
Abstract
The 2013-2016 epidemic of Ebola virus disease (EVD) that originated in West Africa underscored many of the challenges to conducting clinical research during an ongoing infectious disease epidemic, both in the most affected countries of Guinea, Liberia, and Sierra Leone, as well as in the United States and Europe, where a total of 27 patients with EVD received care in biocontainment units. The Special Pathogens Research Network (SPRN) was established in the United States in November 2016 to provide an organizational structure to leverage the expertise of the 10 Regional Ebola and Other Special Pathogen Treatment Centers (RESPTCs); it was intended to develop and support infrastructure to improve readiness to conduct clinical research in the United States. The network enables the rapid activation and coordination of clinical research in the event of an epidemic and facilitates opportunities for multicenter research when the RESPTCs are actively caring for patients requiring a biocontainment unit. Here we provide an overview of opportunities identified in the clinical research infrastructure during the West Africa EVD epidemic and the SPRN activities to meet the ongoing challenges in the context of Ebola virus and other special pathogens.
The 2013-2016 epidemic of Ebola virus disease (EVD) that originated in West Africa underscored many of the challenges to conducting clinical research during an ongoing infectious disease epidemic. The authors provide an overview of opportunities identified in the clinical research infrastructure during the West Africa EVD epidemic and the Special Pathogens Research Network activities to meet the ongoing challenges in the context of Ebola virus and other special pathogens.
M
The lack of coordinated clinical research protocols during EVD outbreaks led to the use of a wide variety of investigational MCMs, instead of a few that could be well studied. These varied MCMs were all given instead under compassionate use for EVD patients cared for in the United States and Europe during the 2013-2016 epidemic. 2 These included convalescent plasma and whole blood; monoclonal antibodies, including ZMapp (MappBio, San Diego, CA), MIL77 (Mabworks, China), and ZMab (Defyrus, Canada, and Public Health Agency of Canada); direct-acting antivirals such as brincidofovir (Chimerix, Durham, NC), favipiravir (Fuji/Toyama, Japan), TKM-Ebola (Tekmira Pharmaceuticals, Canada); supportive therapies, such as FX06 (MChE-F4Pharma, Vienna, Austria), amiodarone, melanocortin, and various immunomodulators, such as the type I interferons with or without ribavirin; and the live attenuated viral vaccine rVSV-ZEBOV (Merck, Kenilworth, NJ). 2
Clinicians seeking access to investigational MCMs for their EVD patients were faced with limited data on the few available products, relying mainly on anecdotal reports or animal response data to help guide treatment decisions for individual patients. Due in part to the urgency to begin administration of investigational MCMs as soon as possible, as well as the lack of a coordinated research network, efforts were undertaken simultaneously at multiple centers without standardized methods for clinical data collection and specimen collection and storage across institutions. Since most EVD patients cared for in the United States and Europe received multiple investigational therapeutics on an uncontrolled basis, inferences about safety and clinical benefit of specific agents were very limited. This resulted in few opportunities to develop coordinated high-quality clinical trials and advance scientific knowledge about optimal EVD therapeutic regimens. 9 By the end of the epidemic, only 1 patient with EVD who had been cared for in the United States or Europe was enrolled in a randomized controlled trial during the epidemic. 10
In the future, a coordinating body with representation from each of the affected countries would be ideal to determine future protocols and assist in prioritization of these studies. In the current outbreak of EVD, the National Institute of Allergy and Infectious Diseases (NIAID) has taken the lead in working with agencies for prioritization of MCMs included in the 4-arm trial. 11
The Office of the Assistant Secretary for Preparedness and Response (ASPR), the US Food and Drug Administration (FDA), and NIAID, in collaboration with the National Academies of Sciences, Engineering and Medicine, completed a comprehensive evaluation of clinical research conducted during the 2013-2016 epidemic. While the report focused on the EVD research efforts in West Africa, many of the lessons learned are also relevant for other resource-limited countries, including the importance of incorporating research as a core component of epidemic response and the cost-effectiveness of capacity building. 12 Funded by ASPR and coordinated by the National Ebola Training and Education Center (NETEC), the Special Pathogens Research Network (SPRN) was created in the United States in 2016 to provide an organizational structure to leverage the expertise of the 10 Regional Ebola and Other Special Pathogen Treatment Centers (RESPTCs) to develop and support infrastructure in the United States to improve readiness to conduct clinical research during a public health emergency. 13
In this article, we provide an overview of opportunities identified in the clinical research infrastructure during the EVD epidemic, the resulting structure of the SPRN, the activities in the workgroups, and the implementation of an expanded access protocol across the SPRN. Ongoing challenges and opportunities in clinical research are reviewed in the context of Ebola virus and other emerging pathogens.
Clinical Research in the EVD Epidemic
In the United States, access to investigational products during the EVD epidemic occurred via uncontrolled single-patient-use Emergency Investigational New Drug (EIND) authorization from the FDA. 14 Many of these investigational products did not have existing clinical protocols for humans and had limited data available on pharmacokinetics, optimal dosing, and safety in humans. Thus, in many cases, investigational protocols had to be developed by local clinical investigators or the product sponsors in parallel with the EIND process for individual local institutional review board (IRB) approval.
Development of protocols was influenced by uncertainties in the international research community regarding the ethical acceptability of withholding treatments with inadequate prior testing in humans, the ethics of conducting research on a disease with a high case fatality proportion during an emergency, and the optimal study design for assessing countermeasures in a setting in which randomized, placebo-controlled trials (the gold standard of medical research) were not always feasible. 15 The few facilities in the United States with established biocontainment units had to quickly implement new protocols in coordination with their clinical research infrastructure and biocontainment unit clinical staff in the midst of patient care. 16 Furthermore, optimal supportive clinical management of EVD patients was not well-defined prior to the 2013-2016 epidemic. The case fatality proportion of 18.5% for the 27 patients with EVD managed in biocontainment units in the United States and Europe was substantially lower than that for patients managed in West African Ebola treatment units, suggesting that intensive care management of patients with other etiologies of critical illness may be beneficial for patients with EVD. However, many unanswered questions remain about the optimal supportive clinical management of patients with EVD, and ensuring access to investigational MCMs across multiple clinical sites remains a challenge. 17
Despite a lack of preparation for the conduct of clinical research specific to biocontainment units and preexisting coordination of research efforts, organizations and individuals obtained and administered investigational products on an emergency basis for the 11 EVD patients cared for at medical centers in the United States. Although patients did not receive similar MCMs under a common protocol, clinical data were shared in weekly international clinical calls to help inform care of new EVD patients and were subsequently published in the medical literature. 2 This was made possible through both federal and local efforts, as well as private industry participation. Federal agencies, including the Centers for Disease Control and Prevention (CDC), the FDA, the Biomedical Advanced Research and Development Authority (BARDA), the Department of Defense (DOD), and NIAID, coordinated information sharing regarding medical countermeasures and compassionate use, while the FDA provided timely review of EINDs and connected institutions to pharmaceutical companies.
At each institution, emergent implementation of the clinical research occurred: local IRBs met ad hoc to accommodate needs, sponsored programs offices rapidly executed confidentiality disclosure agreements and contracts, research pharmacists developed protocols and procedures for product preparation, staff were trained in product administration and safety monitoring, and case report forms were developed. These efforts were replicated for each MCM at each institution. Biotechnology and pharmaceutical companies shared available data on current investigational MCMs, most of which were not publicly available at the time, and worked closely with federal and local partners to expedite the process. 18
As the epidemic continued, attempts to increase coordination across the biocontainment units grew, leading to multiple federal, academic, and industry partners coming together to discuss potential investigational therapies, clinical care options, and collaborative approaches. Despite these efforts, opportunities for improvement in both process efficiency and research outcomes were evident. The epidemic, however, was on the decline well before controlled trials were launched, limiting the ability to conduct effective and robust clinical trials in the already challenging context of an international infectious disease emergency (Figure 1).
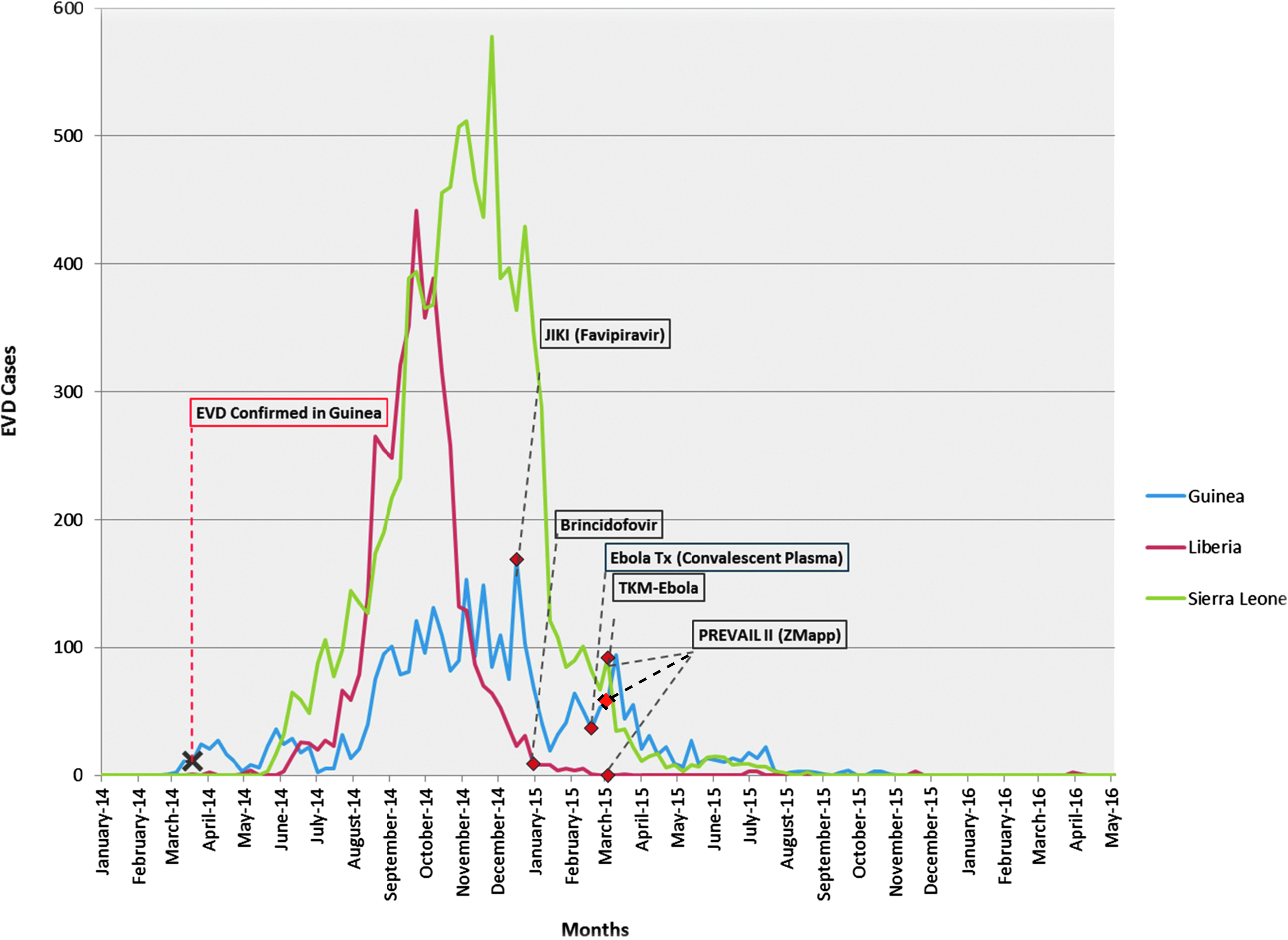
Timeline of Implementation of MCM During 2013-2016 EVD Outbreak
Organization and Mission of the SPRN
In an effort to better prepare the United States to respond efficiently and effectively to future epidemics, NETEC was created to increase the capability of US public health and healthcare systems to safely and effectively manage individuals infected with suspected and confirmed special pathogens 13 (Table 1). When launched in 2015, NETEC was charged with several core responsibilities, including readiness assessment and metric development, education, training, and provision of technical assistance to increase the competency of healthcare and public health workers and the capability of healthcare facilities to deliver safe, efficient, and effective care to patients infected with EVD or other special pathogens. In 2016, NETEC's charge was expanded to include developing infrastructure to support clinical research readiness for future epidemics; the SPRN is composed of the 10 RESPTCs (Figure 2), which are also the institutions that are responsible for providing clinical care in their HHS region.
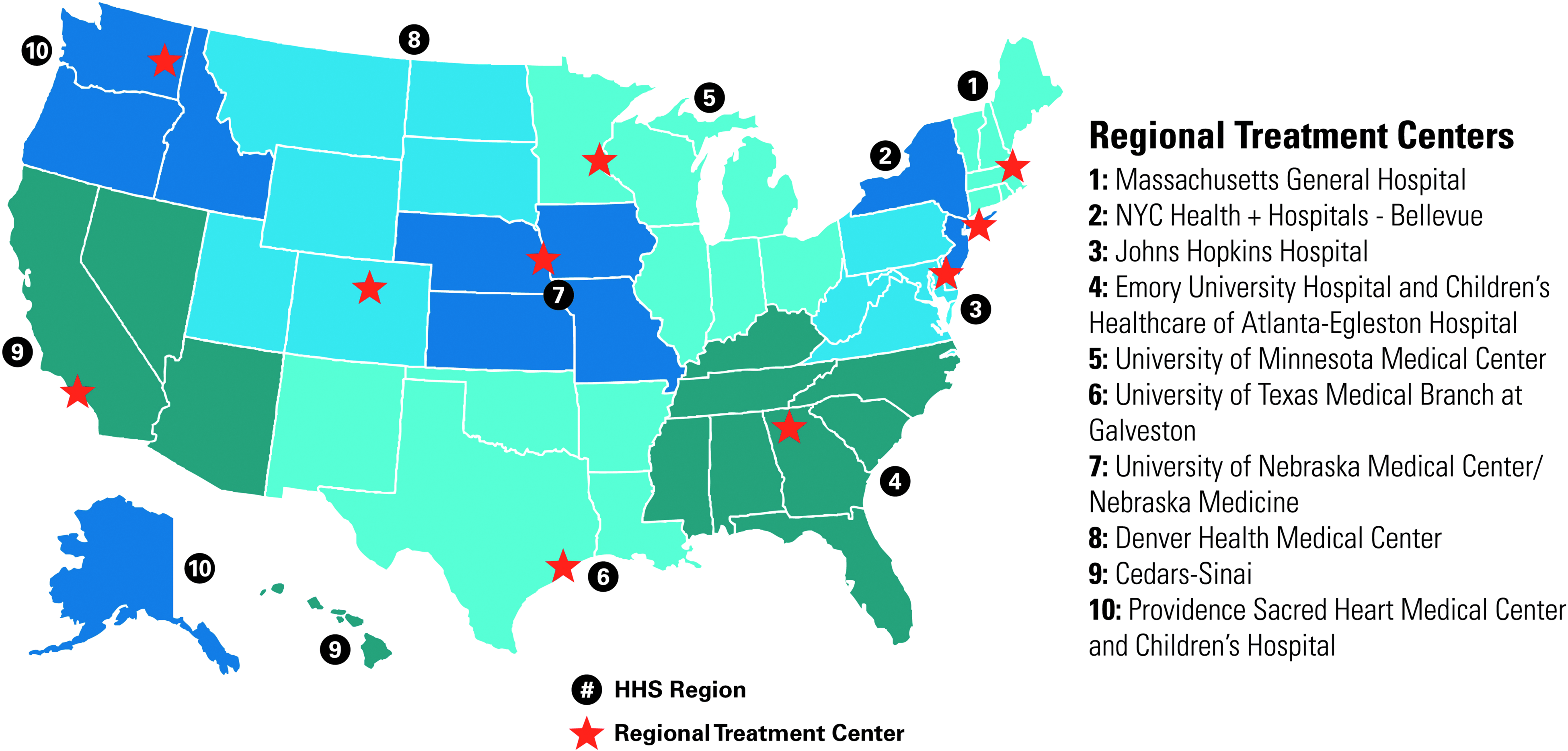
The map depicts the 10 Regional Ebola and Other Special Pathogens Treatment Center (RESPTCs).
List of Potential Pathogens that Could Be Cared for in a Biocontainment Unit (BCU)
Adapted with permission from Corti D, Misasi J, Mulangu S, et al. Protective monotherapy against lethal Ebola virus infection by a potently neutralizing antibody. Science 2016;351(6279):1339-1342.
The SPRN is developing infrastructure through which research can be incorporated into the care of patients at the RESPTCs, with a focus on network engagement, infrastructure readiness, and training readiness. With resources and expertise distributed regionally through these 10 centers, the goal of the network is to markedly improve clinical research readiness for EVD and other special pathogens in the United States.
The SPRN has maintained a close collaboration with federal and other external partners as an extension of the relationships developed during the 2013-2016 EVD epidemic. To facilitate this, the SPRN formed a partner working group with the goal of continuing those collaborations to support better coordination of investigational MCMs. The partner working group, in addition to NETEC membership, includes BARDA, CDC, the FDA, NIAID, the DOD's Infectious Disease Clinical Research Program (IDCRP), and the US Army Medical Research Institute of Infectious Diseases (USAMRIID). CDC, the FDA, BARDA, the Department of Defense, and NIAID provide expertise for the selection of appropriate MCMs, as well as for the progression of MCMs through the research and regulatory pipelines.
Given that individuals admitted to biocontainment units may be infected with Ebola virus or other special pathogens for which there are no licensed treatments, standards of care, or prophylactic options for close contacts or exposed individuals, the MCM working group has focused on assessing the evolving landscape of investigational countermeasures. The goal of the MCM working group is to develop guidance on pathogen-specific therapeutics or prophylaxis measures based on the available supporting scientific evidence and to catalogue the supporting scientific evidence. To acquire this supporting scientific evidence, the MCM working group is assessing existing literature and unpublished findings from federal, academic, and industry partners while organizing the results in reviews that will be designed to provide operational guidance to clinicians during epidemics in any global setting. These include EVD as well as other special pathogens that would utilize investigational MCMs as the primary therapeutic. During the 2013-2016 EVD epidemic, there was a paucity of resources available about potential therapeutics. By contrast, specifically for the current 2018 outbreaks in the Democratic Republic of the Congo, the MCM working group has compiled a status report of investigational MCMs for EVD that were distributed to the NETEC leaders (Table 2). These documents can serve as a template for future MCM summaries for other special pathogens and will be updated routinely as new therapeutics emerge.
Example of NETEC MCM Status Report of Ebola Countermeasures Compiled for the 2018 Democratic Republic of the Congo EVD Outbreaks as a Reference for RESPTCs
The primary deliverable is to document potential MCMs for priority pathogens to inform SPRN research goals; the documents will be available on the main NETEC website. 25 To avoid duplication of effort, the group will liaise with existing groups conducting similar reviews. Public access to these documents will serve 2 purposes: first, they will be a rapidly accessible resource for clinicians involved in the care of people known or suspected to be infected with special pathogens, whether associated with an established RESPTC or not; second, they will be available for researchers to review, which may stimulate ideas for novel or complimentary MCMs.
SPRN Activities
Nine deliverables were created in the SPRN contract in order to benchmark progress in the creation of a network that can support special pathogen research (Table 3). These activities also meet several of the goals and objectives outlined in the 2018 National Biodefense Strategy. 26 They are described below under 3 broad headings of network engagement, infrastructure readiness, and training readiness.
Deliverables for the SPRN as Funded by ASPR/CDC
Network Engagement
All 10 RESPTCs are represented in the SPRN, in collaboration with federal partners. The SPRN has frequent opportunities to accomplish the deliverables, including annual meetings, quarterly calls with the entire SPRN group, and weekly calls for the working group members. Proposals for research studies can be submitted for review to determine whether SPRN members would opt in to participate in a given study.
Infrastructure Readiness
Beginning with the admission of the first patient with EVD, the University of Nebraska Medical Center employed a rapid response IRB that allowed for review of clinical protocols on an expedited timeline, through extensive pre-review of protocols/consents in an iterative process and in close collaboration with the investigators. This was used successfully during the outbreak to review research protocols associated with several investigational drugs and interventions targeting patients with EVD who were hospitalized in the Nebraska Biocontainment Unit at UNMC/Nebraska Medicine. The SPRN central IRB has capitalized on this rapid response model with preexisting signed reliance agreements. These are signed by 2 or more institutions engaged in human subjects research and permit 1 or more institutions to cede review to another IRB, between the other RESPTCs and the UNMC central IRB, and serve to expedite approval of research protocols in emergency situations. Other partners could potentially be brought into the network, as needed, during an epidemic using additional reliance agreements. For example, the SPRN sites currently work with Mapp Biopharmaceutical, Inc. (San Diego, CA) to make ZMapp™ available under an emergency use authorization (EUA) in the event that a patient with EVD is admitted to any of the RESPTCs.
Since there are limited clinical data for humans and many of the MCMs likely to be used in epidemics are in the early developmental stages, human subject protections are critically important when addressing research with EVD and other special pathogens. The SPRN central IRB is acutely aware of special considerations affecting patients hospitalized in biocontainment units and the constraints of conducting research in this unique setting. Obtaining valid informed consent is particularly challenging in the context of serious medical illness; the accompanying fear of death and the lack of approved or alternative treatment options enhance the susceptibility of this vulnerable population to undue inducement and therapeutic misconception. Obtaining informed consent may be particularly difficult if the patient has been transported long distances on an emergency basis, is cognitively impaired, or has few or no family members immediately present to give proxy consent. Even under optimal conditions, additional issues related to risk and benefit, innovative study design, subject privacy, and evolving regulations present challenges for IRBs. The use of a central IRB with experience working through these complexities facilitates the dual goals of conducting ethically compliant research and advancing science.
One of the challenges during the 2013-2016 EVD epidemic was the lack of a standardized protocol to guide the administration of MCMs and prospectively collect clinical data during the course of a patient's illness. Often, since investigational MCMs had never been administered to a human or had only Phase 1 study data, each sponsor company created a treatment dosage in the EIND process with the FDA.
The SPRN protocol workgroup is taking on the development of a master clinical observation protocol that is similar to existing protocols, with the objective being simply to collect and document clinical data in a standardized fashion. This protocol can then be amended to include use of an investigational MCM, all working through the central IRB as described above. Once the master protocol to study special pathogens is written, standardized case report forms with an electronic platform for data collection will be developed. The goal is to standardize the clinical data that are collected at all SPRN institutions, thus allowing data analysis in aggregate. This information will also be available to other institutions if they sign a reliance agreement for the central IRB. Depending on the epidemic scenario, these data may be shared in real time with the affected regions, as was done during the 2013-2016 EVD epidemic.
The ability to collect and store the clinical specimens obtained from patients cared for within the network will provide a significant resource for understanding disease pathogenesis and optimal patient management. Therefore, the SPRN established the biorepository working group to engage with potential partners to develop and maintain a network biorepository. Establishing this capability is challenging given the limited number of facilities that are approved for housing and shipping select agents, especially those requiring biosafety level 4 containment. 27 The biorepository working group continues to develop standard operating procedures for processing and storing specimens from these patients. In addition, the biorepository working group has created a governance structure responsible for prioritizing specimen use by potential collaborators. This was established to ensure a fair, transparent, and safe process for providing access to valuable and likely limited specimens in a way that acknowledges issues of intellectual property rights and resource ownership while encouraging the sharing of resources to optimize research that will have an impact.
Training Readiness
One of the major roles of the SPRN is to ensure that sites have the necessary personnel and skills to administer investigational therapeutics safely and collect data appropriately. Some processes required for conducting research in high-containment environments differ from standard clinical research. Lessons learned from the 2013-2016 EVD epidemic, combined with experienced research teams and exercises, have informed SPRN research training recommendations and tools. Challenges identified among the RESPTCs have included research staff who may not (or cannot) have previously been trained in the use of high-level personal protective equipment (PPE) or, conversely, biocontainment unit clinical staff competent in PPE use who have not been trained in the use of investigational therapeutics or the requirements of research data collection. RESPTCs have different approaches to staffing, with some electing to train research staff to work in the biocontainment unit and others training clinical staff from the biocontainment unit to conduct clinical research, or a combination of both. For sites that need training in the proper use of PPE or research data collection, these resources will be available on the NETEC website.
The SPRN has developed biocontainment unit standard operating procedures to address staffing models and requirements, risk mitigation, informed consent, data collection and documentation, use of investigational therapeutics, handling and local storage of specimens, specimen processing and transport, and activation of the central IRB. These standard operating procedures are available to RESPTCs but do not supersede local policies or procedures, which must comply with all relevant regulations.
The SPRN couples testing and assessment of research readiness with field exercises for special pathogens research. 28 Exercises serve as a cornerstone of the all-hazards approach to preparedness, including for infectious diseases, and are incorporated into local, regional, and national drills. The concept of integrating special pathogens research in the field has not been implemented widely, and much of this insight comes from the experience gained during the 2013-2016 EVD epidemic, including care in resource-rich settings. Annual NETEC site consultations to RESPTC facilities have recently incorporated clinical care exercises during the visits, with options to include activation of the research infrastructure needed to support a scientific evaluation of prophylactic and containment measures, diagnostics, and therapeutics related to Ebola virus and other special pathogens. This has also been drilled in a national exercise funded by HHS, in which implementation of the research protocol for ZMapp™ was included in the field exercise. The complexities of research are well suited to these exercises; the logistics of implementing a new protocol can be vetted during these activities.
Conclusion
The 2013-2016 EVD epidemic provided the first collective experience of managing and using investigational therapeutics for patients with EVD in biocontainment units in the United States. Beyond advancing knowledge and practice in the safe delivery of effective care, the biocontainment units that cared for patients with EVD and the many partners engaged in enabling delivery of investigational products to patients learned valuable lessons. The SPRN is leveraging those lessons and partnerships formed to expand and sustain engagement across the 10 RESPTCs and external partners, to develop research infrastructure for biocontainment units and to establish training readiness to optimize opportunities for clinical research in biocontainment units in the future for national infectious disease priorities.
Footnotes
Acknowledgments
We acknowledge the staff members in our biocontainment units for their hard work, dedication, professionalism, and attention to detail that make our programs successful. NETEC is funded by US Department of Health and Human Services Office of the Assistant Secretary for Preparedness and Response and the Centers for Disease Control and Prevention, CFDA #93.825. The views expressed are those of the authors and do not necessarily represent the official policies of the National Institute of Allergy and Infectious Diseases, the National Institutes of Health, the Centers for Disease Control and Prevention, or the Office of the Assistant Secretary for Preparedness and Response, US Department of Health and Human Services.