
Abstract
The target of eliminating measles has not been achieved, and measles has resurged in Zhejiang, China, since 2013. In this study, we hypothesized that population density and the proportion of the floating population were the potential causes of measles persistence in Zhejiang. Measles cases in Zhejiang from 2004 through 2017 were analyzed using data from the National Notifiable Diseases Reporting System (NNDRS). Reported measles incidence and annual incidence by age were described. Spearman correlation coefficients were used to assess correlations between measles incidence and population density and the proportion of floating population. A total of 48,648 measles cases were reported during the 14-year period. Two large measles epidemics occurred in 2005 (14,317 cases, incidence of 29.38/100,000) and 2008 (12,782 cases, incidence of 25.26/100,000). A higher proportion of cases occurred in young adults aged 20 to 34 years and infants under 1 year of age. A positive correlation was observed between measles incidence and either population density or proportion of inter-provincial floating populations. In general, Zhejiang suffers from a high incidence of measles partly because of its high population density and the low vaccination rates among inter-provincial floating populations. To meet the target of measles elimination, convincing susceptible young adults and migrant children to get vaccinated remains a critical issue.
The target of eliminating measles has not been achieved, and measles has resurged in Zhejiang, China, since 2013. In this study, the authors hypothesized that population density and the proportion of the floating population were potential causes of measles persistence in Zhejiang. They found that Zhejiang suffers from a high incidence of measles partly because of the low vaccination rates among inter-provincial floating populations.
Measles is a contagious disease caused by the measles virus. Although measles mortality has dropped year by year, the burden remains high in some countries. 1 Measles has been a key contributor to vaccine preventable deaths. Globally, an estimated 109,638 deaths from measles occurred in 2017. 2 In 2005, the World Health Organization (WHO) Regional Committee for the Western Pacific Region (WPR) decided that it should aim to eliminate measles by 2012. As 1 of 37 member states in the WPR, China had committed to 2012 as the target year for measles elimination. In 2012, reported measles cases in China fell to a record low of 6,183 (incidence of 0.46/100,000). However, the incidence rate then rose to 1.96/100,000 in 2013, and measles has resurged again. 3
Zhejiang is an eastern coastal province of China with more than 54.4 million registered inhabitants. Administratively, Zhejiang province is divided into 11 prefecture-level cities, with 89 county-level cities. In the 1990s, rapid industrial expansion made Zhejiang a world factory, drawing more and more migrants. These migrants are called the “floating population.” The “floating population” is defined as “migrants who leave their place of household registration for other cities and towns and reside there for at least 6 months.” 4 In the past 10 years, the size of the floating population in Zhejiang has increased rapidly, from 8.6 million in 2000 to 20 million in 2010.
Numerous outbreaks of measles occurred in Zhejiang before the 1965 introduction of liquid measles vaccine (MV). From 1966 to 1977 (voluntary vaccination period), confirmed measles incidence per 100,000 population decreased from 1,057.95 to 332.96, 5 according to the National Notifiable Diseases Reporting System (NNDRS). The 1978 establishment of the national Expanded Program on Immunization (EPI) resulted in a rapid decrease in the incidence of reported measles cases in Zhejiang. 6 Zhejiang started routine measles vaccination in 1986 with a 2-dose schedule administered at ages 8 months and 7 years. In 2005, the timing of the second dose was changed from 7 years old to 18 to 24 months.
Huge efforts have been made to promote vaccination in Zhejiang. Reported coverage rate for first dose measles-containing vaccine (MCV) among children who reached 12 months was above 95% since 1999. 5 Also, by 24 months of age, more than 95% of local children had received 2 doses of MCV since 2006. However, in the context of high recorded immunization coverage, measles has not been eliminated, and the annual average incidence of measles remained at a high rate of 6.38/100,000 during 2004 to 2017. Therefore, the potential influencing factors need to be identified.
Previous studies showed that large population size and density and a high proportion of floating population might be risk factors for measles.7-11 Both conditions facilitate measles transmission by creating a large potential pool of susceptible populations and high contact rates between infected and susceptible individuals.
In this study, we hypothesized that population density and proportion of floating population were potential causes of measles persistence in Zhejiang. We first conducted a retrospective analysis to examine key epidemiologic characteristics of measles from 2004 to 2017, and we then assessed the correlations between measles incidence and population density and proportion of floating population.
Methods and Materials
Sources of Measles Surveillance Information
We analyzed data regarding confirmed measles cases reported from 2004 to 2017 to the NNDSS at Zhejiang Provincial CDC, China. Data on immunization strategies, vaccine coverage, and outbreak control measures were collected from the EPI system. At the county level, information on population size, county area, and floating populations were obtained from the 2010 population census of Zhejiang Province. The total floating population consists of the inter-provincial floating population and the intra-provincial floating population. The inter-provincial floating population are migrants who currently reside in Zhejiang but whose places of household registration are in other provinces. The intra-provincial floating population are migrants whose current residence and place of household registration are both in Zhejiang, but these 2 places are not in the same county. The inter-provincial floating population migrated mainly because of “manual labor or business” (72.9%). The main reasons for migration of the intra-provincial floating population was “manual labor or business” (37.5%), “education and training” (21.3%), and “migration as dependents” (14.1%). 4 The proportion of each floating population was then calculated (%).
Case Definition
Reported cases were defined as any person with fever and a generalized, characteristic maculopapular rash (ie, nonvesicular) and any of following: coryza (runny nose), cough, or conjunctivitis (red eyes). An epidemiologic investigation was conducted on reported cases for information on possible sources of infection. Laboratory confirmation serological testing was performed by measuring measles-specific immunoglobulin M (IgM). Measles cases in this study were either laboratory confirmed or epidemiologically linked.
Statistical Methods
Spearman correlation coefficients (rs) were used to evaluate potential relations between measles incidence (cases/100,000) and population density (population/km2) and the proportion of floating population (%). In order to find which factor was the key contributor to the correlations between the proportion of total floating population and measles, partial correlation analysis was used to reexamine the relationships between these 2 variables (measles incidence and the proportion of total floating population), controlling for population density and either proportion of inter-provincial floating population or proportion of intra-provincial floating population. All statistical tests were 2-sided, and P-values less than 0.05 were considered statistically significant. Statistical analyses were conducted with SAS statistical software, version 9.2 (SAS Institute, Cary, NC).
Results
The data from the 2010 population census of Zhejiang Province was used as the annual average population status for Zhejiang during 2004 to 2017. In summary, the total population was 54,426,891 in 2010. The total floating population was 19,900,863, of which the inter-provincial floating population was 11,823,977 and the intra-provincial floating population was 8,076,886.
Reported Measles Incidence
From 2004 to 2017, a total of 48,648 measles cases were reported to the Zhejiang CDC. The number of measles cases reported in Zhejiang decreased 94.7%, from 6,180 in 2004 to 324 in 2017, and measles incidence decreased 95.6%, from 13.15 to 0.58 per 100,000 population. As shown in Figure 1, 2 large measles epidemics occurred in 2005 and 2008. There were 14,317 cases in 2005 and 12,782 in 2008, and the incidences were 29.38 and 25.26 per 100,000 population, respectively. The incidence decreased slightly since 2009, reaching the lowest level of 0.10/100,000 in 2012. After that, the incidence rose to 2.72/100,000 in 2013, and measles had resurged again. During 2014-15, measles incidence maintained at approximately 2 per 100,000 population and then decreased to 71% (0.58/100,000) in 2016-17.
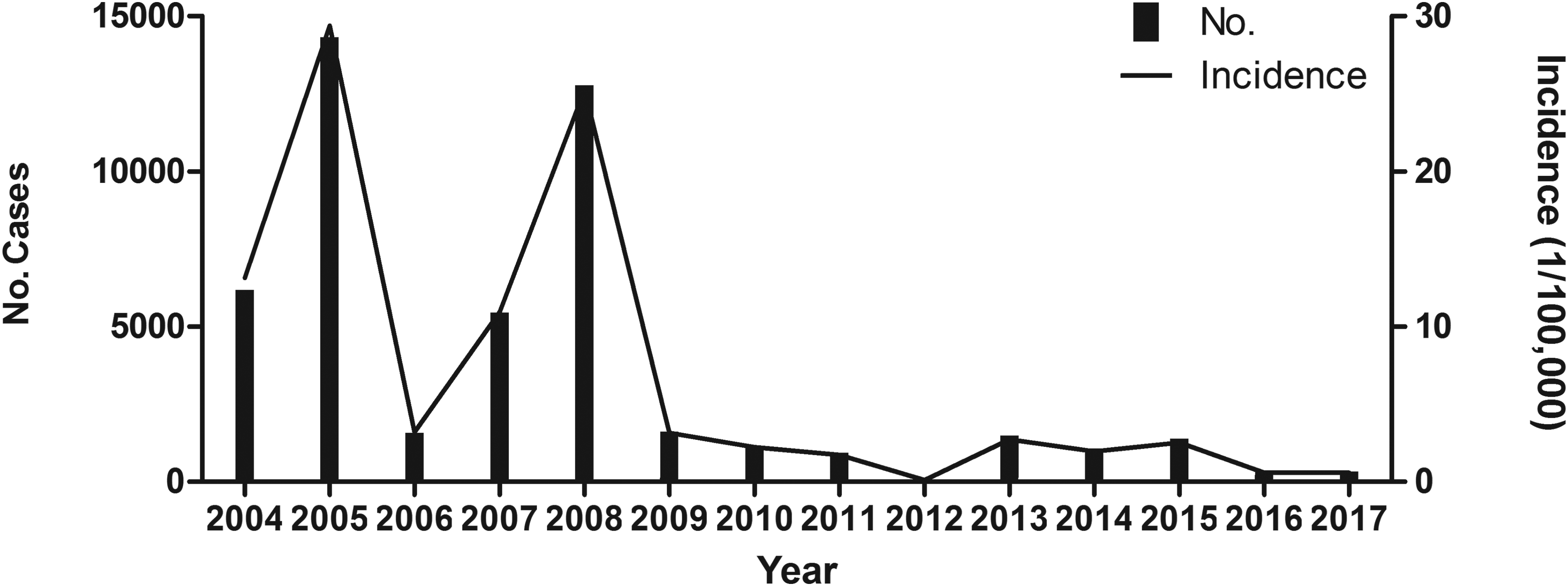
Reported measles cases and incidence during 2004-2017. Two large measles outbreaks occurred in 2005 and 2008. The cases were 14,317 in 2005 and 12,782 in 2008, and the incidence rates were 29.38 and 25.26 per 100,000 population, respectively. Measles incidence reached the lowest level of 0.10/100,000 in 2012. After that, the incidence rose to 2.72/100,000 in 2013, and measles resurged again.

Measles incidence and the proportion of cases by age group. The incidence of measles was highest in infants <1 year old in 2008 (about 685.43/100,000), and higher percentage of cases in infants <1 year of age and adults 20-34 years of age was recorded. Color images are available online.
Age of Cases
Ages of cases are shown in Figure 2. The incidence of measles was high in infants <1 year old in 2005 (about 487.85/100,000). It fell to about 59.29/100,000 in 2006, rose to 266.37/100,000 in 2007, increased rapidly to 685.43/100,000 in 2008, and fell progressively to less than 100/100,000 during 2009 to 2011. After reaching the low level of 2.95/100,000, it increased sharply during 2013 to 2015, then deceased to 8.57/100,000 in 2017.
In adults aged 20 to 34, the incidence of measles rose more than 4-fold, from 8.95/100,000 in 2004 to 41.50/100,000 in 2005 and 36.41/100,000 in 2008, after which it fell to 5.48/100,000 in 2009 and remained at approximately 3/100,000 through 2017. Excluding the 2 years of outbreaks (2005 and 2008), the measles incidence in people aged 35 and older remained below 2 per 100,000 population.
Because of the widespread vaccination of preschool and early school–aged children, the age composition of measles incidence has changed. As shown in Figure 2, among the measles cases, a high percentage of cases in infants <1 year of age and adults 20 to 34 years of age was recorded. Moreover, since 2012, the percentage of cases aged 1 to 19 years had decreased year by year, and the percentage of cases aged ≥35 had risen.
Population Density and Proportion of Floating Population
Population density and proportion of floating population were extracted from the database. The correlation between either of them and measles incidence rates was calculated.
The layout charts are shown in Figure 3. The highest population density was 19,144 (population/km2), and the lowest was 55 (population/km2). The population density was found to be positively correlated with measles incidence rates (Spearman correlation coefficient = 0.488, P < 0.001) (Figure 3A). Higher population density was associated with higher measles incidence. Moreover, the proportion of inter-provincial floating population was the most strongly associated with measles incidence, with Spearman correlation coefficient of 0.584 (P < 0.001) (Figure 3D). No statistical evidence was found between proportion of intra-provincial floating population and measles incidence (Spearman correlation coefficient = −0.041, P = 0.699) (Figure 3C).
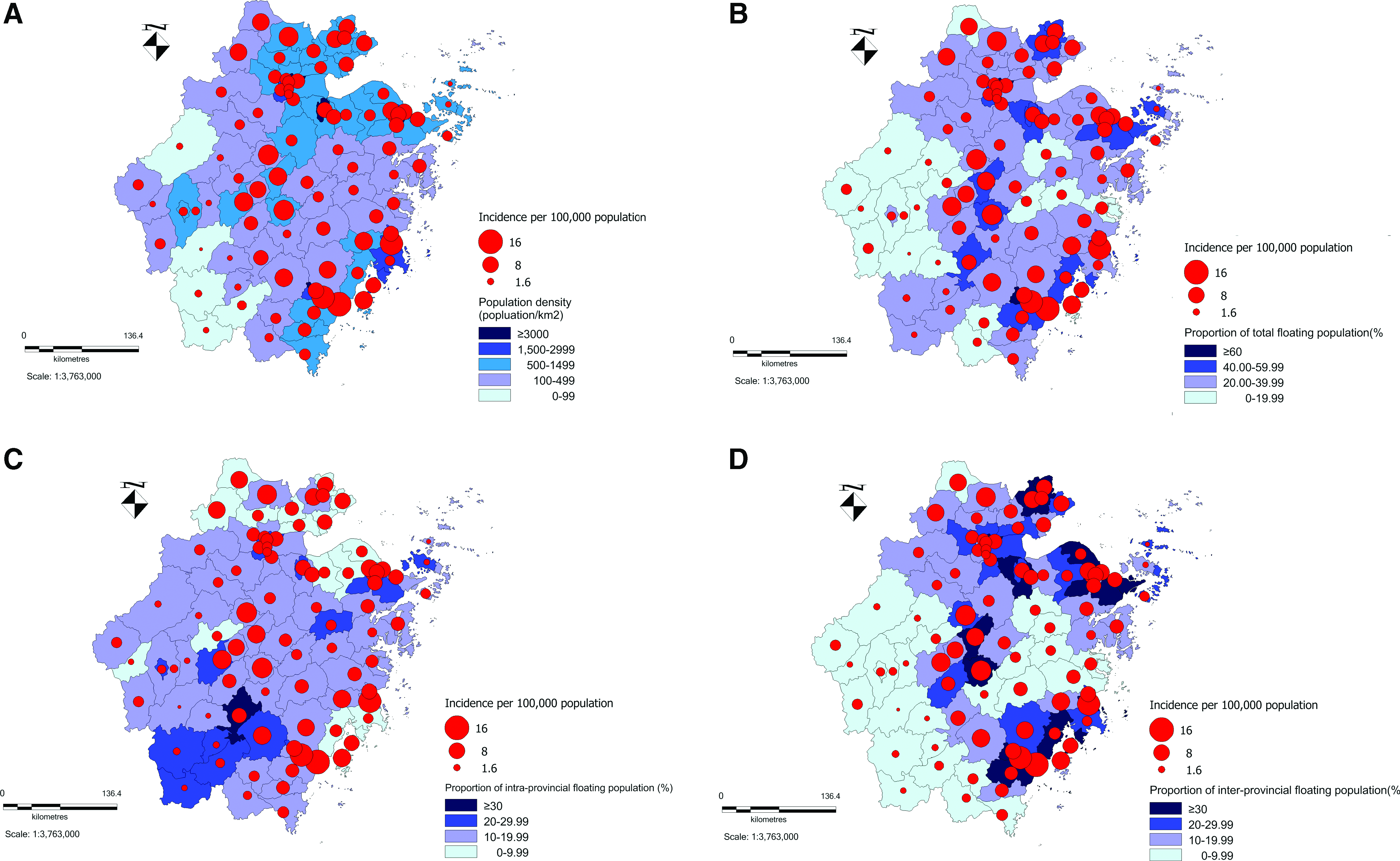
Layout charts for measles based on risk factors. (A) The highest population density was 19,144 (population/km2), and the lowest was 55 (population/km2). The population density was found to be positively correlated with measles incidence rates (Spearman correlation coefficient = 0.488, P < .0001). (B) The Spearman correlation coefficient between total floating population and measles incidence was 0.514 (P < 0.001). (C) No statistical evidence was found between proportion of intra-provincial floating population and measles incidence (Spearman correlation coefficient = −0.041, P = 0.699). (D) Higher proportion of inter-provincial floating population was correlated with higher measles incidence, with Spearman correlation coefficient of 0.584 (P < 0.001). Color images are available online.
Concerning the proportion of total floating population, the Spearman correlation coefficient turned out to be 0.514 (P < 0.001), indicating a close relationship between total floating population and the measles epidemic (Figure 3B). Moreover, in order to find which factor was the key contributor to the correlations between the proportion of total floating population and measles, partial correlation analysis was used to reexamine the relationships between these 2 variables (measles incidence and the proportion of total floating population), controlling for either proportion of inter-provincial floating population or proportion of intra-provincial floating population. Since population density has a high correlation with proportion of total floating population (rs = 0718, P < 0.001), we also included population density as a controlling variable in the partial correlation analysis. After controlling for population density and proportion of intra-provincial floating population, the positive correlation between proportion of total floating population and measles incidence was further emphasized (partial correlation coefficient = 0.604, P < 0.001). On the other hand, no correlation was found between proportion of total floating population and measles incidence after controlling for proportion of inter-provincial floating population (partial correlation coefficient = 0.061, P = 0.572). In other words, proportion of inter-provincial floating population was the key contributor to the measles incidence.
Discussion
We described epidemiologic characteristics of measles in Zhejiang, with 48,648 cases reported during 2004 to 2017. According to data released by the Chinese Center for Disease Control and Prevention, the national incidence of measles was highest in 2008 (9.95/100,000), then decreased to its lowest level of 0.46/100,000 in 2012, rose substantially to above 3/100,000 during 2014-15, and remained at approximately 1/100,000 during 2016-17. In general, except the years of outbreak, the measles incidence of Zhejiang was normally lower than that of the whole country. Moreover, we have observed 2 measles outbreaks in Zhejiang during the 14-year period. One occurred in 2005 and the other occurred in 2008. The incidence rates were both approximately 30/100,000, a 3-fold increase over the average incidence of the previous 20 years. These 2 outbreaks were probably due to the low vaccination rate of migrant children and the lack of vaccination history in adults.12,13 The vaccination rate was 67.95% among migrant children aged 8 months to 3 years in 200512 and 80.82% among migrant children aged 8 months to 6 years in 2008. 14 Both rates in migrant children were lower than that of local children (≥95%).
The recent increase in reported cases of measles has been accompanied by differential changes in age-specific incidence. Risk for measles increased in the young adult group (20-34 years old) and the infant group (<1 year old). Similar results were obtained in several independent studies.15,16 Infants are susceptible to measles because they have not yet reached the age of primary immunization. The increased risk of measles in young adults aged 20 to 34 years might be attributed to 3 reasons. First, young adults aged 20 to 34 were born in the 1980s, and the measles vaccination rate did not exceed 80% in those years. It was about 62% in 1984. 12 Second, the measles vaccine in the 1980s was a liquid vaccine with poor cold-chain conditions, which might result in a higher proportion of immune failures. Third, the antigen of measles vaccine per dose was only 0.2 ml before 2005 and became 0.5 ml after 2005. There may be differences in vaccination effects before and after 2005.
To interrupt all residual adult endemic measles virus transmission as rapidly as possible, it may be prudent to ensure that high-risk groups of young adults have records of 2 doses of measles containing vaccine in Zhejiang Province. However, this would be very difficult because of the large adult population with widely varying circumstances and conditions in Zhejiang. Thus, effective measures should be taken during adolescence. To reduce the number of susceptible adolescents to low levels, revaccination campaigns have been conducted targeting all secondary school students in Zhejiang since 2008, regardless of previous measles vaccination or disease history. The students were revaccinated with measles-rubella combined vaccine (MR). It was more convenient to conduct periodic follow-up vaccination campaigns on students when they were still in mandatory education. In addition to raising the level of measles immunity among the students, the revaccination with MR would reduce the incidence of congenital rubella syndrome (CRS) when female students reach childbearing age (assumed to be 16 years and over).
Our study showed a significant positive correlation between population density and measles incidence. Similar findings had been reported in other localities, including the United States, 17 South Africa,18-20 Japan,21-23 and even worldwide. 24 These observations support a hypothesis that measles incidence is positively associated with population density. Intuitively, for high population density clusters, such as crowds at mass gatherings, the frequency of contacts increased. 25 This increase might drive the spread of measles pathogens in both space and time. For example, it was demonstrated that the risk of measles infection increased once the proportion of the population susceptible to measles in a densely populated area was above 20%. 20
There is a wealth of literature supporting an important role for proportion of floating populations in measles epidemics.8,26,27 Additional studies had shown that vaccination rates for measles was 70.30% for the migrant population aged 1 to 40 years and 90.00% for the local population aged 1 to 40 years in Ningbo, a prefecture-level city in Zhejiang Province. 28 A measles vaccination coverage survey in Zhejiang also showed coverage rates of 76.9% for MCV1 and 44.7% for MCV2 among 718 migrant children aged 8 to 18 months. Among migrant children, factors associated with being unvaccinated included families having multiple children, mother's education level, household income, and children with working mothers. 29
In this study, increasing measles incidence rates were observed with an increasing proportion of inter-provincial floating population but not with an increasing proportion of intra-provincial floating population. One reason might be that the inter-provincial floating populations usually have lower household incomes and come from the provinces, where economic growth is slower and the public health system inferior to that of Zhejiang Province. The migrant parents usually come to work in Zhejiang with multiple children and do not have enough time to take care of each child; in addition, the parents' awareness of the importance of vaccination may be weak.
To combat the epidemic of measles in Zhejiang, drastic control measures were implemented from 2004 to 2017. In 2008, a secondary school–based mass immunization campaign of MR was conducted, and approximately 99% of students received measles vaccination irrespective of their previous immunization status. Since then, this revaccination has been incorporated into routine vaccination services and conducted every year. Moreover, the Zhejiang government implemented a measles vaccine supplemental immunization activity (SIA) for children aged 8 months to 14 years in 2010. In Zhejiang, vaccination history would be checked when children entered kindergarten and primary school to ensure that school-age children have been vaccinated against measles.
Despite these measures, a number of additional activities should be undertaken to improve the measles vaccination rate. Briefly, it is important to improve outreach services, including notification and supplementary immunization activities. It is also necessary to insist on the revaccination campaigns targeting all secondary school students every year. Moreover, improvements are needed to identify and reach migrants with low levels of immunity. For instance, we should implement measles SIA targeting migrant children at some time in every year (eg, Chinese New Year holiday). Additional studies also suggest that nosocomial transmission of measles should be reduced by several efficient measures in Zhejiang. 30
There are several limitations to our study. The main source of measles cases were hospital records, and a proportion of those reported measles cases might have been misclassified. Compared with rural areas, measles reporting was thought to be more complete in urban areas. Therefore, a proportion of actual measles cases may be underreported or misreported. Furthermore, this study is mainly descriptive and did not control for potential confounding factors (eg, changes in population structure and socioeconomic status). Therefore, further studies of more detailed epidemiologic surveillance are warranted to confirm our findings.
In conclusion, Zhejiang suffers from a high incidence of measles partly due to high population density and low vaccination rates among inter-provincial floating populations. To meet the target of measles elimination, convincing susceptible young adults and migrant children to get vaccinated remains a critical issue.
Footnotes
Acknowledgment
The authors declare that they have no conflict of interest. Measles case data were collected from the measles surveillance system. The patients' information contained in the records was removed before analysis. Therefore, no informed consent was required, and there were no ethical issues relevant to the study. This study was funded by the National Natural Science Foundation of China (grant number: 71704042) and the Natural Science Foundation of Hangzhou Medical College (grant number: 2016XZA05).