
Abstract
In response to the 2014 Ebola outbreak in West Africa and resulting cases in the United States, the Occupational Safety and Health Administration developed a personal protective equipment selection matrix to help employers protect workers from exposure to Ebola virus in the event of additional US cases. Now, the world's second largest Ebola outbreak on record continues to expand in the Democratic Republic of Congo, where more than 70 Ebola-infected healthcare workers serve as reminders of the importance of robust infection prevention measures in keeping infectious disease responders from becoming victims themselves. Toward facilitating preparedness for cases associated with the ongoing or future outbreaks, this article discusses the matrix of personal protective equipment recommendations. The matrix applies to a variety of job tasks in health care, laboratories, waste handling, janitorial services, travel and transportation, and other sectors where workers may be exposed to the Ebola virus during outbreak events. A discussion of the information sources and decision-making process for developing the matrix forms the basis of the recommendations. The article then emphasizes challenges and considerations for formulating the matrix, including identifying information sources to help characterize occupational exposures, aligning recommendations among stakeholders with varying viewpoints, and balancing worker protections with feasibility concerns. These considerations highlight issues that remain relevant for preparedness efforts ahead of future US cases of Ebola or other emerging infectious diseases.
OSHA developed a personal protective equipment selection matrix to help employers protect workers from exposure to Ebola virus in the event of future US cases. Toward facilitating preparedness for cases associated with outbreaks, this article discusses the matrix of personal protective equipment recommendations, which apply to a variety of job tasks in healthcare, laboratories, waste handling, janitorial services, travel and transportation, and other sectors where workers may be exposed to the Ebola virus during outbreak events.
The Ebola virus (EBV) outbreak in the Democratic Republic of Congo (DRC), now the second largest on record after the West Africa epidemic approximately 5 years ago, continues to expand. As of March 10, 2019, there have been more than 900 confirmed or probable cases and at least 582 deaths among confirmed cases. 1 More than 70 healthcare workers are among those infected, 26 of whom have died. These worker infections are reminders of the importance of robust infection prevention measures, including personal protective equipment (PPE), in keeping infectious disease responders from becoming victims themselves.
Although the current outbreak has been contained in the DRC thus far, preparing for domestic cases remains critical to ensuring a safe and successful public health response if infected individuals again reach the United States. In addition to several aid workers whom the US government transported from abroad for observation or treatment at the Nebraska Medical Center, Emory University Hospital, and the National Institutes of Health (NIH) since the start of the West Africa outbreak, 2 other individuals presented in Texas and New York with Ebola virus disease (EVD) in 2014 after arriving in the United States on their own. The Texas case spread EBV to 2 healthcare workers.
While well-equipped biocontainment facilities with teams that have undergone intensive training in infection prevention are typically activated to care for intentionally repatriated patients, other healthcare facilities and their workers could encounter spontaneously presenting EBV-infected individuals at any time. Because of their job tasks, workers in laboratories, environmental services (ie, cleaning), law enforcement, air travel and other transportation operations, and waste management, among other sectors, may also be at risk for EBV exposure if cases reach the United States. As such, employers of workers who might evaluate, isolate, handle materials from or contaminated by, or otherwise interact with EBV-infected individuals should have plans to protect employees with appropriate controls, including PPE.
In this article, we describe development of an Occupational Safety and Health Administration (OSHA) EBV PPE selection matrix during the response to the West Africa epidemic and resulting US cases. 2 While we discuss the process for creating the matrix, this article emphasizes challenges and considerations for developing the guidance, especially those relevant to continued preparedness efforts. Understanding the basis of OSHA's PPE matrix and the issues the agency considered in preparing it may facilitate user efforts to incorporate the recommendations into their own workplace planning efforts.
Methods
OSHA aimed to develop adaptable PPE recommendations for safeguarding workers in a variety of different jobs from occupational exposure to EBV in the United States. We organized this information into a matrix that links work tasks with appropriate equipment, an approach consistent with PPE-related communications the agency has issued for other types of emergencies.3,4
Before making equipment recommendations, OSHA needed to assess exposure scenarios warranting PPE. To identify job tasks with possible EBV exposure, we adapted the Centers for Disease Control and Prevention (CDC) EBV-specific epidemiologic risk factors framework.
5
It covered most types of exposures we anticipated addressing in the PPE matrix, and it allowed us to identify workers likely to have at least some EBV exposure risk during an outbreak in the United States. Those included workers with tasks that could result in, among other things:
Close contact with an individual while the person exhibited EVD symptoms; Percutaneous (eg, needlestick) or mucous membrane exposure to blood or body fluids of a symptomatic person with EVD; Contact or droplet exposure to the blood or body fluids of a symptomatic person with EVD; Direct contact with a dead body (considering other factors about the decedent and exposure); and Other low- but not no-risk exposures.
These risk factors focus on contact transmission (ie, exposure to EBV contained in blood, body fluids, or other potentially infectious materials). However, some evidence suggests that aerosols containing infectious particles of a variety of sizes suspended in the air also present exposure hazards.6-8 Without empirical support for excluding this transmission route, OSHA also considered job tasks that could result in EBV exposure in aerosols, including aerosol-generating procedures in healthcare and laboratory work and aerosols generated by maintenance, janitorial, and waste management operations. For all tasks evaluated, our aim was to identify PPE that would prevent contact of exposed skin and mucous membranes with blood, body fluids, or other potentially infectious materials that could contain EBV. We also offered recommendations for respiratory protection when we believed workers might encounter potentially infectious aerosols. In general, activities with lower risks of exposure to potentially infectious blood, body fluids, and other potentially infectious materials required lower levels and/or fewer pieces of PPE, such as single pairs of gloves or facemasks. As exposure likelihood or intensity increased or aerosols became a concern, we added additional PPE, including barrier garments and respirators.
Scarce, up-to-date, peer-reviewed information on PPE for EBV at the time we developed this matrix (ie, early in the 2014-15 West Africa outbreak) forced us to rely frequently on other data sources in assessing hazards and identifying the types of equipment workers would need to prevent exposures. In some cases, well-accepted federal guidelines for infection prevention proved to be readily adaptable to the matrix. For example, we incorporated recommendations for standard and transmission-based precautions that were already routinely followed in hospitals and other healthcare facilities. 9 For laboratories, we used recommended biosafety protocols from the CDC/NIH publication Biosafety in Microbiological and Biomedical Laboratories (BMBL), including biosafety level (BSL)-4 guidelines for PPE and physical containment of EBV samples. 10 The BMBL guidance is well accepted and nearly universally followed as the gold standard for laboratory biosafety. It provided a basis of recommendations to which we added flexibilities that considered alternative practices from the literature concerned with clinical laboratory response to EVD cases.
For other potential occupational exposures, these types of universal guidelines did not exist. In particular, there was virtually no information on which to base PPE recommendations for tasks associated with waste handling, cleaning, and maintenance operations. We identified very little information about biological agent exposures among these types of workers, especially in the US waste and environmental services industries.
To gather perspectives about hazards and controls in these and other types of jobs, OSHA also met with labor and industry representatives, state and local government agencies, and federal partners with expertise in airline and other public and mass transportation operations, public safety and emergency response, public health, waste management, and death care (ie, mortuary and other postmortem) services—in addition to healthcare and laboratory operations. These stakeholder interactions, though largely informal, were particularly useful in providing anecdotal information about job tasks and exposure hazards that were not available from other sources (ie, the scholarly literature). In collaborating with federal partners, OSHA also worked to ensure alignment of recommendations and requirements across agencies, including when CDC and its National Institute for Occupational Safety and Health (NIOSH) also developed guidance applicable to tasks to which our matrix applies.11-17 Additionally, we considered manufacturer guidelines and industry consensus standards (eg, ASTM standards for breakthrough testing) for various pieces of PPE to ensure the capabilities of such equipment matched the protection we aimed to achieve when including it in the matrix.
An overarching goal in designing the matrix was to ensure that recommendations would help employers comply with their obligations under the Occupational Safety and Health (OSH) Act, to provide workers safe and healthy working conditions. Whenever EBV and related hazards (eg, cleaning chemicals) pose workplace hazards, employers likely need to comply with provisions from a combination of OSHA requirements, including standards for bloodborne pathogens, PPE, and respiratory protection and the general duty clause, Section 5(a)(1), of the OSH Act.18-21
For many of the exposure scenarios and PPE options we considered, there was no apparent consensus among available scientific publications, government guidance, and stakeholder views to inform a clear way forward for recommendations. To distill competing information streams into a single set of guidelines, we often had little choice but to defer to the collective knowledge of the authors and other OSHA staff involved in the Ebola response. The authors have infection prevention, industrial hygiene, epidemiology, and occupational medicine expertise, for example. Given the need to issue guidance quickly, we considered the evidence and made what we believed was the best decision possible for various types of fluid-resistant or impermeable garments, respirators, and other types of PPE. Typically, our approach was to discuss possible hazards and available controls and make a recommendation that satisfied our team members' collective concerns for worker health. In these instances, we also developed accompanying notes to explain additional factors that employers should consider when assessing hazards or identifying exposures, selecting PPE for workers, and implementing elements of a comprehensive infection prevention and worker protection program.
In addition to explanatory notes, the matrix also includes flexible PPE options for most tasks it covers. These options identify which equipment should be used at a minimum and which items might be needed during higher-risk work tasks. Users can also move between different PPE ensembles within the matrix as workers' job tasks change. Whenever possible, we also considered alternative approaches for work practices that could allow for varying levels of PPE for tasks in which exposures were controlled by other means. Consistent with OSHA standards requiring employers to perform hazard analyses and provide appropriate PPE to protect workers (eg, those for bloodborne pathogens, PPE, and respiratory protection), the PPE matrix leaves it up to employers to recognize when tasks, such as aerosol-generating procedures or exposures to large amounts of body fluids, warrant different or additional PPE, or when engineering and administrative controls reduce the need for protective clothing and equipment.18-20
Results
Workers Without Appreciable EBV Exposure Risk
While it was apparent that many workers performing tasks covered by OSHA's matrix were at elevated risk for occupational EBV exposure, it was also clear that the majority of US workers had—and continue to have—low or no identifiable risk for such exposure. Most types of employees work in office environments or other settings in which they perform tasks that generally do not require them to wear PPE for infectious diseases. 22 For workers in some of the sectors with the highest employment, such as manufacturing and construction occupations, there was no reason to anticipate EBV exposures, so no new or additional PPE is warranted (beyond anything those workers already might require for protection against routine job hazards). OSHA emphasized this point by including a column in its matrix for workers without exposure.
General Work Tasks
For general work tasks with possible EBV exposures, OSHA's recommendations reflect the kind and severity of anticipated exposures, as guided by the CDC risk framework. Workers who interact but have no physical contact with individuals with risk factors for but no signs or symptoms of EVD require little or no EBV-specific PPE. As the kind and severity of anticipated exposures increase (ie, from casually interacting with individuals with signs or symptoms of EVD to having physical contact with individuals with signs or symptoms of EVD), so does recommended PPE. For instance, when signs or symptoms of EVD are present, the matrix recommends PPE to protect workers from direct contact with and splashes or sprays of potentially infectious body fluids, including face and eye protection, fluid-resistant gowns or coveralls, and shoe/boot covers—items that are not necessary at lower levels of risk associated with casual (noncontact) interactions (see Table 1).
PPE matrix excerpt for general work tasks with possible EBV exposures
Laboratory Tasks
Marrying the BMBL guidelines with stakeholder input and published alternative work practices yielded flexible recommendations for clinical laboratory work. Research laboratory workers may manipulate samples with higher viral concentrations and conduct cell culture work, among other tasks, that may be more hazardous than the diagnostic testing of patient samples in clinical laboratories. Accordingly, OSHA advised using PPE similar to research laboratories for higher-risk tasks, but noted that clinical laboratory tasks may be done at BSL-2 with BSL-3 precautions in cases where worker exposures are mitigated through engineering and administrative controls and safe work practices (as others had previously suggested 23 ). Table 2 summarizes laboratory PPE recommendations.
PPE matrix excerpt for laboratory tasks
Note. FFR = filtering facepiece respirator; APR = air-purifying respirator; PAPR = powered, air-purifying respirator.
Waste, Maintenance, and Cleaning Tasks
For waste, maintenance, and cleaning workers, the matrix includes PPE that offers extra protection for workers' hands (eg, puncture-resistant or other heavy-duty gloves for waste workers who may encounter sharps) and skin (eg, coveralls in lieu of gowns where cleaning and maintenance workers' exposures may not be focused at the front of the body). OSHA also recommended respiratory protection to address hazards from disinfectants, aerosols potentially containing EBV particles, and the degrading effects of moisture in the work environment on respirators and respirator cartridges. Tables 3 to 5 excerpt PPE recommendations for waste, maintenance, and cleaning tasks, respectively.
PPE matrix excerpt for waste-handling tasks
Package waste according to OSHA's Bloodborne Pathogens standard (29 CFR § 1910.1030) and, if transporting waste off-site for treatment and disposal, DOT's Hazardous Materials Regulations (49 CFR part 172).
Note. FFR = filtering facepiece respirator; APR = air-purifying respirator; PAPR = powered, air-purifying respirator.
PPE matrix excerpt for maintenance tasks
Note. FFR = filtering facepiece respirator; APR = air-purifying respirator; PAPR = powered, air-purifying respirator.
PPE matrix excerpt for cleaning (environmental services) tasks
Note. FFR = filtering facepiece respirator; APR = air-purifying respirator; PAPR = powered, air-purifying respirator.
Healthcare and Death Care Tasks
Coordination with CDC/NIOSH shaped PPE guidance for most patient care tasks in hospitals and other healthcare settings, including those involving individuals with or under investigation for EVD. The matrix and CDC's guidance for emergency department evaluation and management of patients under investigation for EVD consistently describe PPE for initial assessment of both symptomatic and asymptomatic individuals. 14 Similarly, the matrix is generally congruent with CDC's guidance for healthcare workers during management of patients with confirmed EVD or EVD-like symptoms. 16 Exceptions to this centered on OSHA's recommendations and options for respiratory protection and more protective guidelines for garments like coveralls, aprons, and head covers in some scenarios. Table 6 summarizes PPE recommendations for patient care tasks. The discussion section of this article further examines differences between OSHA's matrix and CDC's guidelines.
PPE matrix excerpt for patient care tasks
Note. FFR = filtering facepiece respirator; APR = air-purifying respirator; PAPR = powered, air-purifying respirator.
Death care tasks, including packaging and transferring remains of individuals suspected of dying or known to have died of EVD, are likely to involve exposure risks similar to some healthcare tasks also covered in the matrix. Because of this, the matrix's column of recommendations for death care activities closely follows adjacent columns for patient care and transport tasks. Table 7 captures PPE recommendations for death care tasks.
PPE matrix excerpt for death care tasks
Note. FFR = filtering facepiece respirator; APR = air-purifying respirator; PAPR = powered, air-purifying respirator.
OSHA's full PPE selection matrix is available as part of OSHA Fact Sheet 3761, “PPE Selection Matrix for Occupational Exposure to Ebola Virus: Guidance for Common Exposure Scenarios” (www.osha.gov/Publications/OSHA3761.pdf). A version of the matrix and explanatory notes are also provided in Figure 1.
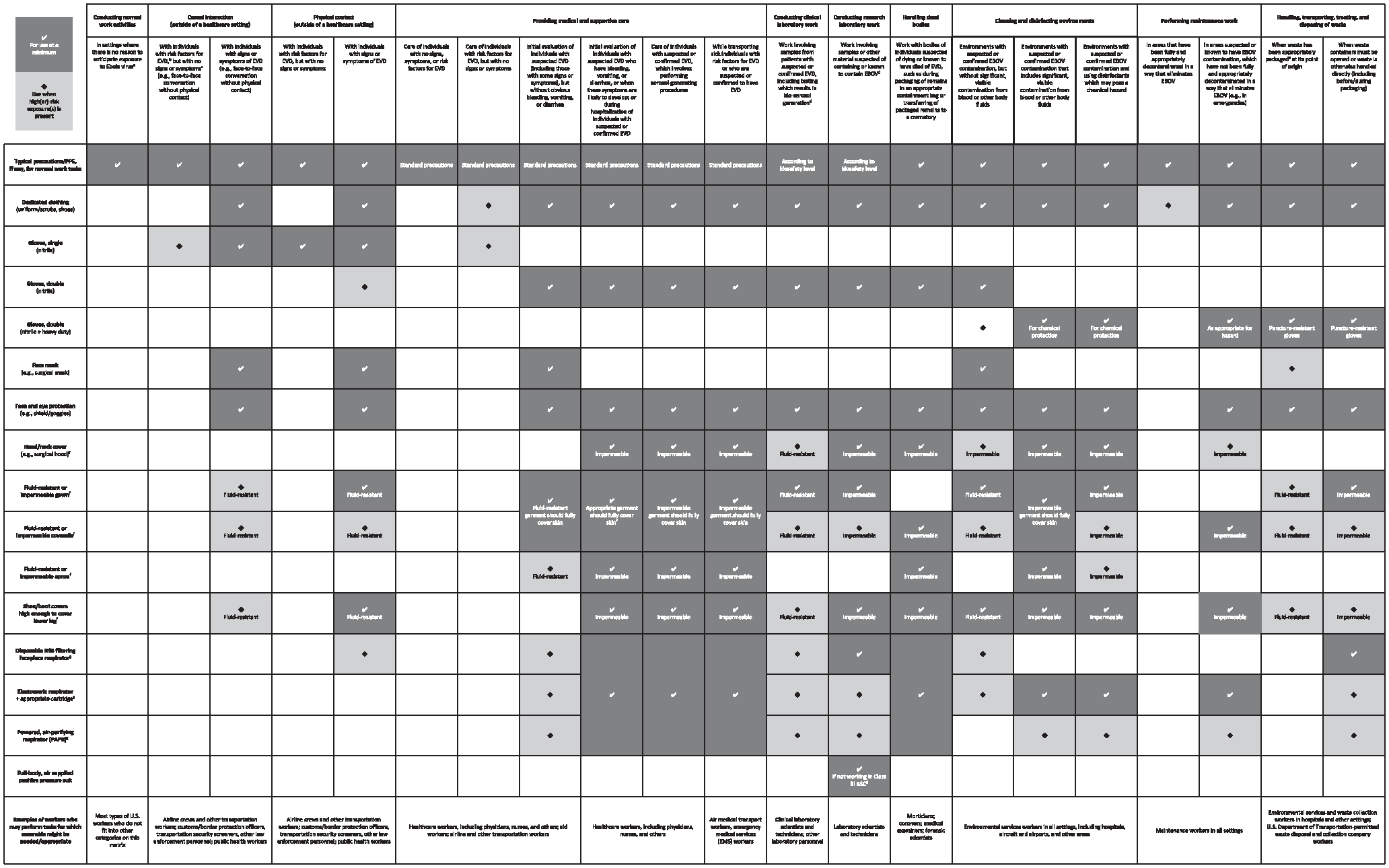
OSHA's full PPE selection matrix
Discussion
General Approach to Developing PPE Recommendations
Planning the matrix initially required determining the extent to which PPE should be used for worker protection against EBV exposures, particularly given that the hierarchy of controls prioritizes elimination and substitution of hazards and reliance on engineering and administrative controls and safe work practices before requiring PPE. Indeed, we agree that these other elements of the hierarchy of controls should be implemented before relying on PPE, if at all possible. However, our extensive PPE recommendations reflect the idea that expanded PPE use offers a more feasible option for protecting workers in healthcare facilities, airports, and waste processing plants; aboard aircraft, ambulances, and other vehicles; and in other workplaces where EBV exposures are most likely during outbreaks. 24 In some cases, using PPE may be quicker and more realistic than retrofitting workplaces with engineering controls (eg, installing negative-pressure isolation rooms with anterooms in hospitals where they do not exist and where the need for them may never arise) during an ongoing outbreak when EBV hazards pose an immediate threat to worker health.
Using PPE as part of a comprehensive infection prevention program also enables workers to continue interacting with patients in healthcare settings, travelers requiring entry screening at borders, and other potentially infectious people without the use of certain engineering controls, like physical barriers, that can preclude direct patient care, body temperature checks, and other interactive tasks. Although some occupational health practitioners may be reluctant to turn to PPE instead of relying on the other elements of the hierarchy, we also note that we are not the first to suggest that available options for preventing worker exposures to emerging pathogens like EBV may be limited, thus necessitating expanded PPE use. 24
Evidence Gaps and Stakeholder Disagreements
As we noted in the methods section, the limited available literature relevant to worker protection against infectious diseases was a major hurdle to developing PPE recommendations, especially outside of health care and laboratories. For employees handling infectious waste, for example, we found only 1 study describing transmission of infectious agents (specifically, Mycobacterium tuberculosis) to US workers. 25 Various studies from abroad described general waste handling work practices, hazards, and precautions, but working conditions frequently differed from those in the United States. PPE recommendations for waste handling, cleaning, and maintenance tasks were further complicated by the fact that exposure to EBV was not the only hazard these types of work pose. Additional chemical, physical, and safety hazards needed to be addressed alongside EBV exposures, a consideration reflected in the matrix's inclusion of heavy-duty gloves and more protective respirators for these types of workers.
Even when published literature and other resources were available to inform our PPE recommendations, we found that there was rarely full agreement among information sources about what equipment to use. Despite our effort to include with the matrix robust explanatory notes about different ways to implement OSHA's guidance while still protecting workers, stakeholder viewpoints in particular were strong and varied. Some workers wanted protections beyond what OSHA deemed necessary. Some employers believed recommended precautions would be difficult to implement. In other cases, employers may have provided workers with overly protective equipment to be cautious, even though authoritative sources recommended lesser protections. Specifically, several stakeholders advocated for stronger recommendations for respiratory protection where none were advised by or being considered for inclusion in guidance from federal agencies. This included during tasks other than medical and supportive care of hospitalized patients with EVD or other higher-risk exposure scenarios OSHA considered as triggers for recommending respiratory protection (eg, during aerosol-generating healthcare and laboratory procedures or cleaning and disinfection tasks that could generate aerosols).
Differing views on respirators likely arise from the complexity of choosing which type of respirator to use for biological agent exposures. There is no permissible exposure limit for biological agents. Identifying sources of exposure, determining how far from a source a worker might be exposed, and characterizing for how long and on what environmental surfaces biological agents remain viable further that challenge. Existing tools for respiratory protection selection generally require users to know at least the occupational exposure limit and expected concentration of the respiratory hazard and, ideally, the concentration at which the hazard is immediately dangerous to life and health. For biological agents, those inputs may not be clear or available. Other gaps in information, including a greater understanding about how EBV is transmitted, its infection process, and determinants of clinical versus subclinical outcomes of exposure also complicate recommendations for PPE and other controls. 26
In the interest of protecting workers, considering stakeholder input, and providing flexibility to employers in selecting specific PPE, OSHA's matrix includes a wider variety of options for respirators than what sometimes appears in other healthcare worker–focused guidance released over the course of the West Africa outbreak response. Specifically, OSHA determined that, though the assigned protection factors of N95 filtering facepiece respirators, half- or full-face air-purifying respirators, and powered air-purifying respirators are different, any of these devices could be used to protect workers from EBV exposure for certain tasks, namely in health care and death care. Some US hospitals have successfully treated EBV-infected patients using various PPE ensembles and without nosocomial infection of participating healthcare workers or ancillary staff. Accounts from such facilities suggest that even the least protective respirator among those mentioned—the N95 filtering facepiece respirator—can be used in a PPE ensemble that successfully protects healthcare workers. 27 Where chemical hazards or excessive moisture would make using a disposable N95 filtering facepiece respirator inappropriate (eg, during cleaning tasks involving significant amounts of disinfectants or other liquids that could impair filtration), OSHA recommended more durable and protective respirators with cartridges designed for the hazard(s) of concern (eg, a combination chemical/particulate cartridge).
For laboratory tasks, using the existing BMBL recommendations as the basis for corresponding sections of the PPE matrix satisfied stakeholders with interests in this area. Importantly, it also provided a reliable roadmap for navigating incongruent CDC and American Society of Microbiology guidance for managing laboratory specimens potentially containing EBV.28,29 Laboratory guidelines from the BMBL manual provided high levels of protection while also having a history of acceptability to and practicability for laboratory workers, managers, and other stakeholders. Research facilities have operated for several decades with well accepted and widely practiced biosafety protocols, including exceptional capacity for agent containment and worker protection when needed. Adaptation of BMBL recommendations allowed clear comparison of controls, including PPE, between various biosafety levels that are routinely implemented in laboratories throughout the country.
CDC and OSHA Recommendations
To help employers comply easily with OSHA requirements while also following other federal recommendations for protecting public health and delivering clinical care, we aimed to align the PPE matrix as much as possible with CDC recommendations. However, there are still differences between the matrix and CDC's guidelines, as we understand them, and employers need to consider these when developing their own workplace infection prevention programs. For example, some CDC guidance for healthcare workers calls for using N95 or better respirators but, when specifying what that means, describes an N95 filtering facepiece respirator or powered air-purifying respirator. 16 For similar exposures, OSHA's matrix includes options for using elastomeric air-purifying respirators with appropriate cartridges (in addition to N95 filtering facepiece respirators or powered air-purifying respirators). An elastomeric air-purifying respirator with at a least a half facepiece and an assigned protection factor of 10 or higher would be expected to provide at least as much protection as a disposable N95 filtering facepiece respirator. Elastomeric air-purifying respirators also can be decontaminated for reuse—a benefit when disposable N95 filtering facepiece respirators are scarce—and are appropriate when workers are using cleaning chemicals for which a combination particulate/chemical cartridge is needed or where moisture would degrade the effectiveness of a disposable N95 filtering facepiece respirator.
It was not just the inclusion of elastomeric respirators that separated the respiratory protection recommendations in OSHA's matrix from those of the CDC guidance. OSHA's matrix recommends using respirators in several situations where CDC does not: for healthcare workers evaluating patients suspected of having EVD but who are clinically stable and do not have bleeding, vomiting, or diarrhea; 30 for testing laboratory specimens that may contain EBV; 29 and for managing body fluid contamination in commercial passenger aircraft. 31 We believe that the uncertainty about potential sources of infection in these situations and, again, the transmission routes through which EBV may spread, warrant respiratory protection: Patients, travelers, and specimens may expose workers to infectious particles if aerosols are generated through natural (eg, a person vomiting) or mechanical (eg, vortexing a sample, disturbing material while cleaning) processes. OSHA also recommends respirators in the matrix's column for workers handling dead bodies of individuals who may have died from EVD, while CDC does not; however, CDC's guidelines apply to handling of remains that are already packaged in a healthcare setting (eg, by healthcare workers in higher level PPE), whereas OSHA's recommendations cover a broader range of death care tasks. 15 Workers handling dead bodies may be at similar exposure risk as healthcare workers until the remains are in sealed, decontaminated packaging.
Other differences between the OSHA matrix and CDC's recommendations involve the extent to which the 2 agencies recommend skin and mucous membrane protection for various workers. Keeping with OSHA's strategy of minimizing exposed skin that could come into contact with EBV in blood, body fluids, or other potentially infectious materials, OSHA sometimes recommends more extensive barrier protection compared to CDC's recommendations. For healthcare workers evaluating clinically stable patients suspected of having Ebola, OSHA recommends using a gown or coverall along with an apron for higher-risk exposures and to protect against unexpected bulk contamination (eg, vomitus, feces), whereas CDC's guidelines note only a gown or coverall. 30 For workers testing clinical specimens that may contain EBV, OSHA included double instead of single gloves, along with a head covering, shoe/boot covers, and coveralls for higher-risk exposures. These items were not part of CDC's recommended ensemble for similar activities, which includes gloves, fluid-resistant or impermeable gown, face mask, and eye protection. 29 Other differences not specifically discussed here may also result from how workers' tasks are categorized. For example, the task-based matrix may prompt airline personnel managing potentially infectious body fluids to use different PPE, such as heavy-duty gloves and additional barrier protections, than they would when following CDC's occupation-based EVD guidance. 31
Matrix Application
In using the final matrix, employers and workers must be mindful that the guidance presents combinations of PPE items selected for certain types of work tasks and sources of exposure. Particularly in cases where skin or mucous membrane exposure to infectious blood or other body fluids is likely, each column of the matrix recommends using items together in a way that we believe will provide sufficient coverage of the skin, eyes, nose, and mouth. For tasks in which aerosol exposures are concerns, the matrix recommends equipment that functions to prevent contact exposures while also protecting workers from inhaling EBV particles or hazardous chemicals. When implementing the recommendations using various brands or types of PPE, employers should ensure that the individual items still meet this objective and that fit-testing supports the use of specific items together, such as a certain face shield or surgical hood with a certain respirator. That may require a qualified industrial hygienist to manage quantitative and qualitative respirator fit testing protocols for workers in full ensembles of PPE.
Importantly, PPE for high-consequence hazards, including EBV, is only effective when workers properly put it on and remove it. This is shown in lessons learned from training initiatives in which healthcare workers failed to demonstrate competency in PPE donning or doffing during training and assessment, including when fluorescent or chemiluminescent dyes applied to PPE were used as markers of would-be exposures under real-life work conditions. 32 However, as the aim of OSHA's PPE matrix is to help employers identify the types of PPE their workers may need for various jobs where we foresaw potential EBV exposure, describing a full donning and doffing regimen was outside the scope both of that work and this article. Other sources, such as CDC, offer protocols for donning and doffing certain PPE ensembles, including for healthcare workers.
The amount of time a worker can wear a PPE ensemble or a particular piece of PPE needed for a task is another important consideration for ensuring the safety and health of workers, particularly when they are at risk for exposure to EBV and related hazards if there are breaches in established work protocols or the PPE itself. Worker stay time in PPE depends on a number of factors, some of which may be difficult to ascertain, including the severity of the hazard the PPE must withstand; the degradation rate or point of PPE failure (ie, permeation rate, breakthrough time from initial exposure until virus particles and/or fluid reach the inside of a garment); an individual worker's physical condition and tolerance for the PPE; heat stress caused or made worse by the PPE; and overall level of worker fatigue, which may also be made worse by the PPE or may compromise a worker's ability to use the PPE properly or remove the ensemble without contaminating him- or herself.
For all tasks where OSHA recommends wearing fluid-resistant or impermeable garments, considering the amount of blood, vomit, and watery excrement (eg, diarrhea) a patient is producing or that is in a contaminated environment should influence user selection of specific fluid-resistant or impermeable items. In accordance with NIOSH's fluid-resistant or impermeable garment document, OSHA recommends providing workers with fluid-resistant garments when the anticipated risk of exposure to blood and body fluids is low and impermeable garments when the anticipated risk of exposure to blood and body fluids is high. 17 Because the PPE matrix cannot describe every possible exposure scenario, it indicates to employers whether specific garments should be fluid-resistant or fluid- and virus-impermeable based on generally anticipated exposures. Employers should determine where exposures are focused (eg, on the center of the body, where the addition of an apron might be most protective, versus on the limbs, where coveralls or shoe/boot covers might be more useful). Examination of a variety of commercially available protective garments also indicated that other considerations beyond fluid-resistant or impermeable coatings on fabric affect the overall resistance or impermeability of the garment, including material thickness and seam and zipper construction and placement. Employers also need to consider other extenuating factors, such as fluid penetration at pressure points, permeation rate and breakthrough time, and garment or equipment performance under the standardized testing conditions NIOSH's research identified.
Providing flexible PPE options whenever possible made the most sense for addressing the practicability challenges as well as for ensuring employers could use different variations of PPE while still protecting their workers. The PPE matrix consolidates a set of recommendations for protective equipment and garments for workers performing a range of work tasks, with those tasks and sources of exposure typically described in ways that allow for employers to select either enhanced PPE for higher-risk exposures or select different PPE items as a worker's tasks or exposure(s) move him or her to a different column of the matrix. Flexibility in how employers assess and control worker exposure is consistent with the philosophy of the hierarchy of controls itself, in that it allows for decision making in the risk-control process rather than adopting a rigid framework for hazard abatement. 33 An employer should provide PPE to workers using the task- and exposure-based categories of the matrix. If work tasks or sources of exposure change, an employer can look at the recommended equipment for higher-risk exposures or across the other columns of the matrix and provide different or more protective PPE for workers as needed. In some instances, such as when laboratory or waste workers perform job functions similar to those of healthcare workers, the flexible, task-based design of the matrix allows users to follow recommendations that most closely align with their job duties, rather than job title, at any given time.
Conclusions
Protective measures, including PPE, for preventing occupational exposure to EBV depend on the type of work, risk of encountering sources of EBV, and the nature of other potential hazards to which workers may be simultaneously exposed. OSHA developed consolidated PPE recommendations applicable to most workers in the United States who are likely to have EBV exposure. When the PPE matrix was originally published, there was insufficient information in the scholarly literature on which to base the recommendations. However, consideration of job hazards and exposure risks alongside stakeholder needs and expert input yielded recommendations suitable for a broad range of work tasks that may be associated with EBV exposure.
Continued debate over what PPE is appropriate for certain work tasks and exposure scenarios highlights remaining gaps in knowledge. Particularly, more research is needed to explore EBV's routes of transmission, including controlled studies to explore the possibility for near- and far-field aerosol transmission that would warrant enhanced respiratory protection for workers performing tasks currently considered to be less hazardous, such as casual (noncontact) interaction outside of healthcare settings with individuals with signs or symptoms of EVD. More work is also needed to inform decision making about worker stay times in PPE ensembles, as well as to identify PPE that minimizes heat stress, worker fatigue, and other undesired side effects of wearing such equipment.
Given these gaps, PPE recommendations and other types of infection prevention guidelines must continue to be updated if and when new trials or other robust studies offer better data to support them. In the meantime, OSHA's PPE matrix remains applicable for preparedness and planning for safe and effective response to possible future domestic EVD cases.
Footnotes
Acknowledgments
The authors thank their OSHA and interagency colleagues who were involved in the development of guidance on which the matrix was based and who contributed their expertise to development of the matrix and review of this manuscript. In particular, the authors thank former OSHA Assistant Secretary Dr. David Michaels and former Deputy Assistant Secretary Jordan Barab for their input on the matrix and drafts of this manuscript. The authors also thank Drs. Thomas Nerad and Margy Lambert for their input on the matrix. The opinions expressed in this article are those of the authors and do not necessarily represent the views of the US Department of Labor (DOL)/OSHA. Mention(s) of products do not constitute endorsements by DOL/OSHA or the authors and are included only as examples of types of PPE.