
Abstract
The Ebola epidemic of 2014 demonstrated that outbreaks of high-consequence infectious diseases, even in remote parts of the world, can affect communities anywhere in the developed world and that every healthcare facility must be prepared to identify, isolate, and provide care for infected patients. The Nebraska Biocontainment Unit (NBU), located at Nebraska Medicine in Omaha, Nebraska, cared for 3 American citizens exposed in West Africa and confirmed with Ebola virus disease (EVD). Symptom monitoring of healthcare workers caring for these patients was implemented, which included twice daily contact to document the absence or presence of signs of fever or illness. This article describes the symptom monitoring experience of the NBU and local and state public health agencies. Based on lessons learned from that experience, we sought a more efficient solution to meet the needs of both the healthcare facility and public health authorities. REDCap, an open-source application used commonly by academic health centers, was used to develop an inexpensive symptom monitoring application that could reduce the burden of managing these activities, thus freeing up valuable time. Our pilot activities demonstrated that this novel use of REDCap holds promise for minimizing costs and resource demands associated with symptom monitoring while offering a more user-friendly experience for people being monitored and the officials managing the response.
This article describes the symptom monitoring experience of the Nebraska Biocontainment Unit and local and state public health agencies. REDCap was used to develop an inexpensive symptom monitoring application that could reduce the burden of managing these activities. The pilot activities demonstrated that this novel use of REDCap holds promise for minimizing costs and resource demands associated with symptom monitoring while offering a more user-friendly experience for people being monitored and the officials managing the response.
The Ebola epidemic of 2014-15 demonstrated that outbreaks of high-consequence infectious diseases, even in remote parts of the world, can have an impact on communities anywhere in the developed world and that every healthcare facility must be prepared to identify, isolate, and provide care for infected patients. Another outbreak in 2018 in the Democratic Republic of the Congo reminds us that the threat of future outbreaks continues. 1
During the 2014-15 outbreak, the Centers for Disease Control and Prevention (CDC) developed guidance for preventing healthcare-associated Ebola transmission, including policies and processes for symptom monitoring and management of healthcare workers who care for infected patients. 2 Symptom monitoring is defined as an assessment for symptoms at regular intervals of individuals who have cared for or been exposed to a patient with an infectious disease but are not yet ill. The individual is immediately isolated if symptoms are detected. Quarantine is the physical separation of an individual who was exposed to a communicable disease. Symptom monitoring and quarantine are important nonpharmaceutical interventions to prevent disease transmission, particularly if chemoprophylaxis, therapeutic medications, or vaccines are not available for a pathogen. Symptom monitoring, with or without quarantine, has been shown to be an effective strategy for containing emerging disease threats such as Ebola and SARS and will likely be a key intervention in the future. 3
During 2014-15, symptom monitoring recommendations for healthcare workers caring for patients with Ebola virus disease (EVD) in US healthcare facilities included twice daily contact to monitor for symptoms and document fever checks throughout the care continuum and continuing 21 days after the last exposure. This article describes the administrative burden experienced by 1 US facility—the Nebraska Biocontainment Unit—in monitoring healthcare workers caring for patients with EVD and an inexpensive, efficient strategy to reduce this burden that meets the needs of the facility and public health authorities.
The Nebraska Experience
In 2014, the Nebraska Biocontainment Unit (NBU), located at Nebraska Medicine, a large academic health system in Omaha, Nebraska, cared for 3 American citizens exposed in West Africa and confirmed with EVD. Prior to CDC's releasing guidance for monitoring healthcare workers in US hospitals, the NBU had already admitted its first EVD patient and implemented staff monitoring with both physical examination and daily phone calls. The monitoring data were initially tracked on paper, but the process quickly became a time-intensive task that involved validating completeness and timeliness of reporting, following up with staff who were not on duty daily or who had not reported, and continually checking the reported information for evidence of symptoms. In addition, the data were submitted daily via secure email to the local and state health departments for submission to CDC.
In an early effort to reduce the administrative burden, Nebraska Medicine developed an electronic database system accessible internally on the hospital's intranet that improved ease of analysis and reporting but was difficult for staff to access while off-site. While this system represented a great improvement, managing it still required substantial staff and leadership intervention. NBU leaders spent a great amount of time each day monitoring data and calling healthcare workers who had difficulty accessing the symptom database. Data sharing and reporting to public health agencies was also cumbersome. Local public health staff reviewed reports that were exported from this system daily and sent by secure email. Local public health staff entered daily symptom data line-lists into the Nebraska Electronic Disease Surveillance System (NEDSS) to facilitate aggregate reporting to CDC by the state health department. Both of these early systems captured the necessary symptom monitoring information and met functional needs, but both were extremely time intensive for an already overburdened group of NBU healthcare practitioners and administrators and public health agency partners.
Use of REDCap to Improve Efficiency
As the Ebola crisis waned in West Africa, Nebraska Medicine and its academic partner, the University of Nebraska Medical Center, the Douglas County Health Department (DCHD), and the Nebraska Department of Health and Human Services (NDHHS) convened to identify more efficient processes and to conceptualize an automated system for monitoring healthcare workers. Funding from Nebraska's Public Health Emergency Preparedness (PHEP) Supplemental Ebola cooperative agreement was leveraged to identify and customize a system. REDCap (Research Electronic Data Capture) is a secure, internet-based application designed to support data capture for multiple uses, such as multi-center data collection projects and web-based surveys. This application has been installed in hundreds of academic institutions, hospitals, and public health departments throughout the world and provides an intuitive interface for validated internet-based data entry and a secure database capable of capturing and handling personal health information if it is installed in a HIPAA-compliant environment. 4 The system provides a user-friendly platform to quickly set up and maintain data collection “projects,” which can include automated survey invitations for collecting data directly from respondents. Such REDCap “projects” are a collection of database tools that provide database management, data collection, and analysis customized for a specific data collection activity.
Data can be entered into a REDCap project either by REDCap users who are securely logged in to the system or via a built-in internet-based survey tool that can be set up to automatically email respondents an access link. When clicked, the link takes participants directly to the online questionnaire. Information entered into the questionnaire automatically populates each participant's record. Survey invitations can be set up on schedules to collect similar information from participants repeatedly over time, and the system can be programmed to send automatic reminders if responses are not provided within predefined parameters. Data in REDCap projects can also be easily shared with authorized users over the internet.
Based on the experience during the NBU activation, our objective was to reduce the burden of symptom monitoring on healthcare practitioners, administrative staff, and public health agency partners by adding automated reminders and alerts. Because REDCap is open-source and readily available, several health departments and hospitals across the United States used it to develop monitoring projects for their Ebola preparedness and response efforts. Many of these early adopters shared their experiences with other health departments on webinars and conference calls and offered their project templates through the Project REDCap website (projectredcap.org). Although REDCap contains some built-in reporting and alert functionality, such features are not specific to user-defined triggers, such as report of a fever or specific symptom of concern or failure to respond to a scheduled symptom monitoring survey request. As a result, users needed to access, download, and analyze data multiple times each day in order to detect symptoms in a healthcare worker in a timely manner. After reviewing multiple projects, we opted to use a project developed at Vanderbilt University Hospital as a starting point for our project. 5
The University of Nebraska Medical Center (UNMC) has an established REDCap infrastructure that is used for both clinical and basic science research. The UNMC REDCap system uses Secure Sockets Layer (SSL) encryption and is hosted in a HIPAA-compliant environment. The system is accessed over the internet by approved users with a user ID and password. Access was granted to UNMC's REDCap system for both DCHD and NDHHS public health staff for the purpose of assessing whether it could be used for public health practice and, specifically, for monitoring of healthcare workers exposed to Ebola.
The project was completed in 2 phases. In phase I, the Vanderbilt REDCap project was customized to conform to local policies and processes. Twenty-five people, including nurses, physicians, transporters, environmental staff, and public health officials who had participated in the actual activation of the NBU, tested the phase I system by submitting initial contact information and twice-daily symptom reviews for 3 days. In phase II, feedback from the phase I test was gathered, and computer programming was used to enhance the “out-of-the-box” functionality of REDCap to improve the system based on the feedback.
Initial REDCap Project Setup
The NBU REDCap project was set up with web-based survey data collection enabled. Four instruments were created: healthcare worker preregistration (for enrolling healthcare workers), healthcare worker contact information and exposure (for gathering initial contact preferences of the healthcare workers and risk assessment), and 2 daily symptom reviews (1 for morning and 1 for evening). The healthcare worker preregistration instrument was designed to be populated by importing a spreadsheet with a list of all healthcare workers to be monitored. The healthcare worker contact information and exposure instrument and the daily symptom reviews were set up as surveys that are completed by the healthcare workers being monitored. The automated survey invitations are triggered by populating the preregistration instrument. A view of the daily symptom review survey from a mobile browser is shown in Figure 1. REDCap interfaces with an email server to facilitate email invitations and reminders. Automatic email survey invitations for morning and evening were created and scheduled to be sent every 24 hours. Because there is no automatic alert functionality in REDCap, data would need to be downloaded at least 2-3 times per day for analysis and identification of positive symptom reports and healthcare worker nonresponse. Statistical analysis software (SAS®) was needed for creating a view of responses to thoroughly assess for completeness and symptom status.
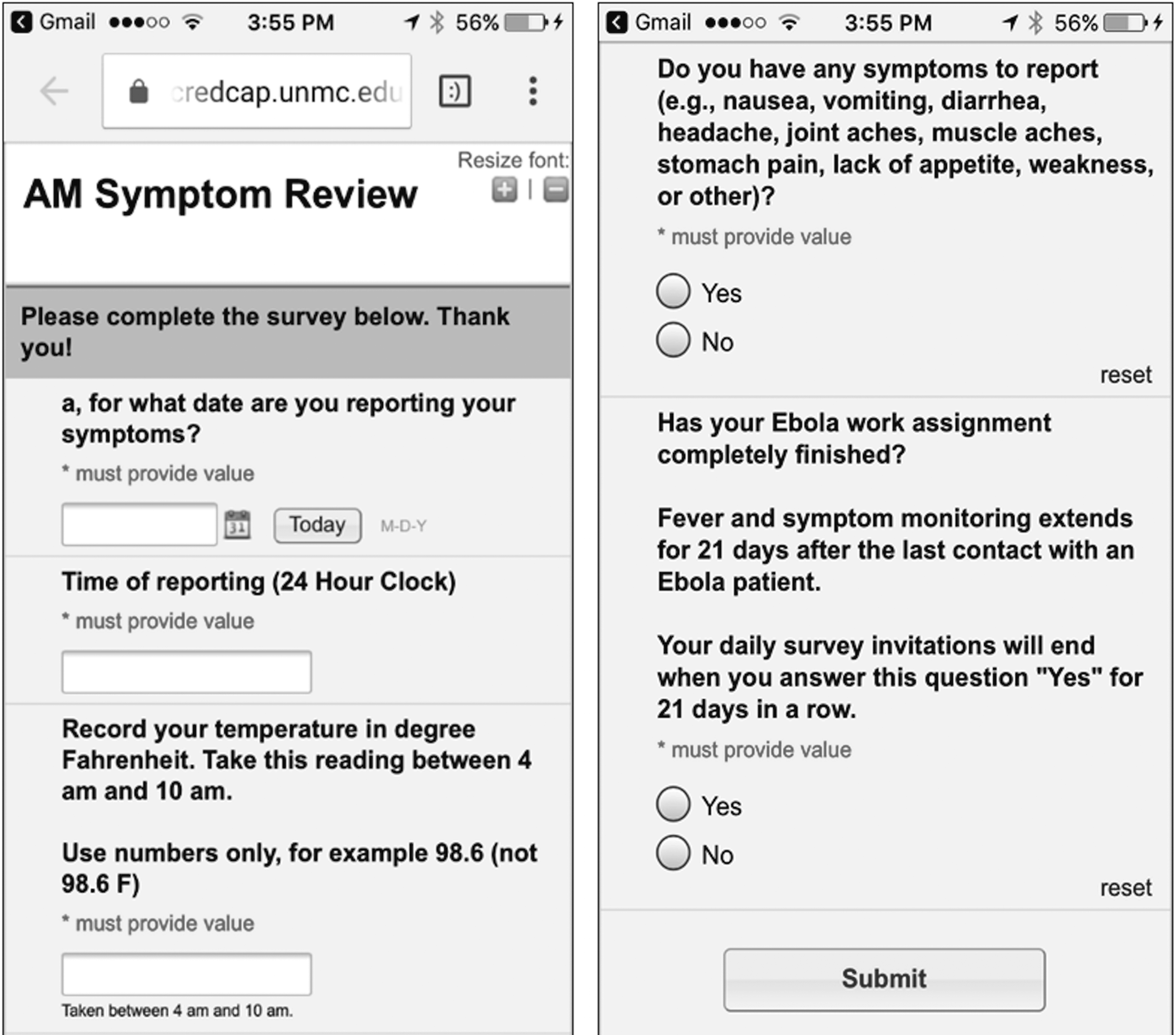
Mobile symptom review form
Phase I Testing
Staff from DCHD, NDHHS, and NBU piloted the project by asking several NBU team members to participate as if they were being monitored for several days. Staff and NBU management noted the ease with which the fever checks and symptoms (or lack thereof) could be reported twice daily through the form accessed directly from the emailed link. It was also much easier for NBU and public health officials to monitor and share data. However, staff reported that it would be difficult to access email twice daily, especially on days off. Ensuring that all healthcare workers were entering all symptom information twice a day was also cumbersome because it still required accessing REDCap several times daily to download data and run customized SAS reports to identify nonresponse or positive symptoms. Symptom monitoring information was also being manually entered and tracked in the state's disease surveillance system (NEDSS) because no processes were established to electronically transmit REDCap data to NEDSS. The key enhancement requested by NBU management and healthcare workers was to deliver the automated reminders and alerts by text message in addition to or instead of email.
Project Enhancements
After several weeks of meetings between system users and the computer programmer, a detailed use case to describe the functionality needed for enhancement of the project was developed (Table 1). Each step of the use case is described with the business need/action, use case requirement, current functionality of REDCap, added programming or systems needed, and actions required by both healthcare workers being monitored and NBU management staff. Automation was used to the greatest extent possible in order to minimize the burden on both groups.
Use Case and Requirements for the REDCap Ebola Healthcare Worker Monitoring System
Note. NBU = Nebraska Biocontainment Unit; REDCap = research electronic data capture; SMS = short message service (cellular phone text messaging).
A separate REDCap project served as a monitoring control panel for entering names and contact information for staff who will be receiving alerts for healthcare worker symptoms and nonresponse. Perl, a free programming language (https://www.perl.org/) familiar to web developers and system administrators was used to add automation of reminders and configurable symptom alerts. Reminders were configured to re-send symptom reporting invitations to staff if they did not enter their symptom review data within 4 hours. Reminders were sent as an email invitation (Figure 2) and as a text message (Figure 3). If staff did not submit their symptom review after 3 reminders, a message was sent to NBU management, who would then reach out to the nonresponding person (Figure 4). In addition to these reminders, an alert message was configured to notify NBU management immediately if a staff member reported fever or symptom(s) (Figure 5). The message also included a phone number to contact the staff member directly without having to log in to the database. Text messaging of reminders and alerts was accomplished by subscribing to an inexpensive cloud-based text message service. In the event of internet outage, a modem was configured to send text messages as a backup.
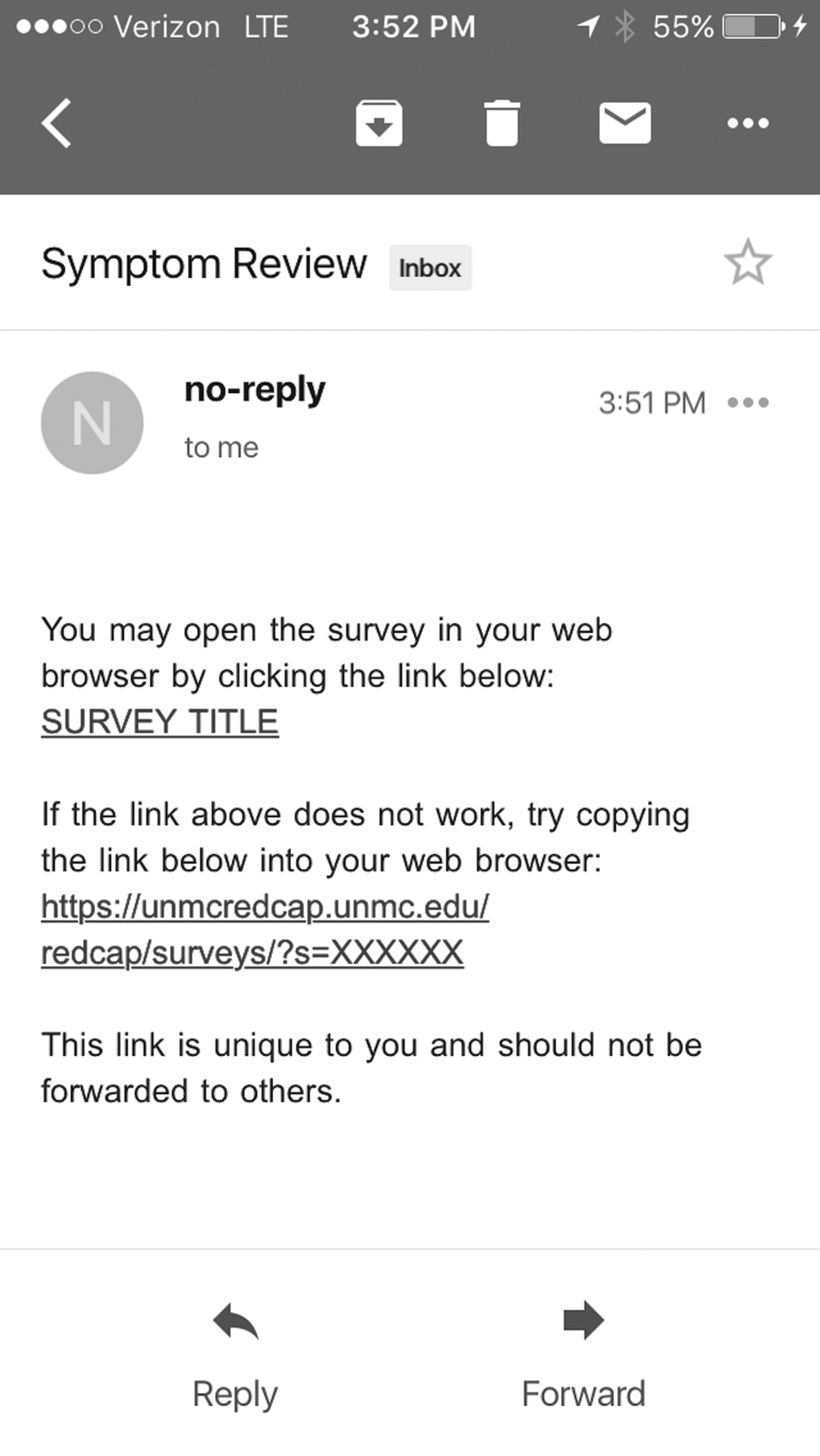
Email reminder to monitored staff
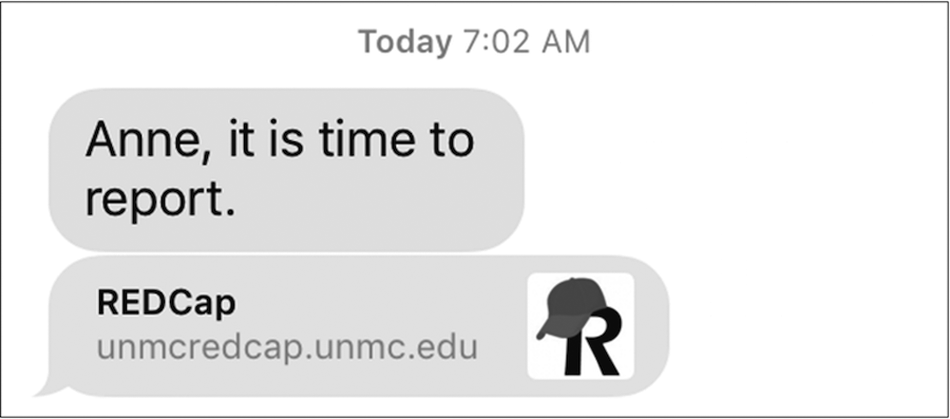
Text reminder to monitored staff

Alert to management for staff nonresponse
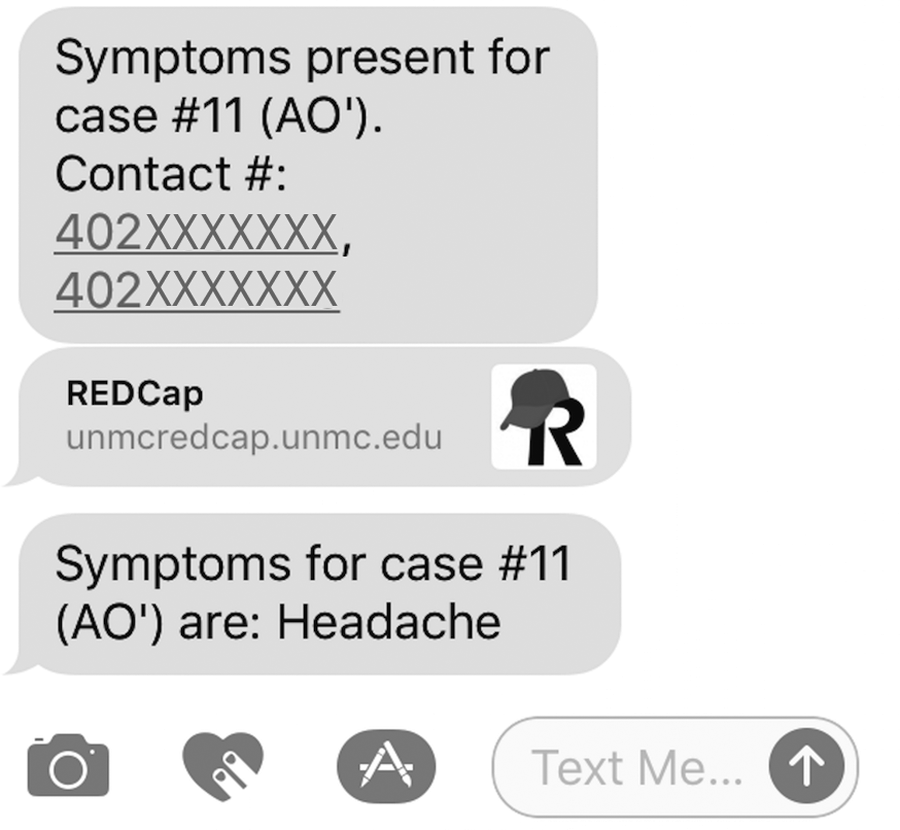
Text symptom alert to management
Post-enhancement Testing
After the phase II system enhancements were completed, the system was tested again with 7 NBU and public health staff. Testers reported that responding to a text message and filling out the symptom review on a smart phone was much more convenient than checking email twice daily. The burden of daily data review and reporting was also eased for NBU management team members because of the automatic alerting functionality included with the enhancements. Additionally, state and local public health officials were granted secure, user-authenticated access to the data, which provided immediate, on-demand access to the monitoring data (ie, NBU management no longer had to provide reports).
Conclusion
Upon completion of phase I, we successfully developed an automated system leveraging REDCap infrastructure to register and enroll healthcare workers for symptom monitoring, capture contact information, establish contact preferences, complete a risk assessment, and administer twice daily symptom reviews. To optimize efficiency and usefulness in phase II, we further enhanced the system by incorporating automated text message reminders and alerts. This enhanced system holds promise to ease the burden on healthcare workers being monitored and eliminate the need for NBU management staff to access and review data multiple times daily. Further, by granting project access directly to public health officials to facilitate data review, NBU management will no longer need to generate daily reports and provide them via secure email. Both NBU management and public health officials in Nebraska are prepared to deploy this new system in the future as needed for healthcare worker monitoring upon activation of the NBU to provide care for patients with EVD or other high-consequence infectious diseases. The REDCap project template, without text reminders and alerts, can be easily shared and imported into other REDCap systems. However, programming for text reminders and alerts needs to be configured by information technology staff who manage the REDCap installation being used. A future enhancement being considered is an automated secure data transfer to send healthcare worker monitoring data from UNMC's REDCap system directly to the state's public health disease surveillance system (NEDSS) to further improve efficiency by reducing the data entry burden of public health staff.
Preparing to care for patients with high-consequence infectious diseases such as Ebola presents an ongoing and costly challenge for hospitals. In 2015, a nationwide survey of general acute care hospitals in the United States noted that the average cost to prepare for caring for patients with EVD was estimated to be $80,461 on the basis of supplies and overtime costs alone. 6 This estimate did not account for the administrative burden and information technology costs involved with developing systems for monitoring of healthcare workers who cared for patients with EVD or other high-consequence infectious diseases or actually deploying such systems during a real event. As evidenced by our pilot activities, enhanced and novel use of a commonly available open-source application such as REDCap can help minimize costs associated with symptom monitoring while offering a more user-friendly experience both for the people being monitored and the officials tasked with managing the response.
Footnotes
Acknowledgments
This project was supported by CDC Public Health Emergency Preparedness funding provided to the Nebraska Department of Health and Human Services, with sub-award funding provided to the University of Nebraska Medical Center. The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention. Use of trade names and commercial sources is for identification only and does not imply endorsement by the Centers for Disease Control and Prevention, the Public Health Service, or the US Department of Health and Human Services.