
Abstract
High-consequence pathogens create a unique problem. To provide effective treatment for infected patients while providing safety for the community, a series of 10 high-level isolation units have been created across the country; they are known as Regional Ebola and Special Pathogen Treatment Centers (RESPTCs). The activation of a high-level isolation unit is a highly resource-intensive activity, with effects that ripple across the healthcare system. The incident command system (ICS), a standard tool for command, control, and coordination in domestic emergencies, is a command structure that may be useful in a biocontainment event. A version of this system, the hospital emergency incident command system, provides an adaptable all-hazards approach in healthcare delivery systems. Here we describe its utility in an operational response to safely care for a patient(s) infected with a high-consequence pathogen on a high-level isolation unit. The Johns Hopkins Hospital created a high-level isolation unit to manage the comprehensive and complex needs of patients with high-consequence infectious diseases, including Ebola virus disease. The unique challenges of and opportunities for providing care in this high-level isolation unit led the authors to modify the hospital incident command system model for use during activation. This system has been tested and refined during full-scale functional and tabletop exercises. Lessons learned from the after-action reviews of these exercises led to optimization of the structure and implementation of ICS on the biocontainment unit, including improved job action sheets, designation of physical location of roles, and communication approaches. Overall, the adaptation of ICS for use in the high-level isolation unit setting may be an effective approach to emergency management during an activation.
The incident command system, a standard tool for command, control, and coordination in domestic emergencies, may be useful in a biocontainment event. The authors describe its utility in an operational response to safely care for a patient infected with a high-consequence pathogen on a high-level isolation unit.
T
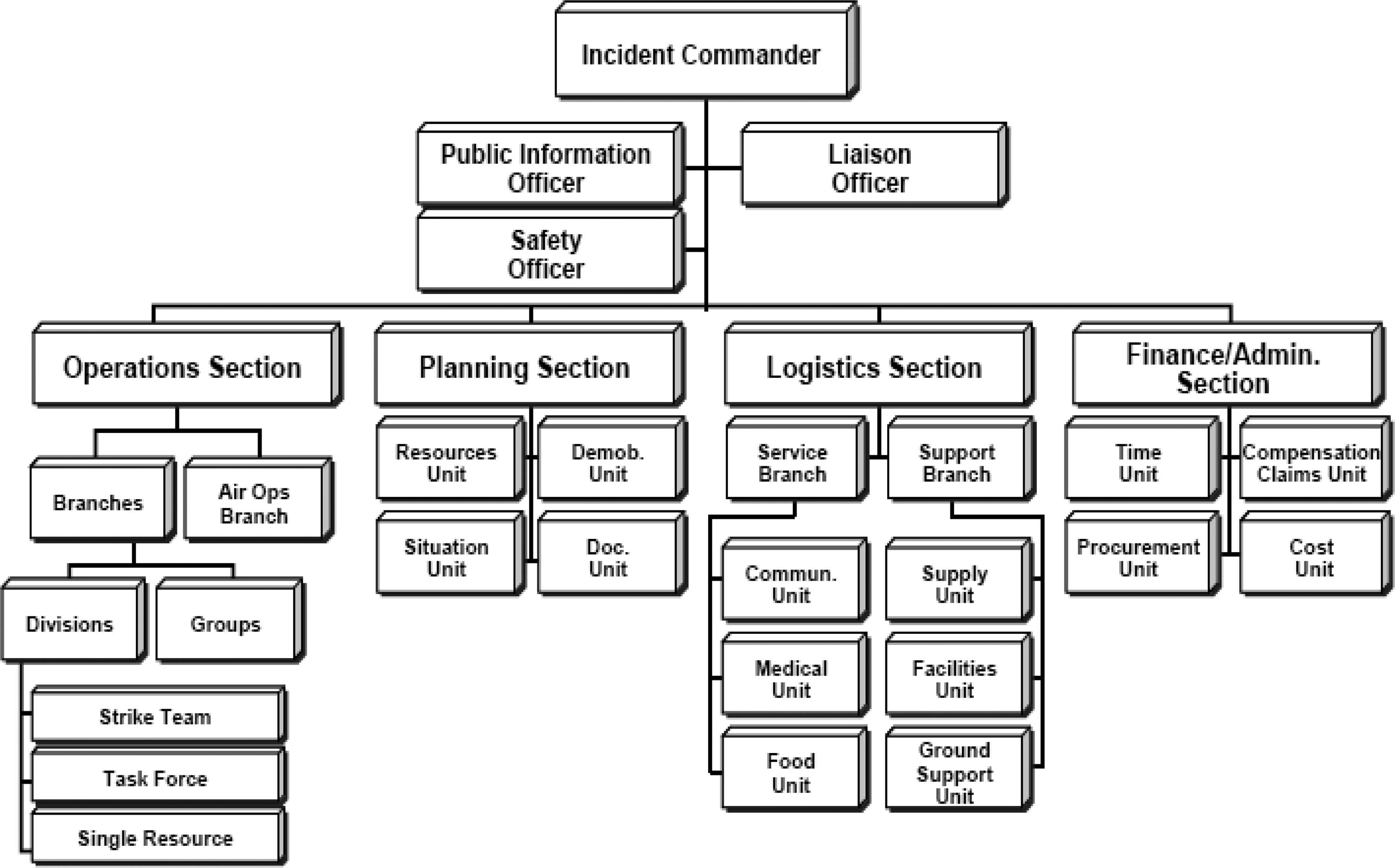
ICS StructureSource: Federal Emergency Management Agency. Incident Command Training Review Material. May 2008. http://www.training.fema.gov/EMIWeb/IS/ICSResource/assets/reviewMaterials.pdf.
The hospital incident command system provides an adaptable all-hazards approach in healthcare delivery systems for both inpatient and outpatient settings. 5 The system is designed to provide a standardized management approach to emergencies such as chemical hazards, explosive incidents, earthquakes, loss of power or water, hostage situations, and other scenarios that might require evacuation of patients and staff.
In response to the 2013-2016 Ebola virus disease (EVD) epidemic, Johns Hopkins Hospital (JHH) created a high-level isolation unit (HLIU), referred to here as the Johns Hopkins biocontainment unit, to manage the comprehensive and complex needs of patients infected with high-consequence pathogens, 6 including EVD. 7 The JHH biocontainment unit is designed to provide clinical patient care while reducing the risk to healthcare workers and the public through high-level isolation, adapted practices, and integrated infection control. The biocontainment unit is 1 of 10 federally funded high-level isolation units, also referred to as the Regional Ebola and Special Pathogen Treatment Centers (RESPTCs), which were established at the direction of the US Department of Health and Human Services Assistant Secretary for Preparedness and Response (ASPR) in 2015, to enhance US national capabilities for the management of patients with high-consequence infectious diseases. 8
The biocontainment unit consists of 3 individual patient care areas with a maximum capacity of 4 patients, including the ability to have 2 patients in 1 room, such as a mother and baby or spouses who are infected with the same organism. 9 The unit includes a laboratory to process clinical and research specimens and 2 autoclaves for effective waste management. 10 The biocontainment unit is staffed by physicians, nurses, laboratory technicians, infection control personnel, respiratory therapists, and radiology technicians who train quarterly in full personal protective equipment (PPE). When not activated for patient care, the biocontainment unit serves as a physical space for training and research activities as well as preparedness drills.
The care team assumes many responsibilities normally provided by ancillary staff, like environmental services, on the activated biocontainment unit to reduce the number of personnel and disciplines that need to train and risk exposure by working on the unit. Beyond the high volume of clinical staff members, many others are involved in the process of biocontainment unit activation and the complex planning, logistics, decision making, and communications that are required for unit operation.
The use of the hospital incident command system has been widely described in the literature.5,11,12 The use of ICS in high-level isolation unit activation and operational response, however, has been limited, but it has been previously demonstrated as an effective approach to the management of patients infected with high-consequence pathogens. 13 The unique challenges and opportunities of providing care in a high-level isolation unit led the authors to modify the hospital incident command system model for use during activation of the biocontainment unit at JHH.
Emergency Management at Johns Hopkins
Johns Hopkins Hospital uses the hospital incident command system to provide an organizational structure that enables many people to work together cooperatively to develop a plan of operational response, termed an incident action plan (IAP). The plan includes the incident goals and objectives, safety directives, response strategies and tactics, situational assessments, and logistics plans for a determined operational period. 14 Establishing metrics and measurements for operational outcomes is an important part of the JHH biocontainment unit planning process, so stakeholders can assess operational performance and adapt the incident action plan accordingly. The process and procedures of the hospital incident command system—which include operating a centralized incident command center, limiting the supervisory span of control, and defining a chain of command—facilitate a more efficient and effective management approach. 15 This is required at JHH when an increased level of coordination and control is necessary to respond to situations such as natural disasters, acts of terrorism, or complex operations like caring for a patient infected with a high-consequence pathogen. In 2018 alone, the system was used to successfully manage a major supply chain interruption, a flood in the adult emergency department, and an ongoing patient throughput crisis during influenza season.
Organizational Structure
The biocontainment unit, in collaboration with the JHH Office of Emergency Management (OEM) and the Johns Hopkins Office of Critical Event Preparedness and Response (CEPAR), created the modified ICS structure for biocontainment unit response operations (Figure 2) that functions separately, but in coordination with, the hospital incident command center (HICC). The scalability of ICS allows structure to be adapted to serve the unique needs and institutional seat of the biocontainment unit. Subject matter experts and key stakeholders met to determine the location of the biocontainment unit incident command center, delineation of roles between the biocontainment unit and the hospital incident command center, physical location of the biocontainment unit command staff, and the expertise required to fill each role. Job action sheets were created to clearly define the roles and responsibilities of each biocontainment unit ICS position. This structure has been tested and refined during 2 functional and 1 tabletop exercises.

Modified ICS
Administration
The biocontainment unit leadership structure is housed in the Johns Hopkins University Department of Medicine, which follows departmental disaster plans under the direction of the hospital incident command center. Biocontainment unit activation is a collaborative decision made by the hospital's executive leadership, in conjunction with hospital emergency management and with the advice of biocontainment unit leaders and the state health department.
The biocontainment unit works closely with CEPAR and JHH OEM to coordinate system-wide responses to potential infectious disease threats. This ensures that the resources needed—including personnel, materials, and finances—are available during an activation, when resource requests are made through either the biocontainment unit or the hospital incident command center.
Leadership Team
The biocontainment unit leadership team consists of an executive medical director from the division of infectious diseases and the department of hospital epidemiology and infection control (HEIC), an operational medical director from the division of pulmonary and critical care medicine, an associate medical director from the critical care division of anesthesiology and critical care medicine, an associate medical director from the division of infectious disease, and a director of research from the department of emergency medicine. The leadership team also includes a program manager from hospital epidemiology and infection control, a nurse educator, a nurse manager, and a program administrator.
The command structure of the biocontainment unit is largely collaborative and integrated but has 4 main components based on discipline (medicine, hospital epidemiology and infection control, administration/emergency management, nursing). During biocontainment unit activation, any of the individuals from the biocontainment unit leadership team can assume a chief role in operations, communication, and logistics of the ICS.
Staffing
In order to support the biocontainment unit's intensive staffing needs, the leadership team, in conjunction with the hospital incident command center, can pull staff from the departments of nursing, pharmacy, respiratory therapy, pathology, emergency medicine, and individual clinical divisions (eg, pulmonary and critical care, infectious diseases, anesthesiology, and critical care medicine) via resource requests through the biocontainment unit incident command center and hospital incident command center. Staffing for the biocontainment unit is important to consider because of the high nurse-to-patient ratio. Trained biocontainment unit nurses are pulled from their home units to staff an activated biocontainment unit, so their shifts must be backfilled to maintain normal hospital operations. Staff assignments must be distributed appropriately in order to avoid pulling a large number of nurses from one location, which could imperil normal operations. The hospital incident command center assumes responsibility for ensuring that staff members' home departments, and the hospital more broadly, are not negatively affected by the staffing needs of the activated biocontainment unit.
Training
The multidisciplinary training provided to all staff allows them to understand how they will operate within this ICS structure. In addition, the biocontainment unit drill committee has been structured to ensure operational readiness at all times. The committee follows the Homeland Security Exercise and Evaluation Program (HSEEP) principles in the planning, implementation, and evaluation of all drills. 16 The biocontainment unit holds a minimum of 4 exercises per year with at least 1 full functional, 1 tabletop, and 1 no-notice exercise. Scenarios include routine clinical care issues as well as special considerations like pediatric care, patient transport, and communication.
Training and exercises place emphasis on the proper practice and choreography of all activation skills. This includes the activation of ICS, initial staffing mechanisms, PPE donning and doffing to minimize the risk for self-contamination during the doffing process, 17 patient care activities, resource requests, and waste management. Training occurs frequently, at least quarterly, to reduce skill degradation and to foster interdisciplinary teamwork and collaboration.
Incident Command System Roles
The decision to open the biocontainment unit requires the input of at least 1 member of the biocontainment unit leadership team, and this person initiates and assumes command of the biocontainment unit ICS. The biocontainment unit incident commander then begins the process of mobilizing staff and assigns them to ICS roles as staff become available. Given the high resource burden of biocontainment unit activation and operations, the use of ICS is critical to ensure continuity of operations as well as a minimization of the impact to the broader hospital, to the extent possible.
The role of biocontainment unit incident commander is filled by a member of the biocontainment unit leadership team who does not have direct patient care duties during a given activation and is primarily responsible for communicating with the hospital incident command center and other stakeholders while coordinating and leading the biocontainment unit ICS team. The role of the biocontainment unit operations chief is filled by a biocontainment unit–trained physician, also without direct patient care duties. The planning section chief role is filled by a member of the hospital epidemiology and infection control team. The safety officer role is filled by a hospital epidemiology and infection control team member or a member of the health, safety, and environment department.
These individuals are subject matter experts who understand the unique risks associated with providing patient care on the biocontainment unit and are experienced with the unit protocols that are designed to address and remediate issues that arise. The logistics chief role is filled by a biocontainment unit nurse who is knowledgeable about the myriad resource needs during a biocontainment unit activation. All of these individuals are located off the unit, in the biocontainment unit incident command center, except for the safety officer and the logistics chief, who are generally stationed on the biocontainment unit. Placing the logistics chief on the biocontainment unit allows that individual to visually assess supply and staffing demands and effectively communicate other resource needs while still maintaining communication with the incident command center with minimal impact on operations on the biocontainment unit. The safety chief sits in the biocontainment unit to ensure real-time situational awareness of and urgent response to any potential safety or security challenges. These positions expand and collapse as necessary, depending on the size and scope of the emergency and the needs that arise during the response. It is important to note that the finance section of the biocontainment unit ICS structure is supported by hospital incident command system administrative staff and not stood up in the biocontainment unit ICS. During activation, financial and administrative decisions are made at the hospital incident command center, in conjunction with JHH leadership. Biocontainment unit incident command center staff are able to visualize all activity on the unit through use of a secure, bespoke video conferencing system (Polycom, San Jose, CA), a critical communication and situational awareness tool.
Incident Command Center Location
To ensure the biocontainment unit needs are met, while maintaining safety and security of the unit, the biocontainment unit incident command center is established in a secure location outside of the high-containment area. During a biocontainment unit activation, both the biocontainment unit incident command center and hospital incident command center are activated, and communication is established between them via 2-way radios. In addition to supporting overall hospital processes, the hospital incident command center provides support for positions such as the liaison officer and the public information officer, who are not activated for the biocontainment unit ICS. This support is important, as the other biocontainment unit ICS roles primarily require expertise in biocontainment unit operations.
Response Operations
The concurrent activation of the biocontainment unit and hospital ICS allows for a scaled response with operational control maintained at the optimal functional level. For instance, the biocontainment unit ICS is responsible for maintaining staffing models with specially trained providers to safely provide patient care. The activation of these providers has a significant impact on overall hospital operations. The hospital incident command center is responsible for providing these clinicians to the biocontainment unit while activating and managing alternative resources, personnel and otherwise, to ensure continuity of hospital operations.
As a biocontainment incident draws to a close, both the biocontainment unit and hospital ICS teams must consider how and when to begin the process of demobilization. In this structure, the decision to deactivate the biocontainment unit ICS is made jointly between the hospital and biocontainment unit incident command leadership. Deactivation may begin prior to the discharge of the patient, as resource requirements are reduced, but occurs in phases that allow for the biocontainment unit to transition from a fully operational clinical unit and to a non-activation dormant state.
After a biocontainment event, the unit must be terminally cleaned and restocked to prepare for the next event. While this process may not require the full complement of resources and incident command needed for a clinical event, the post-clinical phase of operations persists as long as necessary to return to normal operations. Both the hospital and biocontainment unit ICS will continue to provide the operational and logistical planning to ensure that the biocontainment unit returns to operational readiness in a timely manner while limiting the impact on hospital and health system operations.
Implementation
This biocontainment unit ICS structure was first tested during a full functional exercise in which both the hospital and biocontainment unit ICS structures were activated to support the acceptance of a simulated pregnant patient from the Johns Hopkins outpatient center. This exercise highlighted the complexities of facilitating transport of a patient suspected to be infected with a high-consequence pathogen from the outpatient center to the biocontainment unit. Overall, the exercise and implementation of the biocontainment unit ICS was successful, and anecdotal reports suggest this exercise ran more effectively than previous ones, even though it was more complicated and involved broader participation across the hospital and health system.
As part of HSEEP compliance, the biocontainment unit team conducted a hotwash, developed a comprehensive after-action report, and identified opportunities for performance improvement. While the biocontainment unit ICS component of the exercise was successful, it highlighted opportunities for continued improvement. A debriefing after the exercise allowed the biocontainment unit team to rapidly evaluate the process in a no-fault environment. After-action report findings have led to a revision of job action sheets and a plan to modify the ICS structure during a partial activation, such as a lab-only activation.
The team also determined that biocontainment unit command staff cannot function in multiple roles or have patient care responsibilities. For instance, the safety officer role requires full attention and therefore must not be assigned other infection prevention or biocontainment unit duties. Potential safety issues arise when command staff are assigned additional tasks beyond their job action sheet. Prior to testing the biocontainment unit ICS structure in an exercise, the biocontainment unit team was not certain whether the incident commander and the operations chief should be located inside or outside the biocontainment unit, and this continues to be tested in exercises to determine the best location. Currently, the biocontainment unit incident commander and operations chief are located in the biocontainment unit incident command center.
The team also elected to locate the biocontainment unit incident command center outside the biocontainment unit high-containment area, in a secure location with audiovisual communication into the biocontainment unit. This configuration worked well, and the exercise confirmed that the physical separation of the command team from the unit did not impede efficiency as long as communications were maintained appropriately. A biocontainment unit incident command cart, including relevant procedures and materials for initial activation, was also created as a follow-up action to aid in prompt activation and to provide the ability to modify the pre-identified location of the biocontainment unit incident command center, if necessary (Figure 3).
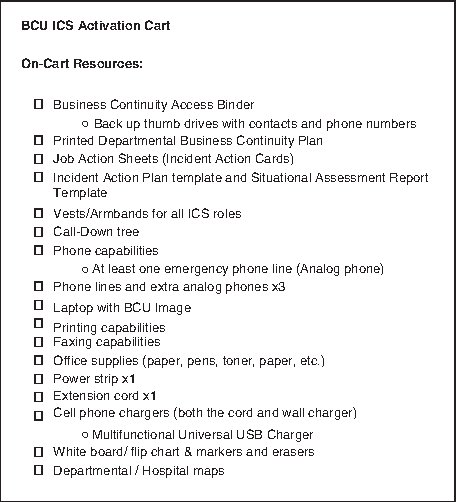
Biocontainment Unit ICS Activation Cart
A high-level isolation unit activation provides a unique challenge in interfacing with the public. Misinformation, or a lack of information, has the potential to create public panic, and information must be provided in an accurate, clear, timely, and actionable manner. Likewise, hospital operations can be negatively affected by healthcare workers' being concerned about an occupational exposure. The biocontainment unit ICS does not directly interface with the public, but instead depends on a joint information center through the hospital ICS for dissemination of information to both the hospital staff and general public. By using the central joint information center, the biocontainment unit ICS is able to leverage the full media relations capacity of the hospital system while avoiding the confusion created by multiple messages coming from one institution.
Discussion
Since the Ebola epidemic of 2013-2016, there has been an increased focus on improving readiness for high-consequence pathogens globally. This effort has included the creation of dedicated high-level isolation units as well as guidance for assessment and frontline hospitals to support the rapid identification, isolation, and treatment of infectious disease threats in the community prior to a safe patient transfer to a more appropriate facility. High-level isolation units must be activated on short notice to receive patients, within 8 hours or less, and may benefit from implementing an ICS structure to manage the complex and unique challenges involved with patients with highly infectious diseases.
As the ASPR Region 3 high-level isolation unit, the JHH biocontainment unit requires a leadership and emergency preparedness structure that allows it to be able to be activated and to respond to serve its unique role in hospital operations and community safety. It is activated only in times of need and, thus, does not function like other hospital units; standard models of unit governance do not readily apply to the biocontainment unit. This specific ICS structure was created for the JHH biocontainment unit, and it has been functionally tested in a large-scale exercise. ICS provided a critical structure for the support of simulated patient care processes and clarified the lines of command and communication among clinical providers, unit leadership, and hospital and health system leadership. The biocontainment unit ICS interfaces with the hospital ICS to scale the response appropriately and limit the impact on hospital operations.
JHH maintains a dedicated, highly functional emergency management system, which includes training and support in incident command for hospital administrators and clinicians and routine use of the hospital incident command system. While the hospital incident command system provides a general structure for incident response in the hospital setting, modifications were necessary based on the unique needs of a biocontainment unit. For instance, the unit leadership decided to physically co-locate the safety officer in the biocontainment unit physical space while locating the biocontainment unit incident command center outside of the biocontainment unit area. While aiming to minimize the number of staff that are physically located in the biocontainment unit environment, having the safety officer on site does provide a higher level of situational awareness required to rapidly address any potential threats to patient or provider safety.
Lessons learned from application of ICS in the biocontainment unit setting—such as where to place various ICS staff, how to interface with a larger hospital system, and the creation of an ICS cart for ease of activation—can be extrapolated for use in other hospital units, especially high-level isolation units and those that may have a role in the assessment and treatment of patients with high-consequence infectious diseases.
Conclusion
A high-consequence pathogen outbreak is a unique event with implications for unit and hospital operations, as well as a potential impact on the greater community. The application of ICS principles to high-level isolation units provides the structure and logistical support to ensure the safety of patients, healthcare workers, the hospital, and the surrounding community. This use of ICS for the JHH biocontainment unit can serve as a model for other hospitals preparing to provide care for patients infected with high-consequence pathogens.
Footnotes
Acknowledgments
The authors thank the Office of the Assistant Secretary for Preparedness and Response, Hospital Preparedness Program (HPP) Ebola Preparedness and Response Activities for providing financial support. The authors also thank the Office of Emergency Preparedness and Response of the Maryland Department of Health and the National Ebola Training and Education Center (NETEC) for their ongoing contributions to our mission. The authors also thank the leadership of the Johns Hopkins Hospital, Health System, and University for their ongoing support of the JHH biocontainment unit mission to keep patients, providers, and the community safe from the threat of highly infectious diseases. This work was supported by the Office of the Assistant Secretary for Preparedness and Response, Hospital Preparedness Program (HPP) Ebola Preparedness and Response Activities (No. U3R2015002863).