
Abstract
The use of investigational therapeutics in the care of patients with Ebola virus disease was documented in the literature following the 2013-2016 outbreak. In order to access these types of therapeutics, facilities must have processes in place to quickly and efficiently activate study protocols, obtain the medications, and administer them in a timely manner. Testing these procedures in advance of a real-world event is crucial to ensuring successful implementation and execution. Drills and exercises are routinely used as part of the emergency preparedness planning process, as they provide a low-risk environment in which to test plans and procedures. Including research activities in full-scale emergency preparedness exercises is a novel approach that should be considered when creating a comprehensive special pathogen program. One important aspect of creating an agile response program is developing and sustaining strong relationships with key collaborators. Including departments not previously engaged in infectious disease preparedness exercises provides a forum to strengthen these relationships, clarify roles, and identify gaps. This article describes the process used to incorporate research-centric objectives focused on the use of investigational therapeutics for Ebola virus disease into a full-scale exercise, the evaluation process used to measure the identified objectives, and the results of the exercise.
This article describes the process used to incorporate research-centric objectives focused on the use of investigational therapeutics for Ebola virus disease into a full-scale exercise, the evaluation process used to measure the identified objectives, and the results of the exercise.
Drills and exercises in emergency preparedness play a vital role in national preparedness by facilitating community stakeholders' testing and validation of plans and capabilities. The drill or exercise can be used to help identify capability gaps in order to create plans for improvement in the areas tested. A well-designed exercise provides a low-risk environment in which to test capabilities, familiarize personnel with their roles and responsibilities, and foster meaningful interactions and communication across organizations. 1 For any locality, the rarity of major public health emergencies necessitates the use of practice-based exercises to simulate real-life experiences in order to develop and improve skills and to assess response capabilities over time. 2
In order to take advantage of the small window of time available to acquire meaningful clinical data and have a positive impact on patient outcomes in infectious disease outbreaks, a research team and its many stakeholders must be ready to implement research operations in a way that minimizes the impact of emergency response and clinical care that often accompany rare, sporadic events. 3 Including research activities in full-scale emergency preparedness exercises is a novel approach that should be used when creating a comprehensive special pathogens program.
We define a special pathogen as a highly infectious, highly contagious, and highly hazardous pathogen that produces severe disease in humans, such as Ebola virus disease. 4 Defining characteristics of a special pathogen can include an association with high morbidity or mortality, or both; a high likelihood of secondary cases (person-to-person spread); the absence of an effective vaccine, prophylaxis, or treatment; and a pathogen for which clinical or public assuredness concerns might prompt the use of a biocontainment unit. This is particularly important in preparing to manage patients with special pathogens in venues such as biocontainment units, where very few medical countermeasures are FDA approved.
During the 2013-2016 Ebola virus disease outbreak, in light of the paucity of available treatments, multiple investigational therapeutics—including monoclonal antibody, ZMapp™—were introduced into treatment regimens to augment supportive care in an effort to minimize morbidity and decrease mortality rates.5,6 Continued development of vaccines and novel treatment options for Ebola and other special pathogens have increased the need for biocontainment units to develop and maintain the ability to rapidly implement and systematically conduct research protocols.
In 2016, the Department of Health and Human Services (HHS) Office of the Assistant Secretary for Preparedness and Response (ASPR) provided funding to the National Ebola Training and Education Center (NETEC) to develop this capability. 7 The Special Pathogen Research Network (SPRN) was initiated as a resource under NETEC to support research at the 10 regional treatment centers in the United States, including a central rapid response institutional review board (IRB), biorepository, data repository, common policies and procedures, training resources, and readily available subject matter experts. 8 SPRN was established in large part as a recognition that the hectic attempts to efficiently and systematically operationalize the conduct of research and data collection during the 2013-2016 Ebola virus disease outbreak fell short.
Incorporating the procurement, delivery, and administration of an investigational therapeutic adds both depth and complexity to the traditional patient transport and clinical admission exercise. This element allows the care team to work through the very real challenges of including investigational therapeutics into the suite of treatment options and delivery of care for Ebola virus disease and other special pathogens (Figure 1). NETEC and the SPRN, in collaboration with HHS/ASPR, Mapp Biopharmaceutical, Inc., and the Regional Ebola and Other Special Pathogen Treatment Centers (RESPTCs), incorporated these elements into a full-scale exercise that was conducted during April 2018.
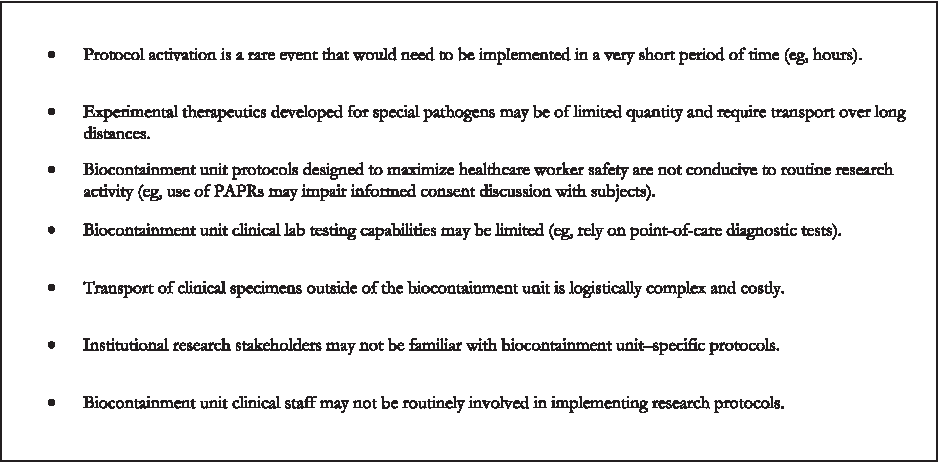
Specific Challenges Associated with Incorporating Research Protocols into Biocontainment Unit Activation
Tranquil Terminus was a 4-day, multistate exercise funded by HHS/ASPR that tested the nation's ability to move patients with Ebola virus disease and other special pathogens safely and securely from diverse domestic healthcare facilities to RESPTCs throughout the United States. The exercise involved more than 50 local, state, regional, federal, private sector, and nongovernmental organizations, focusing on the notification processes, coordination decisions, and resources needed to move patients with Ebola, using both air and ground transportation resources to move 7 simulated Ebola virus disease patients to 4 RESPTCs within HHS/ASPR regions IV, VI, IX, and X. The exercise began on April 9, 2018, and concluded on April 12, 2018. This article discusses the planning, execution, and outcomes centered on the incorporation of the use of investigational therapeutics in the treatment of patients with Ebola virus disease as part of a national full-scale exercise.
Methods
Exercise Design
The investigational therapeutics objectives incorporated into the Tranquil Terminus exercise were developed based on the findings of a previous exercise conducted in the Nebraska Biocontainment Unit (NBU). This initial full-scale exercise was part of a state-based comprehensive activation and transportation exercise conducted in May 2016 and, to our knowledge, was the first full-scale exercise that integrated research capabilities for Ebola and other special pathogens.
Building on the Nebraska Biocontainment Unit's findings, Tranquil Terminus was designed to engage multiple stakeholders who were identified as key partners in the execution of the defined objectives related to research and investigational therapeutic capabilities (Table 1). The RESPTC activation triggered the initiation of a rapid response IRB, as well as the procurement, delivery, and preparation of investigational therapeutics. These components were considered to be critical elements of the exercise at the participating RESPTCs.
Exercise Objectives and Core Capabilities
To facilitate the design and conduct of this portion of the exercise, a distinct exercise planning team coordinated by NETEC focused on the research components, in addition to the larger planning team that focused on the more global identification, facility activations, and transport of the simulated patients. The individual teams' efforts were then coordinated and aligned by the designated team leaders and the acting exercise directors at each of the RESPTCs via email and planning meetings.
NETEC subject matter experts developed a complementary suite of exercise documents and templates based on the Homeland Security Exercise and Evaluation Program (HSEEP) relating to the research component, the exercise plan, the communications plan, exercise evaluation guides, the master scenario events list, and the after-action report or improvement plan. 1 When customizing the exercise scenario and objectives, consideration was given to the after-action report from a previous Nebraska Biocontainment Unit exercise, the Hospital Preparedness Program (HPP) Ebola Preparedness Measures,7,8 and each participating agency's focused objectives. These research objectives were integrated into the primary exercise master scenario events list. The global exercise planning committee, led by HHS/ASPR, initiated planning meetings months in advance and met regularly to define the key elements that needed to be addressed in the exercise. The overarching design, conduct, and evaluation of this exercise benefited from collaborative planning that involved personnel from each participating organization.
Two meetings were conducted to determine the priorities for the concepts and objectives to be addressed, define objectives based on those priorities, align exercise objectives with core capabilities, and identify exercise planning team members in each participating facility and agency. The first meeting focused on the feasibility of integrating the identified research components into a complex full-scale exercise to include: (1) the intended scope of the research capabilities, (2) the capacity and willingness of the RESPTCs to participate and implement an existing protocol for the administration of ZMapp™, (3) the activation of the central IRB-approved protocol from the University of Nebraska Medical Center (UNMC) IRB for the existing ZMapp™ protocol, and (4) the ability of Mapp's vendor to ship mock ZMapp™ vials to 4 RESPTCs during the exercise.
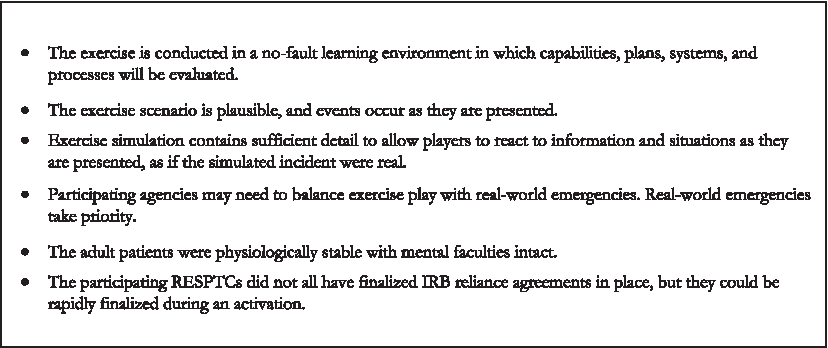
The second meeting focused on further developing the research components to be included in the exercise. Included in the discussion was the activation of facility-based rapid response IRBs to review a new protocol, the implementation of an existing protocol for the administration of ZMapp™, and the integration of a central IRB at UNMC. Because the exercise was planned during the time when the RESPTCs were in the process of activating their sites for the ZMapp™ clinical trial and moving toward fully executed central IRB reliance agreements, the exercise planning team acknowledged and accepted the artificiality that reliance agreements were not actually in place (Figure 2). Subsequent meetings for exercise development were held at regular intervals with both planning groups in parallel to ensure alignment of exercise timelines and objectives.
Exercise Assumptions
Exercise Scope
The research focus for this exercise was divided into 2 phases during the planning and execution processes. The first phase focused on facility-based systems of coordination, which included identifying and admitting individuals with Ebola virus disease who were eligible to receive ZMapp™, followed by initiating the process to procure ZMapp™. The emphasis during this phase of exercise play was on the research objectives and included the timely identification, notification, and coordination processes to obtain investigational therapeutics for patients confirmed as having Ebola virus disease (Table 1).
At this juncture the second phase of the exercise was initiated; it addressed the receipt of mock ZMapp™ vials by the RESPTCs. Well-defined steps for receipt, reconstitution, and preparation of the medication were provided by Mapp Biopharmaceuticals, Inc. (Mapp Bio) and included measurable objectives for both internal and external processes. It was during this phase of the exercise that integration of the established ZMapp™ objectives were emphasized (Table 1).
Exercise Execution
Assumptions and Artificialities
In any exercise, assumptions and artificialities are necessary to complete exercise play in the time allotted and account for logistical limitations. Exercise participants accept that assumptions and artificialities are inherent in any exercise, and awareness of these allow the exercise to proceed as planned. The exercise assumptions (Figure 2) and artificialities (Figure 3) were communicated to exercise participants in advance. The controllers and evaluators provided reinforcement of these concepts at each participating site as needed during exercise play.
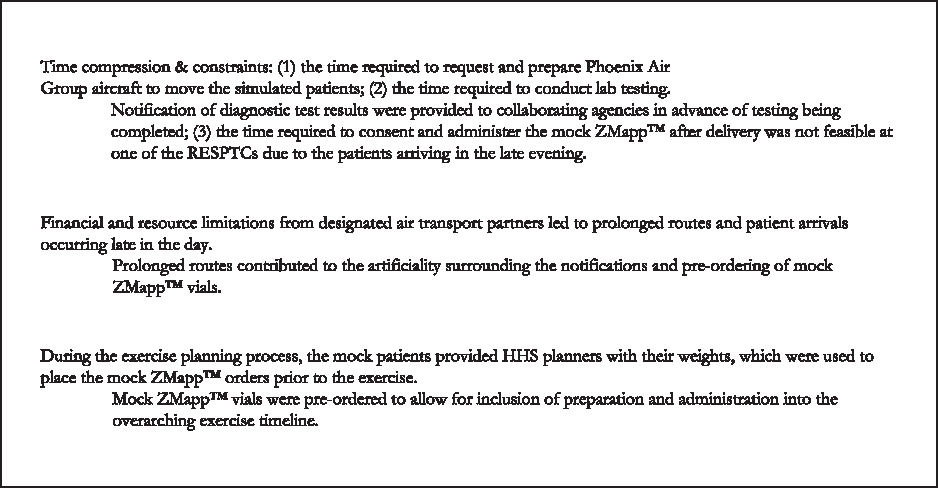
Exercise Artificialities
Conduct
The Tranquil Terminus exercise included numerous global and agency-specific objectives related to the identification, transport, and admission of simulated patients with Ebola virus disease not included in this discussion; however, the scope and timing of the larger exercise construct directly affected the capabilities being addressed here. There were multiple distinct clusters of EVD patients who originated from 5 different locations across the United States and were subsequently transported to designated receiving facilities for treatment, 4 of which were RESPTCs. These RESPTCs each received at least 1 patient during the exercise who met the criteria to activate the ZMapp™ study protocol. Once they received notification of the need to activate their respective biocontainment units, the RESPTCs were asked to initiate the process to receive ZMapp™. Each of the RESPTCs were familiar with the current study protocol and were given the opportunity to clarify any issues or concerns with operationalizing the protocol with Mapp Bio and the NETEC SPRN in advance of the exercise.
Upon receiving the request to activate the RESPTC biocontainment unit for patient(s) confirmed to have Ebola virus disease, each RESPTC proceeded to mobilize its teams for response. Each institution designated personnel to perform the functions needed to initiate the study protocol that were aligned with what their roles would be in a real event. Participating personnel at each site included research pharmacists, nurses, research coordinators, and infectious disease physicians.
The initial action steps and projected timeline for each institution to begin the procurement of mock ZMapp™ were clearly identified in the master scenario events list (Figure 4). The scope of the research component varied by site, based on the anticipated arrival time of the simulated patients. While all 4 RESPTCS requested, received, and reconstituted the mock ZMapp™, only half of the sites opted to exercise the consent and administration processes, due to the late arrival times of their respective patients. Inclusion of the ZMapp™ research protocol in just-in-time training at one of the participating RESPTCs enhanced staff understanding of the consent and administration process despite time limitations that prohibited actual consent and administration of the medication during exercise play.

RESPTC Timeline and Communications for ZMapp Events
Exercise Evaluation
Evaluators with subject matter expertise in the use of investigational therapeutics, research processes, and Ebola virus disease were identified to participate in this exercise. In addition to the global exercise evaluators, each participating RESPTC was also provided at least 1 designated evaluator for research objectives. Evaluators were selected from within NETEC and the Biomedical Advanced Research and Development Authority (BARDA) to fill these roles. Evaluation guidelines (see Supplemental material at https://www.liebertpub.com/doi/suppl/10.1089/hs.2018.0100) previously developed by NETEC were customized and disseminated to each evaluator to facilitate the standardization of data collected. These data were then reported in the hotwash and controller/evaluator debriefings for inclusion in the after-action report.
Results and Discussion
Exercises play a key role in preparedness programs as a means of identifying both capability gaps and areas for improvement. The hotwash is a forum during which facilitators, controllers, and evaluators capture participant perspectives on the key strengths and areas for improvement identified during the exercise. 3 Immediately upon conclusion of the 4-day exercise, participating agencies and facilities were invited to take part in a hotwash facilitated by HHS/ASPR. A representative from each facility was designated and asked to give a brief report using a Plus/Delta process as an evaluation tool to identify what processes worked during the exercise and what processes need improvement. In addition, NETEC conducted an internal evaluator debriefing to focus on global findings as well as observations on the specific capabilities at each site.
The participating RESPTCs reported that incorporating the use of investigational therapeutics into the Tranquil Terminus exercise added immense value. Including research pharmacy personnel, IRB members, and research coordinators not previously engaged in infectious disease preparedness exercises provided a forum to strengthen relationships, clarify roles, and identify gaps. The designated evaluators concluded that the majority of the measurable objectives identified in the evaluation guidelines were satisfactorily met and concurred with the participating sites that the inclusion of a research component in a full-scale exercise for biocontainment unit activations provided valuable insight into use of investigational therapeutics. Participating observers noted strengths related to the use of investigational therapeutics in a full-scale exercise and the ability to leverage relationships between facilities and industry partners to rapidly implement an investigational study protocol.
Key areas for improvement identified during exercise play that were brought forward for consideration focused on the ability of the participating sites to implement the study protocol for investigational therapeutics and the capacity to operationalize the shipment and receipt of the appropriate dose using mock ZMapp™ vials within the defined time frame.
The infrastructure for a central IRB system, with a rapid response capability, is important in order to be able to efficiently activate a clinical trial network in response to a public health emergency such as an outbreak. At the time of the exercise, the central IRB had already reviewed and approved the study protocol and was prepared to provide final execution of the reliance agreements to support each site. One of the 4 sites opted to activate its own rapid response IRB during the exercise, demonstrating that if this was a single site project, or there was a need to review outside of the central IRB during an activation, this alternative approach could be successfully completed. The exercise demonstrated the potential variance in each site and their institutional requirements, thus illustrating the importance of not only having a pre-established network but also exercising its capability in order to identify potential complications in protocol activation. While all sites exercised the activation of the protocol, not all sites yet had reliance agreements between their IRB and the NETEC rapid response central IRB at UNMC in place, which will be necessary in an urgent outbreak setting. By developing and implementing this infrastructure up front, which can require significant effort and time, the ability to rapidly respond to regulatory aspects of a trial on short notice will be greatly enhanced.
The objective for the shipment of mock ZMapp™ vials was for the arrival to occur within 24 hours of the ordering time. In 3 out of 4 sites, that objective was met; the fourth site received their vials shortly after the 24-hour time mark had passed. This was attributed in part to exercise artificiality, as there was a reliance on commercial airlines that had an extended delay during a routine layover; in a real world event, alternative mechanisms to deploy medications could be used, including shipping outside of normal business hours or on chartered flights.
Some of the other areas for improvement identified at participating sites were also attributed directly to the exercise design and identified artificialities during the hotwash. For example, because the mock ZMapp™ was pre-ordered, some of the patients' weights varied from their actual weights taken during the exercise, causing the quantity of mock vials to be fewer than what was required to appropriately treat the patients. In a real world event, medication would not be requested nor shipped prior to verifying the patient's weight with the designated healthcare professional. Two of the mock ZMapp doses were also initially addressed to the wrong address, but this was identified by the receiving site early in the process and rectified in time for the medication to arrive within the 24-hour deadline.
The uncertainties of public health response require a mechanism to respond to outbreaks and emergency situations of any type. The ability to quickly activate a network protocol using a central IRB to stand up the entire network so it is fully prepared to administer available investigational products is exceptional.
These findings were recorded and provided to HHS/ASPR to be included in the formal after-action report. A robust after-action report often indicates a well-designed and executed exercise. Exercises are designed to stress the response system and identify any potential gaps. Each of the areas for improvement identified as a result of this exercise have resulted in actionable steps for those who participated.
Conclusion
The integration of research objectives into infectious disease preparedness exercise efforts demonstrates the value of such an activity and how further developing research capabilities serves to advance the readiness of facilities designated to provide care to patients with special pathogens. In advance of this exercise, most of the RESPTCs had joined the Smart IRB, which is a central reliance agreement mechanism facilitating the overarching reliance agreement between sites, but a limited number had completed the study-specific reliance agreement with the central IRB. The administrative processes required to complete these components were stimulated by the exercise, prompting participating sites to work through study-specific reliance agreements and contracts with the sponsor in order to be at a more advanced state of readiness for the exercise from a regulatory perspective.
The inclusion of research pharmacy personnel, IRB members, and research coordinators not previously engaged in infectious disease preparedness exercises helped to integrate these teams that will need to work together. Preparedness gaps were identified related to the use of investigational therapeutics in the care of patients with special pathogens, and potential solutions were generated to mitigate these gaps and further strengthen these teams. Ongoing scrutiny of the existing therapeutic landscapes for other high-consequence pathogens and support for clinical research networks to conduct studies between outbreaks should help to reduce response times for initiating clinical research in future outbreaks of EVD and other emerging threat pathogens. It is critical that the infectious disease and emergency management communities begin to more routinely consider the inclusion of pertinent research activities into exercise design and conduct. As the ability of facilities designated to provide care for patients with special pathogens advances, the incorporation of investigational therapeutics into treatment and care options should be seen as the new minimum standard of care. Indeed, as the development of medical countermeasures increases, there must be a mechanism in place to not only administer these in a timely manner but also accurately capture relevant clinical data for inclusion in structured studies and future analysis.
NETEC and the SPRN are perfectly positioned to provide support and guidance to advance these aims. The creation of this network, cultivation of relationships with federal and private industry partners, and the use of a central IRB at UNMC are all assets that will benefit infectious disease preparedness efforts in between and during infectious disease outbreaks. Ongoing collaborative efforts should continue to expand the focus of preparedness efforts to include research objectives that further develop relationships among public health agencies, industry partners, and designated treatment facilities. The SPRN component of the federal exercise, including the rapid research protocol activation, was shown to be feasible and successful. Further exercises involving the approval and delivery of experimental medications are needed for the advancement of emerging special pathogen research, medical countermeasure development, and the advancement of national preparedness to manage patients confirmed as having Ebola or other special pathogens.
Footnotes
Acknowledgments
The authors express sincere gratitude to the designated Regional Ebola and Other Special Pathogen Treatment Centers, the US Department of Health and Human Services (HHS)/Office of the Assistant Secretary for Preparedness and Response (ASPR), Mapp Biopharmaceuticals, and World Courier for contributing to the design and participating in the execution of this exercise. The authors would like to acknowledge Chad Connally, BSN, RN, at the University of Texas Medical Branch and Christa Arguinchona, BSN, RN, CCRN, at Providence Sacred Heart Medical Center for their valuable comments and suggestions provided to improve the quality of this article. Funding for exercise activities described in this article was provided by the US Department of Health and Human Services (HHS), Office of the Assistant Secretary for Preparedness and Response (ASPR). The views expressed in this article are those of the authors and do not necessarily reflect the views, assertions, opinions, or policies of the US Department of Health and Human Services.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.