
Abstract

During a pandemic caused by a novel strain of influenza virus, it is estimated that more than 68 million people in the United States may seek acute medical care.1-3 Providing protection for healthcare personnel who care for patients is essential to ensure continuity of healthcare services during a public health emergency, including a pandemic. 4 However, at the onset of a pandemic, a well-matched vaccine may not be available, and limited supplies of antiviral medications will likely be reserved primarily for treatment of ill patients, instead of prophylaxis. While a hierarchy of infection prevention measures will be widely used, surges of infectious patients may leave many healthcare personnel to use respiratory protective devices (RPDs) as a primary means of self-protection. 5 To promote healthcare worker protection against occupational exposures, the Centers for Disease Control and Prevention (CDC) has sought to understand the optimal roles of RPDs, such as N95 filtering facepiece respirators (N95) and surgical masks (sometimes called medical masks), in the context of a pandemic. Prioritization of RPD allocation to healthcare personnel to limit exposures will require critical deliberation as demand outstrips RPD availability. To arrive at a rational, equitable, and transparent allocation process, stakeholders should build on lessons learned about personal protective equipment (PPE) supply chain from recent outbreaks, such as the 2009 H1N1 influenza pandemic, the 2013-14 H7N9 influenza outbreak, and the 2014 Ebola epidemic. 6
Stochastic modeling suggests that shortages of RPDs during a novel influenza pandemic may become severe. 2 Even when accounting for a surge in manufacturing capacity and conservation at the bedside, health systems may face insufficient numbers of RPDs to meet the needs of healthcare workers and emergency service personnel. If an influenza pandemic becomes severe, such as the one experienced in 1918, several billion N95 respirators are expected to be required to protect US healthcare personnel and emergency services personnel. 2 Importantly, these estimates account only for health care; they do not include the estimated number of N95 respirators needed for workers in all other US sectors.
RPDs are manufactured for the United States in quantities needed to support anticipated normal market demands. Meeting large, sudden increases in demand that would be expected to occur during a severe pandemic would pose a major challenge to US health care. In an influenza pandemic, immediately accessible RPD inventories are too small, and manufacturer surge production is not sufficiently robust to meet anticipated demands. Even if the start of a pandemic could be anticipated, at least 3 to 4 months' lead time is required for manufacturers to produce, and health systems to acquire and store, the RPDs that would be needed for even the earliest wave of cases. 6
Strategies to Conserve RPDs
Measures to conserve RPDs will be essential. The approach to conserving RPDs should be equitable, efficient, and effective and will require a preexisting framework for decision making that is reasoned, stepwise, layered, and transparent. Key strategies are outlined in Figure 1. These include:
Strategies for decreasing demand for respirators, including control banding
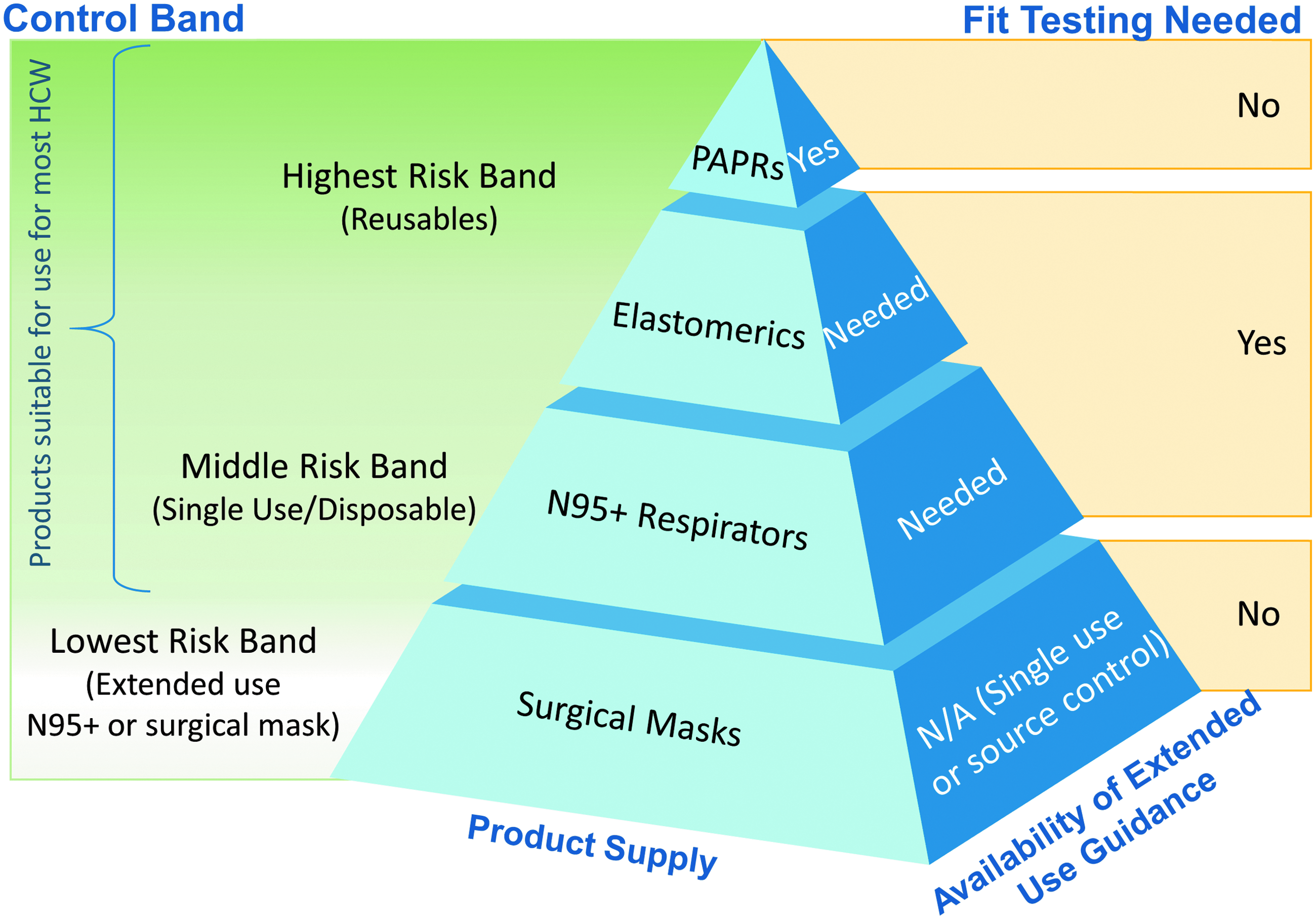
Categorizing individuals or groups based on perceived level of exposure and infection risk, also referred to as “control banding,” is one way to help improve prioritization and selection of respiratory protection.9,10 In this issue of Health Security, Sietsema et al emphasize a need for a pre-established strategy to appropriately quantify estimated risk and exposure, and to assign a control band as a component of pandemic preparedness and response. 11 This approach includes (1) identifying and categorizing workers based on the type of their work and resultant risk of exposure to the novel influenza virus, and (2) prioritizing source and pathway controls to reduce influenza exposure before relying on respiratory protection.
A control banding framework is a key step toward rationalizing allocation of RPDs during an influenza pandemic in which resources are severely constrained. For this conceptual framework to be fully effective at a population level, wide-scale buy-in will be important, including coordination among federal, state, and local public health agencies, healthcare delivery systems and coalitions, community leaders, and other key stakeholders. The framework posited by Sietsema et al addresses work sectors other than health care. However, during an influenza pandemic, it will be critical to maintain healthcare services. As such, healthcare personnel will need to be prioritized as a target population requiring RPDs. Future development of control banding constructs must include the healthcare delivery sector.
Sietsema et al propose an initial framework for categorizing worker respiratory protection tiers called “risk bands,” based on the perceived probability of occupational exposure before an emergency occurs. The US government has similar strategies for critical workers (including healthcare personnel) for other medical countermeasures that are anticipated to be in limited supply, such as vaccine during an influenza pandemic.
12
In October 2018, the CDC released the Interim Updated Planning Guidance on Allocating and Targeting Pandemic Influenza Vaccine During an Influenza Pandemic,
12
which describes major principles to help in planning prior to a pandemic emergency and decision making at the time of an event. In the development of this guidance, outreach efforts with various stakeholders (eg, pandemic planning working groups, public engagements) led to the conclusion that critical populations that should be protected, including: (1) people who are essential to the pandemic response and provide care for individuals who are ill, and (2) workers who are at greater risk of infection due to their job. In addition, to help inform allocation and targeted vaccine use, the vaccine planning guidance includes:
Vaccination tiers and targeting of population groups based on pandemic severity; Planning estimates for the number in each population group; and A description of subgroups that should be considered in instances of extreme product shortages.
For RPDs, control banding serves a similar purpose, to inform allocation and targeted use of RPDs if supply is limited, and may serve as a springboard for pandemic planners to further explore and define at-risk workers. RPD conservation guidance should also consider how applying extended use or reuse of N95 respirators may be applied to risk bands, recognizing that even with this banding approach, there may remain critical shortages of N95 respirators and surgical masks. In a worst-case scenario, when supplies of RPDs and surgical masks are exhausted, more drastic mitigation strategies may need to be considered, such as wearing common household or workplace materials for barrier protection. 13
Lastly, during a severe pandemic, it is probable that demands on the healthcare system will exceed capacity. Accordingly, nontraditional care settings will be needed to care for those with less severe illness, reserving hospitals for those most ill. Alternative care options may help to decrease the overall number of RPDs needed. For example, telemedicine, nurse triage lines, and proactively providing home care instruction eliminate the need for healthcare personnel and for source control, given that there would be no face-to-face patient encounters. 14
A Call to Action
During an influenza pandemic, RPD demands may not be met by available supplies. RPD shortages may require the US workforce, including healthcare personnel, to conserve RPDs. Further development of control banding strategies must include the healthcare workforce to ensure conservation tactics are equitable, efficient, and transparent. Efforts to conserve RPD supplies or to shift from conventional standards of care to crisis standards will be necessary to ensure that those with the highest occupational risk for exposure who provide critical functions are protected. 15
The projected gaps in RPD availability serve as a call to identify actionable solutions, like control banding, prior to the next pandemic. Having tested and validated plans will require broad stakeholder engagement and will need to include a robust communication effort that explains why levels of protection may be different across healthcare personnel. Additional engagement with the public health sector, including infection control experts, and healthcare stakeholders will be necessary to develop an acceptable and feasible strategy to assure that critical workers are protected during a pandemic influenza response.