
Abstract
I
As part of the response to the incident, government must provide instructions on how the public can inquire about potential victims of that incident (eg, calling a hotline or visiting an ad hoc assistance center set up for that incident). Thanks to the proliferation of smart devices and communication methods, it has become easier for people to let their loved ones know they are safe. However, for those who are injured (or worse, deceased), government must be able to efficiently identify, track, and provide information on these individuals as part of the incident management.
To improve the family reunification process, the New York City Department of Health and Mental Hygiene (DOHMH) has developed a system to simultaneously search multiple hospitals in real-time for reported missing persons. In addition to reuniting people more expeditiously, this system also reduces the case load for law enforcement and reduces administrative demands on the healthcare system during the emergency response.
Challenges with Family Reunification
Government response efforts after a mass casualty incident to help reunite family with affected victims is referred to as family reunification. The process of accounting for victims and connecting them with friends and family requires significant coordination among the responding agencies, receiving hospitals, and inquiring public. 1 Identifying affected individuals can become even more complex when there are multiple hospitals involved and “walking wounded” who self-transport to medical care.
Shortly after any mass casualty incident, government sets up a hotline and, depending on the scenario, a family assistance center to provide services to the friends and family of the victims and/or missing persons. This includes taking information from those who cannot get in touch with loved ones and want to report them as potentially missing because of the incident. This requires a network of dedicated staff and agencies to communicate and investigate the whereabouts of a large number of people. Collecting, sharing, and disclosing the information gathered on victim status presents a significant challenge in the response to a mass casualty incident. Issues such as multiple callers for the same person, delays in initial registration at the hospital, and privacy are all concerns that must be addressed to improve family reunification.
Leveraging Health Information Organizations
The ability to electronically search multiple hospitals simultaneously will significantly expedite the reunification process. This can be done without connecting to individual hospitals, but rather by leveraging organizations known as health information organizations (HIOs), which were created to facilitate health information exchange (HIE). These organizations are also known as regional health information organizations (RHIOs) in some parts of the Unites States.
To address the growing need for sharing health information electronically, regional health information organizations partner with a variety of healthcare providers and public health agencies to facilitate access to electronic health records (EHRs) and securely share them to improve the quality, safety, and efficiency of healthcare delivery. 2 While the development and growth of health information exchange has been ongoing for over 20 years in the United States, the passage of the Health Information Technology for Economic and Clinical Health Act (HITECH Act), which was part of the American Reinvestment and Recovery Act (ARRA), in 2009 created a major new funding opportunity to drive the adoption of electronic health records and health information exchange. 3
For the purposes of family reunification in a mass casualty incident, regional health information organizations capture what is known as health level 7 (HL7) admission, discharge, and transfer (ADT) data, which contain the patient's demographic information (name, gender, address, phone, etc) and location within a healthcare facility (ie, inpatient, outpatient, emergency department, etc). This admission, discharge, and transfer data can be searched in near real-time for the names of individuals who have been reported missing and have been treated at a local hospital emergency department(s), thereby helping law enforcement missing persons detectives to follow up on individual cases.
Regional health information organizations represent several types of healthcare facilities, such as hospitals, nursing homes, and private providers. The search results are limited to those healthcare facilities that participate with a particular regional health information organization—an issue that a jurisdiction must be aware of when planning this capability. It is critical that the regional health information organization represent the ambulance-receiving hospitals in the jurisdiction.
After a mass casualty incident, the public is instructed to call a hotline (or visit a family assistance center, or something similar) to report individuals who may have been affected by the incident and cannot be reached (missing person reports). The size and scale of the incident usually drives the number of missing person reports. During the mass shooting incident in Las Vegas on October 1, 2017, there were more than 3,500 missing person reports filed for the incident. 4 All of these reports had to be investigated and cleared by the responsible authorities in the jurisdiction (eg, the respective law enforcement agency).
Further complicating family reunification efforts was the high number of individuals who self-transported to area hospitals (approximately 80% of patients self-transported after the Las Vegas shooting).5,6 Las Vegas–area hospitals had no notice about the total number of arriving patients or the types of injuries, as they would have had with traditional ambulance transportations. Searching regional health information organizations for information matching missing person reports is most useful in an emergency scenario like the Las Vegas shooting, when first responders do not have complete awareness of all potential victims and when there are multiple hospitals receiving patients across a geographic region. This kind of incident is known as an “open manifest” incident; a “closed manifest” incident is one in which the occupancy or attendance is known. In contrast, during several smaller mass casualty incidents in New York City (eg, building collapses, truck and car ramming incidents), searching regional health information organizations would not be necessary or as useful, since all of the victims and/or the hospital destinations were known.
Current Implementation in New York City
The NYC DOHMH has developed the New York City Emergency Patient Search (NYCEPS) application, a web-based search tool connected to regional health information organizations that serve the NYC metropolitan area. In NYC, there are 49 ambulance-receiving hospitals that are covered by 3 regional health information organizations. DOHMH's search tool has a connection with 2 regional health information organizations to allow patient searches for 42 of the 49 hospitals for the sole purpose of family reunification after a disaster. Because of a technical limitation, DOHMH was unable to connect the New York City Emergency Patient Search (NYCEPS) portal to the final regional health information organizations (which represented the 7 remaining hospitals in the Bronx). However, DOHMH staff were trained and given access to the general provider portal to manually perform searches, if required.
Currently, NYCEPS is set up for health department staff to conduct manual searches using a minimum of 4 data fields. Staff must enter the last name, first name, gender, and date of birth or age range of the reported missing person. In the aftermath of a mass casualty incident in NYC, missing person reports are taken either by 311 hotline operators or in person at a family assistance center and entered into an electronic system called the Unified Victim Identification System (UVIS), the primary disaster management system used by the New York City Office of the Chief Medical Examiner (OCME) and New York Police Department (NYPD) for coordinating activities related to missing persons and victim identification after a mass casualty incident. The health department staff would then look at these reports in UVIS and enter the information into NYCEPS to search for a potential match.
A major technological enhancement is currently in progress between the DOHMH and the chief medical examiner's office to integrate and automate the NYCEPS patient search technology in UVIS to avoid the need for manual searches. Once this is complete, missing person reports captured in UVIS will automatically search the databases of the 3 regional health information organizations for matching patient data. In the event of a match, UVIS will flag and automatically notify the NYPD detectives working to reunify people. This will allow NYPD to quickly follow up with reporting parties regarding a potential match at a specific hospital, thereby reducing the NYPD's caseload and manual efforts required to track down individuals.
Advantages of an Automated Electronic Patient Search
Leveraging regional health information organization data for family reunifications has several key benefits for the public, healthcare system and responder resources, and particularly for law enforcement. First, it could help the public avoid calling and/or visiting numerous hospitals. In turn, it has the potential to reduce some of the burden on hospitals that otherwise would be flooded with walk-in and phone inquiries from the public searching for loved ones, which would allow hospital staff to focus on their core mission of health care. Second, there is no additional data entry required by the healthcare facilities. Finally, it can reduce the queue of missing person cases that law enforcement must investigate and ultimately enable quick reunification of family and friends.
Depending on the jurisdiction's missing person intake system, a manual or automated search may be set up to query regional health information organization data. If there is an electronic intake system (such as UVIS), then it may be possible to automate the search so that as soon as the missing person's information is captured and saved, a search of the regional health information organizations is immediately and automatically triggered.
In the absence of an electronic system for search management, a jurisdiction would need to explore the options to manually search the regional health information organizations (and repeat the search for those who do not match initially). This would need to happen either via the regional health information organizations' public portal or a custom developed portal like NYCEPS. Though potentially helpful, manually searching for what could be hundreds or thousands of missing persons is a staff resource–heavy operation. This further highlights the importance of an application like UVIS, which serves as a centralized repository to collect missing person reports and victim information during an emergency. 7 The UVIS application is a free application developed using Homeland Security grants; a usage license can be obtained by submitting an application to the NYC Office of the Chief Medical Examiner.
During a hospital emergency department patient surge, patient care takes priority over administrative needs, such as entering patient demographic data into the hospital's electronic health records. Often, patients will initially be registered anonymously or under a pseudonym until there is time to determine the patient's real information. Eventually, an unidentified patient will have a real name entered into the electronic health record, but this could happen several hours after admission. Therefore, in the initial hours after a major mass casualty incident, regional health information organization searches could turn up empty even when those people are in the hospital, due to delays in updating the electronic health records. This highlights the importance of automating recurring searches, so that queries are repeated without a human initiation, and having automatic notification of law enforcement personnel working on family reunification.
Adding to the complexity of family reunification is the fact that 1 person may be reported up to 100 times by different people. 8 In the absence of an electronic system like UVIS that can identify and consolidate these duplicate reports into 1 case file, this duplication may cause further challenges and lead to inefficient and redundant work for the responders.
Disclosing Information to the Public
Upon finding a successful match for a reported missing person using the regional health information organization data, law enforcement must reach out as quickly as possible to the reporting party with the potentially helpful information. Once the technical integration is complete with UVIS, a notification will be made to NYPD any time a match is made, allowing NYPD to quickly pull up the case file and contact the searching party to follow up with them regarding the potential match at a hospital (see Figure 1). Determining what to say is at the discretion of the law enforcement agency. For example, does law enforcement want to ask any further questions to confirm the identity of the missing person or to ensure the safety of the patient prior to disclosing the information about the hospital location?
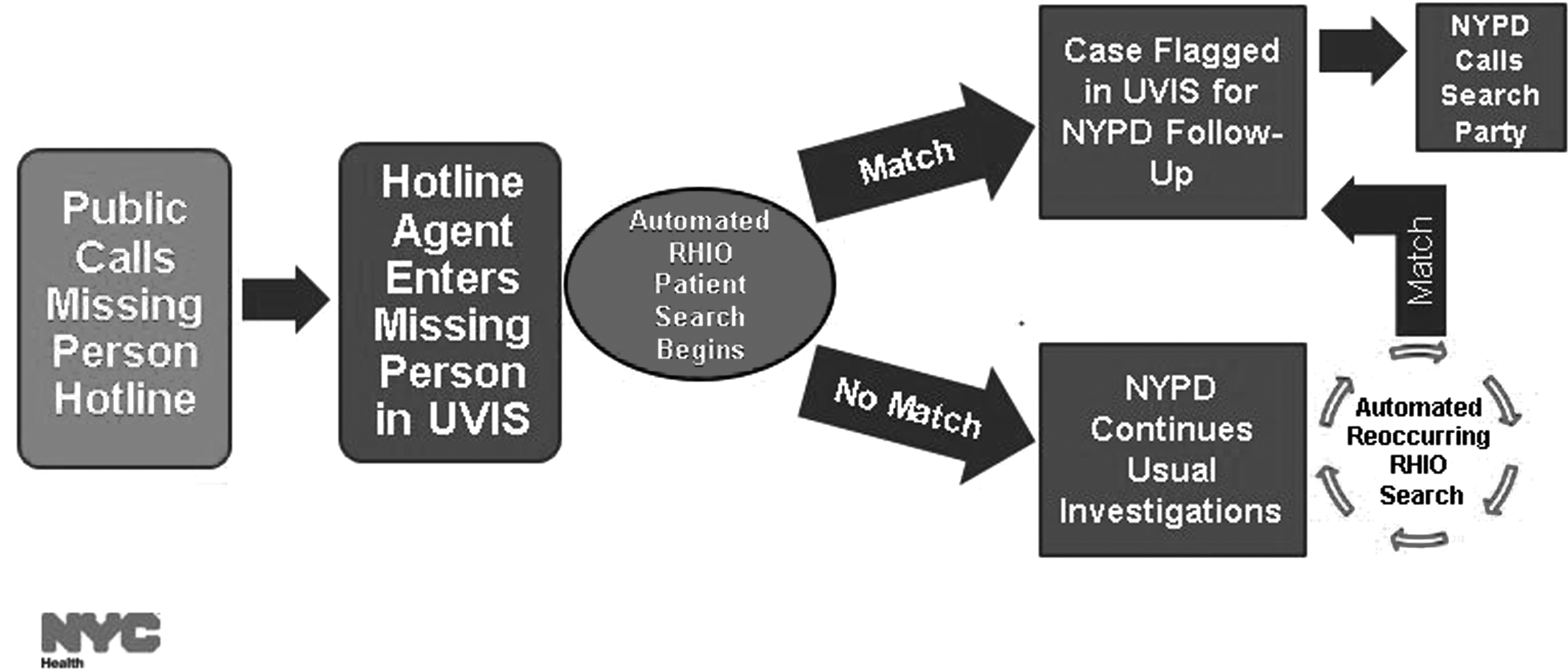
UVIS Real-Time Search.
Legal and Privacy Considerations
Although clinical data from the regional health information organizations are not needed for family reunification purposes (only admission, discharge, and transfer data), any data from an electronic health record (even just the name and location of a patient) is considered protected health information by HIPAA. 9
In New York State, the network of regional health information organizations is governed by the Statewide Health Information Network of New York (SHIN-NY), which is led by the New York State Department of Health with other stakeholders. SHIN-NY policy specifically allows the use of regional health information organization demographic and admission data by “disaster relief agencies” for the sole purpose of “locating patients during an emergency event.” 10 Additionally, even if a patient denies consent for their medical data to be accessible at the regional health information organization, it will still be available for emergency purposes as part of the SHIN-NY policy. Nonetheless, there is still a need for data use agreements between the regional health information organization and stakeholder agencies (ie, DOHMH, OCME, NYPD) to ensure the data are used only for family reunification purposes and no other law enforcement activities (eg, criminal investigations).
Challenges and Lessons Learned
Several issues must be considered in order to leverage regional health information organizations for the purpose of family reunification.
Hospital Coverage
Since regional health information organizations cover local healthcare providers, nursing homes, and other healthcare facilities in addition to hospitals, governments should check the regional health information organizations in their jurisdiction to ensure coverage of ambulance-receiving hospitals, which are most likely to receive patients after a mass casualty incident. When NYCEPS was initially developed, there were several hospitals that were not participating (ie, not sharing their electronic health records system) with any of the 3 NYC regional health information organizations. Eventually, the hospitals did become participants with the regional health information organizations and improved NYCEPS coverage.
Technical Capability
The regional health information organization must be able to receive an electronic query from an external server and return the admission, discharge, and transfer information required. While seemingly a simple technical requirement, development time for the application and query configuration in NYC was significant and required many hours of testing and troubleshooting. Furthermore, one regional health information organization's software was not capable of receiving such an electronic inquiry and was unable to be connected initially, though now a solution is being developed.
Unidentified Patient Naming Conventions
It is also critical that healthcare facilities in a jurisdiction have a standardized naming convention for unidentified patients. Hospitals have unique (albeit similar) naming conventions and associated disaster registration protocols that may not adequately accommodate the high volume of patients in a major incident. At times, the pre-named triage tags meant for surge incidents have resulted in redundant naming and patient care confusion. For example, if a hospital had 100 pre-named tags and they exceeded that number of patients, they recycled the names again.
To avoid this, regional healthcare networks should aim to have consistent naming conventions so that an electronic system (like NYCEPS) can be programmed to automatically pick up on unidentified registrations across the hospital network (via the regional health information organizations) to support family reunification efforts. This will help reduce law enforcement reliance on hospital staff to coordinate and obtain this kind of information.
Conclusion
After a mass casualty incident, it is government's responsibility to execute an effective family reunification plan to reconnect families and friends with victims of the incident. Leveraging health information organizations and regional health information organizations as a method to simultaneously search multiple hospitals for missing persons is a strong tool to assist with family reunification in the aftermath of a mass casualty incident.
Agencies responsible for facilitating family reunification in response to a mass casualty incident should first explore obtaining an electronic victim tracking system, such as UVIS, which presents many advantages for victim tracking and family reunification purposes. Additionally, agencies should explore the existence of regional health information organizations and the extent to which they partner with healthcare facilities in their jurisdiction. Agencies should check with their local health departments to determine if there are any existing relationships, as health departments may already be working with regional health information organizations for other public health purposes and can assist with developing new relationships.
Due to the lack of nationwide health information organizations (many are connected only at a state level), connecting to individual regional health information organizations is necessary in order to expand geographical coverage. However, there are still likely to be gaps in coverage if injured survivors leave the state where the incident occurred to seek treatment (as happened in the Las Vegas shooting, where some injured people left Nevada). Until regional and/or state-wide health information organizations are interconnected nationally, this will continue to be a challenge. Once a technical connection between a victim tracking system and a regional health information organization is complete, the majority of the technical solution can likely be reused for connecting to additional regional health information organizations; however, each connection will require some modifications based on the regional health information organizations' software environment. Overall, a tool like NYCEPS that can search for patients across multiple hospitals in real-time provides a benefit to all stakeholders of the incident. It provides value to the public, the healthcare system, and first responders. By building and then integrating this simple search tool into the jurisdictional protocol, government responders can simultaneously reduce the workload of hospitals and first responders as well as provide a beneficial public service to help unify loved ones.
Footnotes
Acknowledgments
Development of the NYC DOHMH New York City Emergency Patient Search (NYCEPS) tool was made possible by funding by Cooperative Agreement Number U90TP000546, funded by the Centers for Disease Control and Prevention, Coordinating Office for Terrorism Preparedness and Emergency Response. The contents of this document are solely those of the authors and do not necessarily represent the official views of the Centers for Disease Control and Prevention or the United States Department of Health and Human Services. The authors would like to acknowledge New York City Department of Health and Mental Hygiene staff Namrata Kumar, Shashidhar Shivanna, and Rehab Uosef, who were critical in the development of the NYCEPS application; the staff at Healthix, New York Cares Information Gateway and Bronx RHIO for their strong partnerships in building the family reunification tool; and Lt. Christopher Zimmerman and Lt. Kevin Sherlock of the New York Police Department.