and frequency of shifts to which employees are assigned during the outbreak response is important to ensure that employees have adequate rest. The next most common method was the importance of providing psychological support on-site to employees responding to the outbreak (n = 5). The third most common way leaders supported the ability of employees to respond was assuring priority access to vaccines, prophylactic medication, and/or medication to treat those exposed during the outbreak (n = 4). Of note, 2 of the participants who mentioned the importance of providing priority access to vaccination for employees noted that departments should be cautious about publicly disclosing priority access to responders for fear of some backlash from the public. Finally, a few participants mentioned provision of personal protective equipment (PPE) as a method of supporting staff's ability to respond to an outbreak (n = 3). PPE is essential to minimize the risk to those responding. In the words of a director:
I think the agency has an obligation in infectious disease to protect their employees. So, it's easy to say when you're hiring somebody, yes, I'll be there 24/7 when you need me. It's a little different, I know when H1N1, at first all the unknowns with that, we had good responses, we went on and things happened. But I think you have, when you demand people to come in for something like a serious infectious disease, you have an obligation to them not just to call and say you're required to be here. And if agencies realize that and prepare for that, and you've got your PPE and you've got your education, and sometimes it will be “no.” I cannot put my staff in danger to do that, and you have to be able to make those decisions at a higher level.
Related to the importance of leadership noted above, 1 director noted that, during a response,
I try and let my staff know that wherever they are, whatever they need, I'm there for them. I will walk on fire. If they need me to walk on fire, by God, I'll try and do it. And that instills in them, then, the same feeling that they would do for me. Lead by example kind of thing. So, if they see me wanting to do that, then they're more willing to take a deep breath and say, you know, I really would not rather go take care of this smallpox, but [name of director] is there, she's putting herself at risk, all I could do is help her. She needs me.
This quote also relays the importance of team building as it relates to successful response to a disaster.
Related to the ways leaders can support employees' ability to respond, 3 participants mentioned the importance of providing priority access to vaccines and medications to the immediate family members of employees asked to respond. Doing so would acknowledge that it would be hard for employees to respond to help those in need if they were concerned about the health and safety of their family.
Once the outbreak is over, another way leaders can support employees' long-term ability to respond is to conduct “hotwashes” or feedback sessions. Five participants noted that these sessions are opportunities to share and learn about what worked well and what did not. Soliciting feedback conveys a commitment to quality improvement and an interest in having the next outbreak response be better than the last. The assumption here is that any improvements would benefit the community at large as well as the health and safety of local health department staff. No participants mentioned attention to staff mental health and well-being as a component of these feedback sessions.
Family Responsibilities
Participants were asked to comment on the caretaking responsibilities staff have and how that may affect their ability to respond to an infectious disease outbreak. A number of participants mentioned ways in which having dependent children may affect their ability to respond (n = 9). About half indicated that those with dependent children will want assurances that their families will be safe during the response (n = 4), and another half added that parents may be reluctant to leave home knowing if they return they may expose their family to the infectious agent (n = 5). Four participants highlighted the fact that response may be especially hard for those with young children. One participant noted:
Sometimes it depends on the age of your staff. We have in our department several individuals who have young children at home. School age but yet younger that aren't able to stay by themselves. And that has impacted the way that they were able to respond. And so, if you have a health department staffing that's primarily people over a certain age where their kids are teenagers they can sort of go their own way. But people with younger children, they are much less flexible. And you don't want them to. … Daycare isn't always the answer unless you have a lot of 24-hour daycares available. But that is a concern.
Two participants added that ability to respond may also be affected if staff have responsibility for older relatives who are dependent in ways similar to young children. Finally, 4 participants mentioned the importance of considering pets as dependents.
Discussion
In summary, about half of the focus group members indicated that all local health department employees would be expected to respond to an infectious disease outbreak. There are a variety of ways that local health department staff are notified of the expectation to respond. In some cases, local health department employees abide by a professional code that encourages response to an infectious disease outbreak. There is concern that not all local health department employees are aware of the expectation that they respond. One way to address this gap is to systematically inform local health department employees and provide the support they need to respond when called to do so.
Focus group members identified a number of ways that local health department leaders can prepare and support local health department employees in responding to an outbreak. A recent survey of healthcare students (medicine, nursing, pharmacy) found that having received disaster training predicted higher willingness to respond to an infectious disease outbreak. 18 In addition to assuring that local health department employees receive role-appropriate knowledge and skills in advance of an outbreak, there are other ways local health department leaders can support employees' ability to respond during an outbreak, such as providing adequate materials and supplies as well as access to postexposure prophylaxis (eg, vaccines). Extending access to family members may also facilitate willingness to respond. In reference to family, local health department leaders need to anticipate and address local health department staff concerns about the safety of their family members.
In their qualitative interview study of international healthcare workers responding to the Ebola epidemic in West Africa, Gee and Skovdal found that a number of social factors attenuated risk perception among frontline responders, including institutional trust (Médicins sans Frontières, in this case), duty of care, and humanitarian ethos. 19 They also found that worry about family members reduced willingness to respond. The authors concluded that the roles of fostering trust, taking care of health workers, and taking care of families ought to be addressed in advance of and during an outbreak as well as being the object of further research in enhancing willingness to respond.
Given our descriptive findings and building on the ideas shared in Gee and Skovdal, we conclude that there are at least 4 overlapping sets of commitments relevant to local health department staff willingness to respond to an infectious disease outbreak (Figure 1). In presenting these proposed commitments, we want to encourage further discussion that may lead to ways to help local health department staff understand the networks of commitments they have and to assist these agencies' leaders to acknowledge and foster these commitments to enhance the willingness of staff to respond to an infectious disease outbreak.
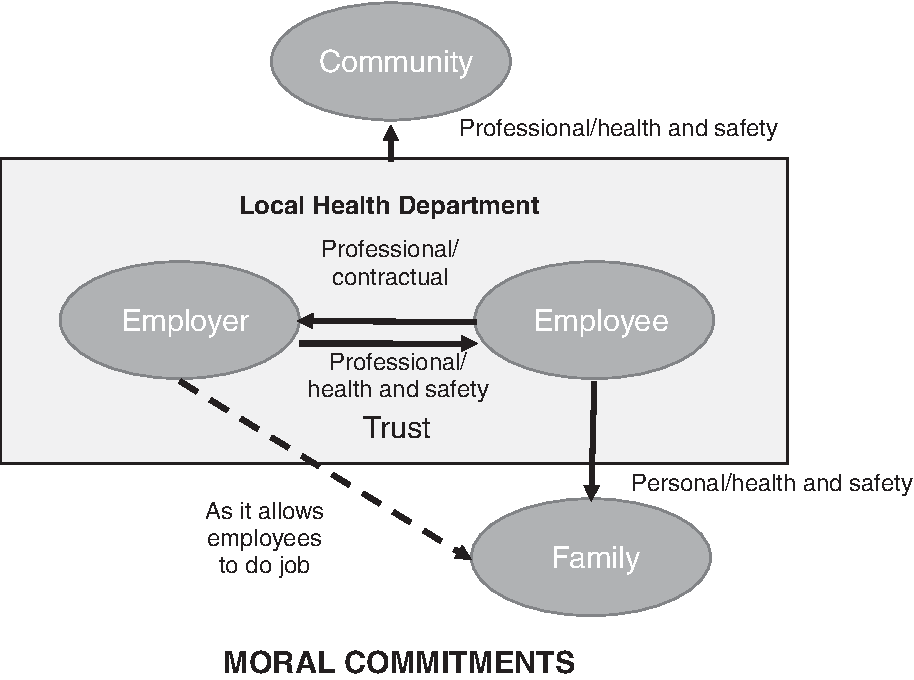
Commitments Relevant to Local Health Department Staff Willingness to Respond to an Outbreak
In the background of any response led by a local health department, or which the local health department is a part of, it is assumed that as a public social service agency, the local health department has a professional commitment to the health and safety of the community it serves. A commitment to social justice, a core principle of public health, requires that the local health department may have a particular obligation to the health and safety of the least well off in the community. 20 It is the staff of the department that acts on this commitment, fulfilling their varied professional roles and responsibilities. Responding to an infectious disease outbreak is one of many activities the local health department engages in to promote the health and safety of the community. 21
As depicted in Figure 1, within the local health department (inside the large shaded box), the director (or equivalent) has a professional commitment to the health and safety of employees. We propose that being as clear as possible with employees about what their role and responsibilities may be during an outbreak; supporting employees with the appropriate education, training, and drills to make sure they can fulfill their role and responsibilities; and guaranteeing access to preventive and therapeutic interventions and essential equipment is how this commitment is best conveyed. It is by being supportive in these ways that department leaders can foster trust among employees. By extension, as depicted by the dashed line, departments have professional commitments to the health and safety of their employees' families. Providing priority access to clinically preventive and therapeutic measures for families may facilitate staff response. Local health department staff have a professional commitment to fulfilling their specific role as a member of the response team. While it may be the fact that the strength of professional commitment varies by job description or title, if it is the case that the department cannot meet its commitment to health and safety of the community unless the entire department responds, this needs to be made clear to all staff. When there is an expectation that some or all employees are required to respond to an infectious disease outbreak, this ought to be made clear in a systematic way to all employees and formalized in a way that is easily understood as well as repeated at regular intervals.
Finally, local health department staff have a commitment to the health and safety of their families. Local health department leaders need to consider this commitment when forming expectations about employee willingness to respond as well as considering actions that may support this commitment. As shared by our focus group members, supporting the families of staff will allow employees to focus on their professional roles and responsibilities during an outbreak. A commitment that we did not hear much about in the focus groups was the commitment local health department employees have to their colleagues. This is either related to the way we asked our questions, and/or it was not a commitment at the forefront of their minds when considering the impact of their willingness or unwillingness to respond to an infectious disease outbreak. Future research ought to explore whether local health department employees think of their colleagues when considering their willingness to respond and whether a commitment to their colleagues could be enhanced as a way to increase willingness to respond.
It is inevitable that the commitments described above will come into conflict. Even for those professionals who have chosen public health as a career because it allows them to play a role in the health and well-being of a community and who are well educated in terms of their roles and responsibilities during an infectious disease outbreak, an internal conflict may likely exist between their professional duty to serve and commitment to the health and safety of their family. The leaders of the local health department must consider how best to assure the health and safety of their employees and their families to support staff willingness to respond. While the leaders have no control over the severity of the agent or outbreak that may occur, they ought to consider the knowledge, skills, and resources as well as social needs of their staff in advance of and during an infectious disease outbreak. As 1 staff member concludes:
I think one of the things you hit on. That people are still fearful. And I think that oftentimes will override whatever policies are in place. A lot of people. If you are worried about your own well-being, or your life or your family, your families' lives, you are not going to worry about your job over that. Most people I would imagine would say, my job is not worth my life. And that's just kind of the reality of the way I see it. We could write any policy we want.
The findings of this qualitative exploration have some limitations. First, while we were able to recruit local health department staff from across the country and describe a diverse set of experiences and opinions, our findings are not generalizable to a national sample. Second, we recruited from attendees at 2 national conferences. We conducted our focus groups at the conferences to facilitate face-to-face interaction and capitalize on the value of the focus group method. Participants' attendance at the conference highlights both their commitment to the field as well as the fact that their local jurisdiction has the funds to support their attendance. Both bias our sample toward those more able, and perhaps more willing, to respond. Third, many of those who volunteered to participate in our focus groups may have a professional and/or personal interest in infectious disease outbreak response and therefore represent the experience and opinions of a subset of local health department staff.
Conclusion
Despite the limitations of our findings, we believe they lead to a series of next steps in a research agenda. First, as noted above, commitment to fellow employees did not come up in the focus groups. We hypothesize that such a commitment might exist if local health employees were asked directly about their role and responsibility as it relates to their co-workers. A focus group or in-depth interview study could be designed to answer this question. If it does exist and resonate with employees, it could be added to the overlay of relevant commitments. In addition, there may be other commitments not yet identified. There may also be nuances about the commitments identified that should be explored further. These questions could also be further explored with a qualitative study.
A next step in the research agenda would be to see if and how any of these commitments are relevant to how a local health department employee might articulate a duty to respond during an infectious disease emergency. A quantitative study could be designed to measure the strength of these commitments using vignettes to force respondents to choose 1 commitment over another or rank their commitments. Findings from this study could be used to design interventions to make local health department staff aware of these commitments and anticipate how they may affect their willingness to respond to an infectious disease emergency. The findings could also be used by health departments to prioritize investment in particular resources to maximize employee ability to manage what will likely be competing commitments when it comes time to decide whether to respond to an infectious disease outbreak.
A final suggestion would be to explore whether and how any of these commitments play out in disasters other than infectious disease outbreaks. We would hypothesize that the majority of this could be transferable to disasters involving chemical or radioactive compounds, where there is a clear physical risk to responders and special protective equipment is required. Some of these commitments may be relevant to other types of disasters and/or to other types of responders. Their applicability is worth pursuing. Pursuit of these and other questions can lead to ethically informed decision making and processes in local health departments to optimize public health surge capacity amidst a broadening array of infectious disease threats.