
Abstract
Laboratory-acquired infections (LAIs), an occupational illness, are defined as all infections acquired through laboratory or laboratory-related activities. A report published in 1898 described an LAI resulting from Corynebacterium diphtheriae being transmitted through mouth pipetting. Despite all efforts, LAIs continue, especially in developing countries like Pakistan, which has been fighting to curb many infectious diseases. As reflected in the published literature, the biosafety culture is severely lacking in many laboratories, and there are no data available from Pakistan on LAIs. Our objective was to ascertain the frequency and rate of LAIs in various labs with versatile portfolios in relation to biosafety and biosecurity practices in Karachi. Ours is a descriptive multicenter cross-sectional study conducted in 30 laboratories located in Karachi from November 2017 to April 2018. Data were collected from laboratories including the university hospital labs, research labs, animal labs, and biomedical labs. Out of 30 facilities, half (n = 15) were clinical/biomedical laboratories, 16.6% (n = 5) were university hospital laboratories, 26.6% (n = 8) were R&D laboratories, and 6.6% (n = 2) were animal laboratories. Needle stick was found to be the most common injury, followed by animal bite/scratch, cut on mucous membrane, falling of personnel, and burn injury.
Laboratory-acquired infections (LAIs), an occupational illness, are defined as all infections acquired through laboratory or laboratory-related activities. The objective of this study was to ascertain the frequency and rate of LAIs in various labs with versatile portfolios in relation to biosafety and biosecurity practices in Karachi.
Laboratory-acquired infections (LAIs) are an occupational illness and are defined as infections acquired through laboratory-related activities. They have been occurring since the beginning of work with infectious agents, 1 but epidemiologic investigation of LAIs has begun relatively recently. The first report of an LAI resulting from Corynebacterium diphtheriae was published in 1898, when the bacterium was transmitted through mouth pipetting. 2 The first survey of LAIs was carried out in Europe in 1915 by Kisskalt, who reported 50 cases of typhoid fever that resulted in 6 fatalities. Most of these infections were transmitted by mouth pipetting. In 1929, Kisskalt reported 83 more cases of LAIs, 59 of which were lab-acquired typhoid. Mouth pipetting was again found to be the most common route of these transmitted infections. 2 In 1976, Pike et al published the largest survey of LAI; they reported 4,079 LAIs caused by 159 infectious agents, which resulted in approximately 173 deaths. More than half of these LAIs were reported as being caused by only 10 infectious agents. 3 Since this study, many surveys have been conducted that reported LAIs from various bacteria, viruses, parasites, and fungi. In the United Kingdom, enteric infections, such as shigellosis, and tuberculosis were found to be the most common LAIs in clinical laboratory workers.4,5 The Flemish environmental agency in Belgium conducted a survey in 2006, which reported 2 LAIs from Listeria monocytogenes and Brucella melitensis. This was followed by another survey in Belgium from 2007 to 2012, which reported 140 LAIs. 6
Laboratory-acquired infections can occur by exposure to or inhalation of an agent, contact with mucous membrane, or percutaneous inoculation, but in most cases, the actual cause remains uncertain. Therefore, the significant increase in work with pathogenic organisms and the emergence of infectious diseases make LAIs a global health security concern.
Since an infected laboratory worker can be an index patient for a new epidemic, 7 many biosafety guidelines have been developed as well as sophisticated containment equipment to prevent LAIs. 8 Despite these efforts, LAIs continue to occur and cannot be ignored, especially in developing countries like Pakistan, which has been fighting to curb infectious diseases. As reflected in the published literature, the biosafety culture is severely lacking in many laboratories,9-11 and no data are available from Pakistan on this topic.
Therefore, this study was conducted to identify and ascertain the incidence of LAIs, to develop indigenous data, and to review protocols followed in response to incidents in research, veterinary, and clinical laboratories. This study will serve as a starting point to understanding the spectrum of problems; to designing and implementing policies and training programs that can mitigate risks in handing, transportation, and storage of infectious pathogens; and to propagating a culture of safety in Pakistan.
Methodology
A comprehensive questionnaire composed of 64 questions was designed under the guidance of technical experts in microbiology and biorisk management from Pakistan and the United States. The questionnaire was formulated to assess the biosafety measures in place, compliance with standard operating procedures (SOPs) and international guidelines, microorganisms or toxins handled, availability and use of personal protective equipment (PPE) and other containment measures, emergency preparedness, suspected LAIs, and possible route of exposure in laboratories with diverse portfolios. The survey was conducted by a research associate under the supervision of the principal investigator among the 30 laboratories in Karachi, Pakistan. The laboratories were selected by a cluster random sampling method. The data were obtained from laboratory staff and recorded by the research associate under the supervision of the principal investigator. Data were then entered and statistically analyzed using SPSS version 20 by a biostatistician.
The data consisted of categorical variables, mostly of the nominal and ordinal type. Each category in the variable was separated from the other. Descriptive statistics were recorded in percentages and frequencies for categorical data. Cross tabulations were done between different categorical variables for finding comparisons between different variables. Bar graphs and pie charts were created as a visual presentation of the data and statistics to generate the numeric description of the data. Bar graphs and pie charts show the relative number of participants in each category (by reporting the percentages/counts within each category). The graphs were made to provide visual comparisons between the different variables. A descriptive analysis provides a detailed report of the percentages and frequencies of all the categorical variables in the study.
Results
Laboratory Affiliations
Of the 30 facilities that were included in the survey, 50% (n = 15) were clinical/biomedical laboratories, 16.6% (n = 5) were university hospital laboratories, 26.6% (n = 8) were research and development (R&D) laboratories, and 6.6% (n = 2) were animal laboratories. Clinical and biomedical laboratories have the same status, while university hospital laboratories are associated with inhouse healthcare laboratories whose main patients are inpatients in the hospital.
Biosafety Levels Surveyed
In cross tabulation analyses, the survey team found that most laboratories were designated as biosafety level 2 (BSL-2), across the 4 types of facilities surveyed. Among clinical/biomedical labs, 6.7% were BSL-1, 73.3% were BSL-2, 6.7% were BSL-3, and 13.3% of the facilities have both BSL-2 and -3 labs. In university hospital labs, 80% were BSL-2, and 20% of the facilities have both BSL-2 and -3 laboratories. All of the animal laboratories were BSL-2, keeping in mind the risk groups with their biosafety and biosecurity challenges. In R&D laboratories, 87.5% of the facilities were BSL-2, and 12.5% were BSL-3 (Table 1).
Biosafety Level of Laboratories Surveyed: Cross Tabulation
Laboratory-related Activities
Data regarding the type of services provided by the laboratories revealed that 83.3% (n = 25) of the laboratories were doing bacteriology, 73.3% (n = 22) were doing serology, 66.7% (n = 20) were doing clinical pathology, and 56.7% (n = 17) were doing molecular diagnostics. Only 13.3 % (n = 4) were dealing with virology, 30% (n = 9) with cell culture, and 10% (n = 3) with toxicology (Table 2).
Types of Services Provided by the Surveyed Facilities
Safety Culture
To prevent exposure to potentially infectious material and to prevent LAIs, it is important to determine the level of biorisk management implementation. We found that 46.6% of the facilities have clearly defined the roles and responsibilities for implementation of biosafety practices. In 43.3% of the facilities, management has stated a commitment but does not have clearly defined roles, while in 10% of the facilities, management has not made a commitment to biosafety (Figure 1).
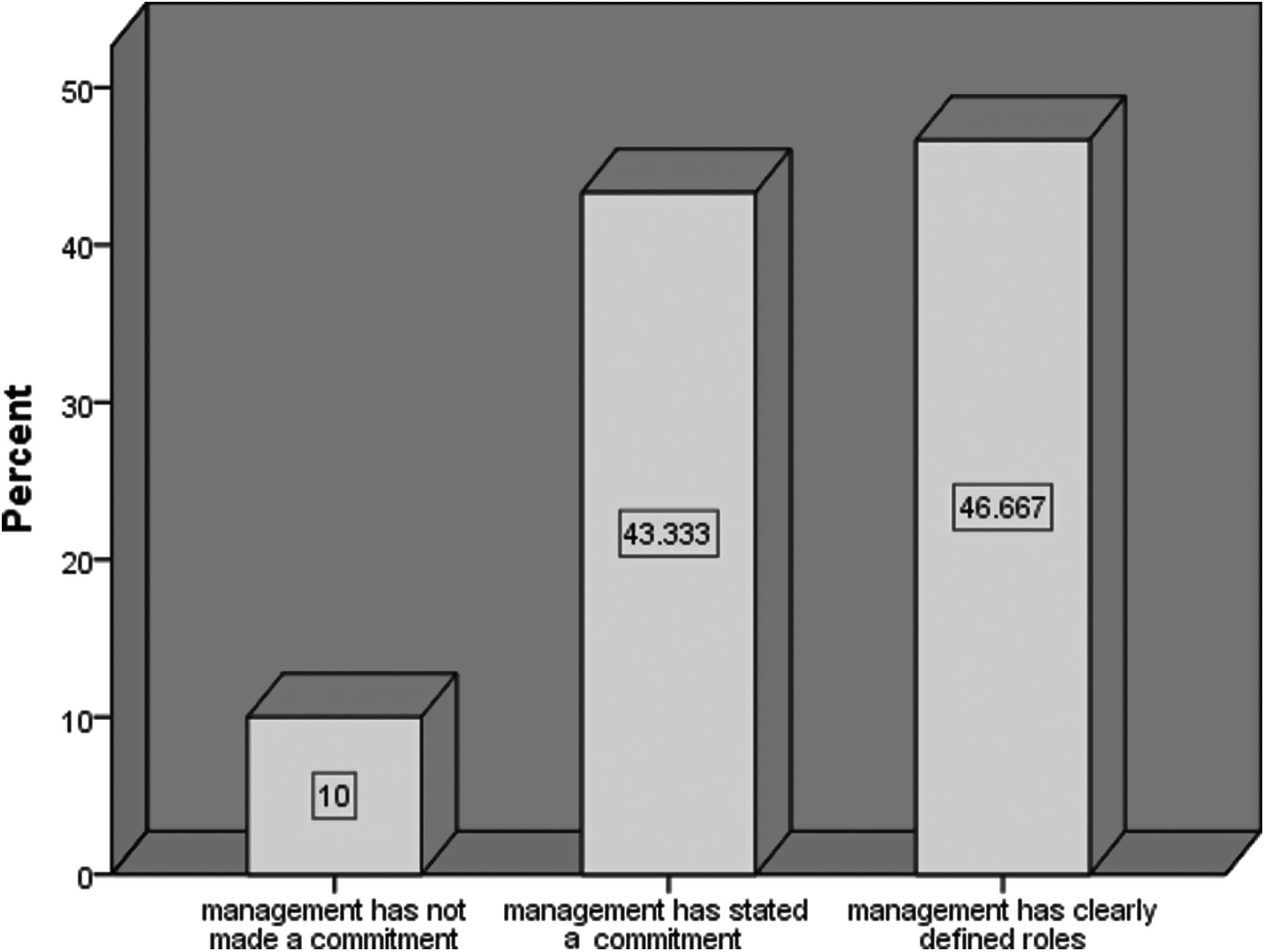
Level of biorisk management in place in various institutions
International Biosafety Guidelines
Regarding biosafety policies and guidelines, 50% (n = 15) of the laboratories follow World Health Organization (WHO) guidelines, 12 26.7% (n = 8) follow Biosafety in Microbiological and Biomedical Laboratories (BMBL) guidelines, 13 and 1 (3.3%) has its own policies; 16.7% (n = 5) do not follow any biosafety policies or guidelines (Figure 2). It was interesting to find in cross tabs distribution that 80% of the clinical/biomedical labs follow WHO laboratory biosafety guidelines, while 20% do not follow any biosafety guidelines. Of the university hospital labs, 80% follow BMBL guidelines, while the remaining 20% follow other guidelines (mostly WHO). Half of the animal labs follow the WHO biosafety manual, while 50% do not follow any specific guidelines. Of the R&D labs, 25% follow WHO laboratory biosafety guidelines, 50% follow BMBL, 3.3% follow their own laboratory's SOPs, and 16.7% follow various biosafety policies or did not have any prior knowledge of biosafety policies and guidelines (Figure 2).

Biosafety guidelines followed by institutions
Biosafety Officer
The placement of a biosafety officer in a facility is important for safeguarding the employees, as it ensures labs adhere to biosafety practices. We found that 70% of the facilities have assigned the responsibility of a biosafety officer in their institute, while only 3.3% also have assigned responsibility to different related personnel. While 80% of the facilities have assigned the role of biosafety officer to laboratory managers and 13.3% to a scientific manager, 86.7% of facilities have assigned the role of biosafety officer to microbiologists, and 70% of the facilities have given this role to pathologists (Table 3). The biosafety officer is responsible for promoting a culture of safety according to his or her expertise in biosafety and biosecurity, which enables a facility or institute to curb the unintentional or intentional misuse or exposure of potentially infectious material and to prevent incidents in the laboratory environment.
Assignment of Roles and Responsibilities Related to Biosafety and Biosecurity
Biosafety Facilities
The study found that 86.6% (n = 26) of the laboratories have posted biohazard signs, while 13.3% (n = 4) of the labs do not have any warning signs outside of their laboratories. Regarding the availability and use of primary containment biosafety cabinets (Class II), the questionnaire showed that in 10% of the laboratories, primary containment biosafety cabinets did not exist at all, while in 30% of the laboratories primary containment biosafety cabinets were present, but they were used only periodically; in 60% of the laboratories, primary containment biosafety cabinets (Class II) were used consistently (Figure 3). However, the proper annual field certification for biosafety cabinets as per the NSF 49 standard were not done in the facilities, as NSF-certified professionals are not currently available and trained in Pakistan. This function is currently performed by engineers referred by the vendors of biosafety cabinets.
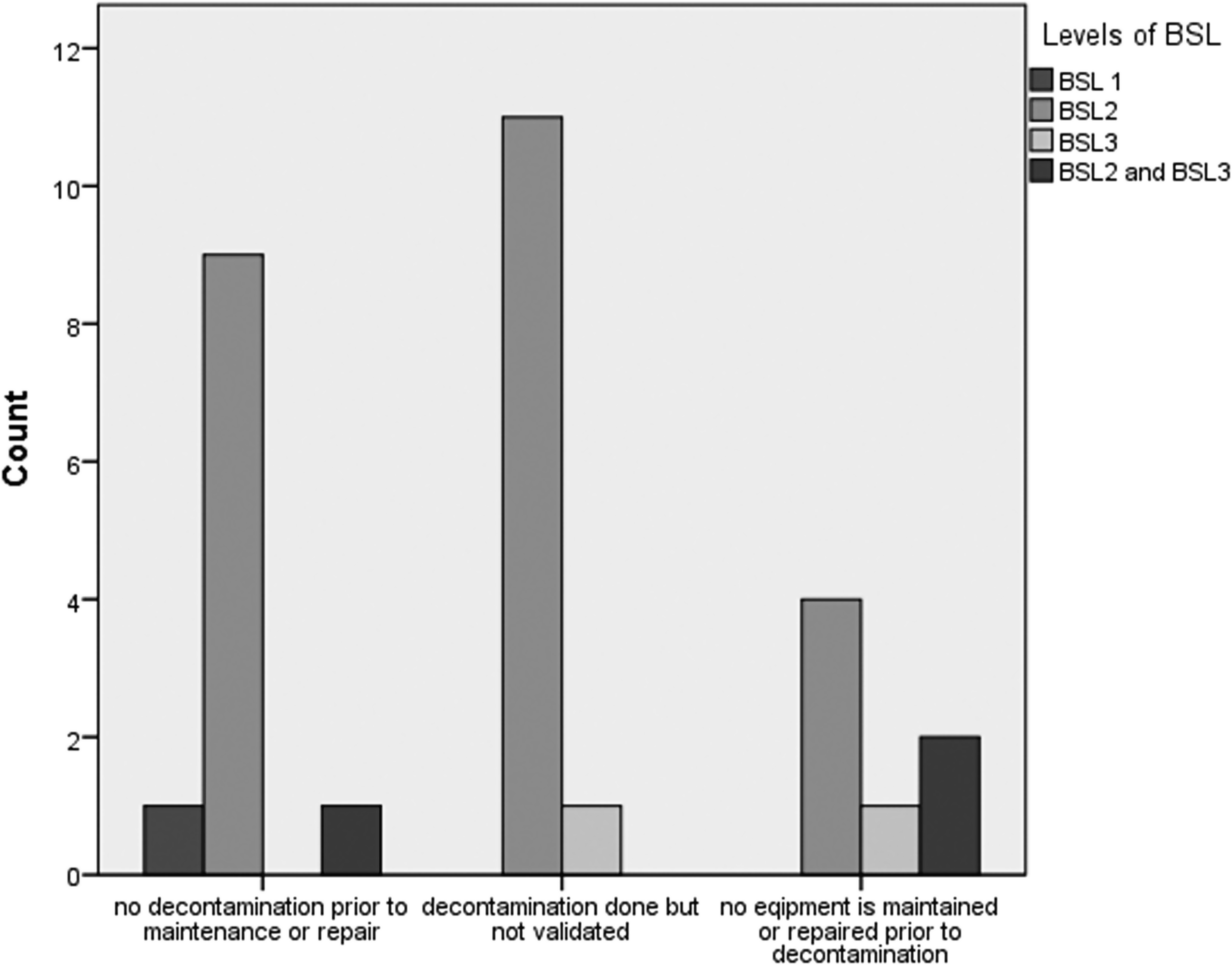
Biosafety compliance and equipment decontamination procedures in laboratories
Personal Protective Equipment
Assessments regarding the compliance with biosafety measures revealed that in 50% of the facilities there is strict compliance with biosafety measures, while in 43.3% of the facilities biosafety measures are often not put into practice, and in 6.6% biosafety measures are not respected at all. Forty percent of the laboratories have active personal protective equipment (PPE) programs (eg, lab coats, gowns, gloves, face masks) with clearly defined procedures; 53.3% have some procedures regarding PPE but lack oversight in implementation; and 6.6% of laboratories have limited resources for PPE. Proper use of PPE can be effective in limiting the incidents of LAIs if used and maintained properly.
Equipment Decontamination
It was observed that equipment maintenance or repair is not up to standard, and it was seen that in BSL-2 laboratories there is no decontamination prior to maintenance or repair of laboratory equipment. Among the 30 surveyed laboratories, 11 were not following decontamination procedures for maintenance and repair, and among them 9 were BSL-2 laboratories. Twelve laboratories were following decontamination procedures but do not validate it; among them 11 were BSL-2 facilities. In addition, in 7 remaining laboratories, of which 4 were BSL-2, there was proper decontamination prior to maintenance and repair (Figure 3). This could important in preventing LAIs if done properly before maintenance.
Occupational Health
Assessment of the occupational health programs of institutes reveals that 23.3% of facilities have protocols for annual medical examination of employees, 50% provide vaccinations, and 96.7% conduct baseline medical examinations and require employees to report illnesses. However, none of the institutes has any system for serum banking. Data regarding preventive measures against bloodborne pathogens show that 46.6% of the facilities were following the bloodborne pathogen standard of the US Occupational Safety and Health Administration (OSHA, 1910:1030), while 23.3% were not following it, and 30% of the facilities were not even familiar with it. Table 4 shows the prevailing status of occupational health programs in these facilities. Increased awareness is an immediate need, in addition to some regulatory intervention.
Occupational Health Program Activities Required by the Institution
Risk Assessment
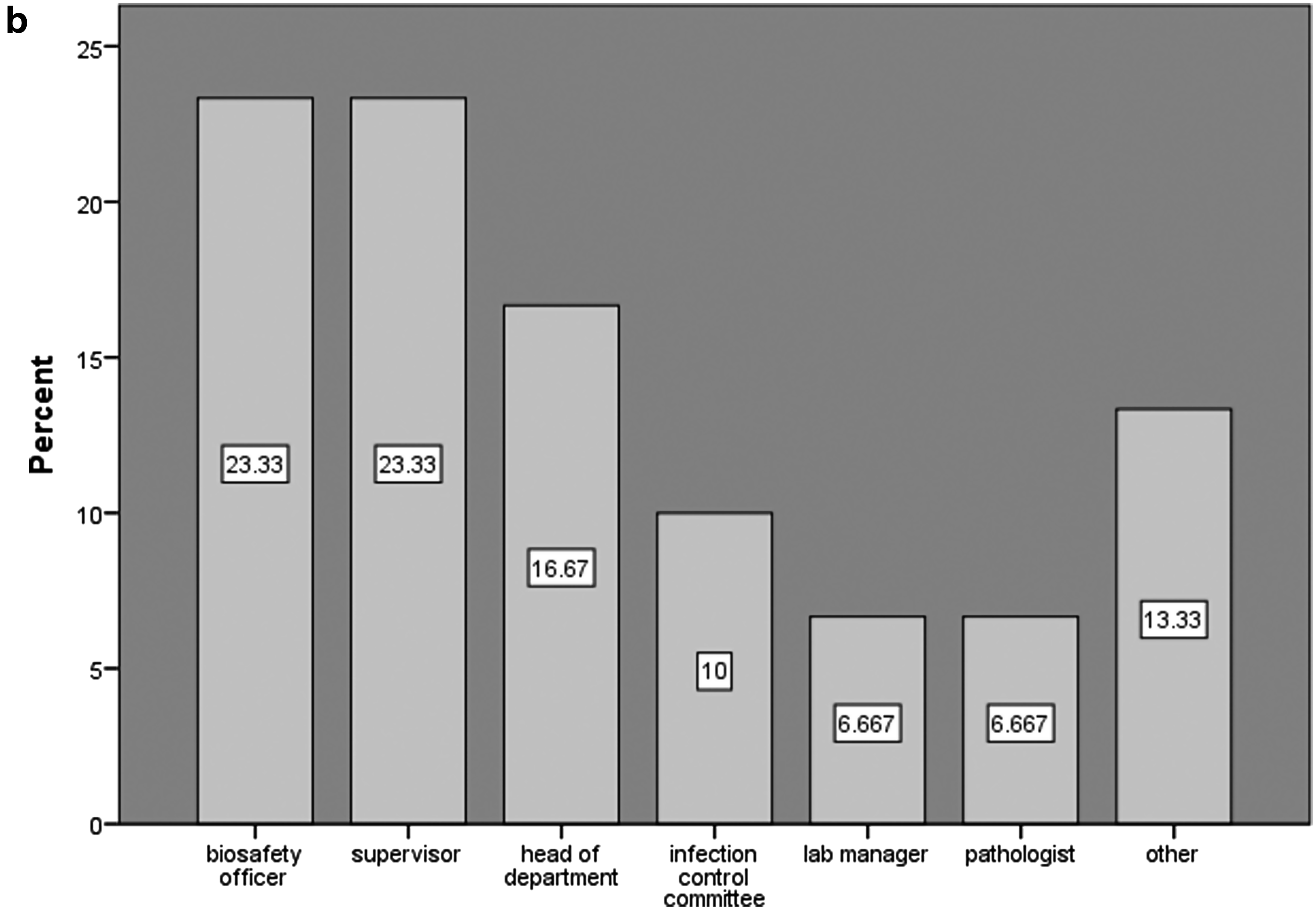
Seventy percent of facilities were not aware of the importance of risk assessments; 30% have protocols for risk assessment before starting any new procedure or on a routine basis, and they have SOPs for risk assessment before adopting new procedures, which is mostly done by committees or professionals such as an infection control committee (13.3%), a biosafety officer (6.6%), or a microbiologist, pathologist, lab manager, or institutional biosafety committee (3.3%). A total of 63.3% of the institutes report having policies and procedures in place for incidence reporting that are strictly followed; 30% have policies but they are often not followed, while 6.6% of the institutes do not have any policies for incident reporting. In 23.3% of the facilities, incidents were first reported to a biosafety officer and supervisor, followed by the head of the department (16.6%), an infection control committee (10%), and the lab manager and pathologist (6.6%). However, in 23.3% of the facilities, no follow-up steps are taken, while 76.6% provide immediate medical surveillance and generate a report, 66.7% also do follow-up check-ups, and 63.3% take corrective measures. This could result in prolonged absence of an individual from duty and have an effect on his or her economic well-being.
In all of the BSL-1 laboratories, there is no SOP for risk assessment; 70.8% of the BSL-2 laboratories, 50% of the BSL-3 laboratories, and 66.7% of the facilities that have both BSL-2 and BSL-3 laboratories have no SOP for risk assessment before adopting new procedures (Figures 4a and 4b).
Risk assessment strategy
Incidence response plan
Procedure Performed
More than 90% of the institutes perform a variety of procedures (Table 5) that generate aerosols and droplets, such as mixing/vortexing (96.7%), as well as separating needles from syringes (76.7%), decanting liquid specimens (93.3%), and spilling infectious material (73.3%).
Procedure Performed in Institution Producing Aerosols and Droplets
Laboratory Incidents
Needlestick was found to be the most common injury in 76.7% institutes, followed by animal bite/scratch (13.3%), cut on mucous membrane (3.3%), and falls and burn injuries (3.3%). Subcutaneous needlestick injury was the most common needlestick injury in 60% of the facilities, while for rest of the facilities, the site of the needlestick injury was not determined (Table 6).
Most Common Injuries in the Institution
Standard Operating Procedures
Assessment of SOPs for needlestick injury show that in 60% of the institutes, there is an SOP for needlestick injury that is strictly followed, while 23.3% of the institute have an SOP but it is often not followed; in 16.7% of the institutes, there is no SOP at all (Figure 5).
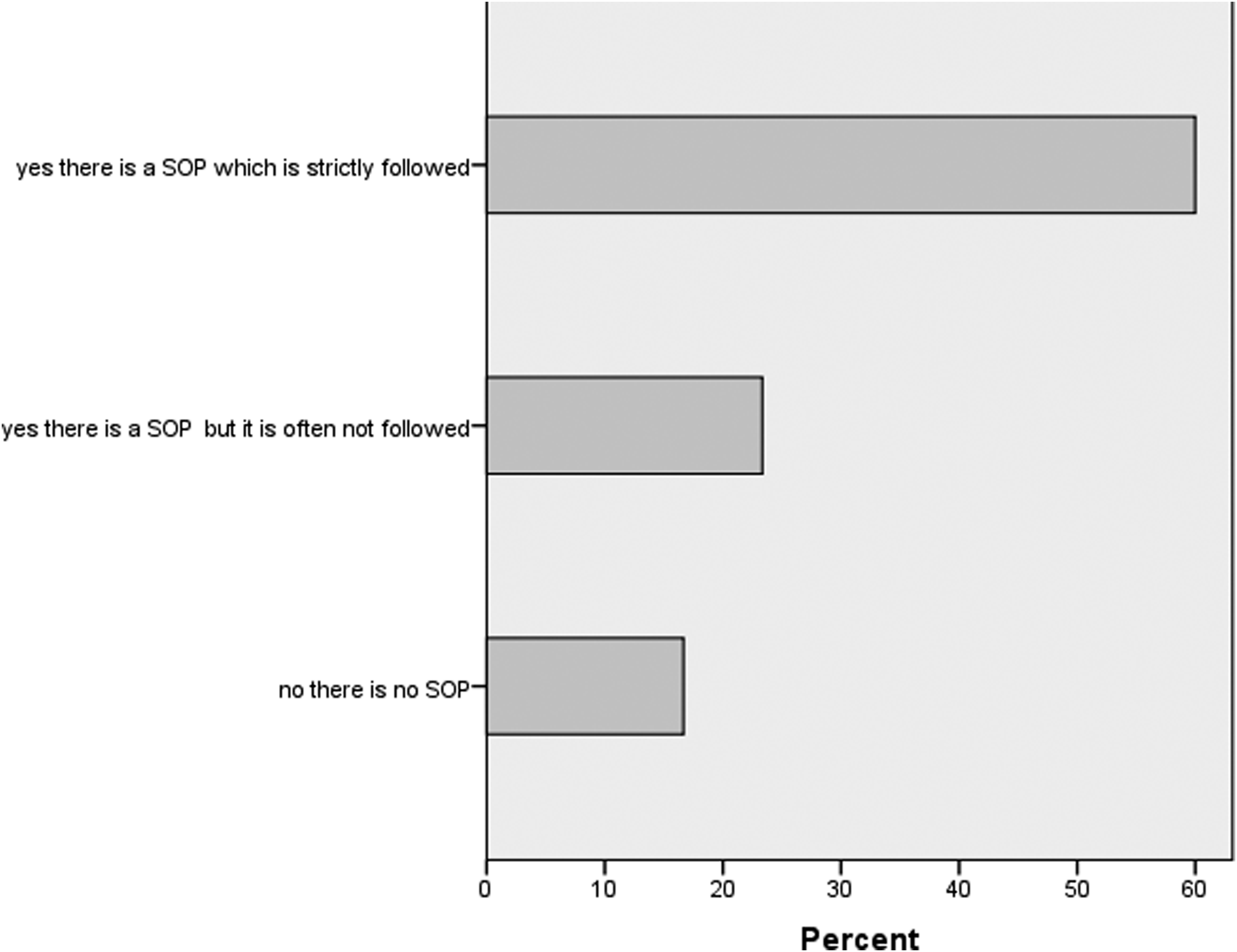
Presence and compliance with SOP for responding to a needlestick injury in various institutions
Transmission Routes
In the laboratories visited, 33 cases of suspected LAIs were reported. Of these 33 cases, 13.3% were transmitted by inhalation and percutaneous inoculation; for 83.3% of the cases, transmission routes were unknown as there was no proper system in place to determine the transmission routes of LAIs. Data regarding the potential causes of suspected LAIs in the surveyed facilities revealed that no or low compliance with biosafety measures was the cause of LAIs in 23.3% of cases. Causes included lack of knowledge regarding the biorisk related to an activity, lack of attention, a too heavy workload (in 6.7% cases), and not enough training (in 13.3% of cases) (Table 7). In addition, 73.3% of the participants said that the cause of suspected LAIs is unknown, which reflects a lack of training of participants.
Transmission Routes and Potential Causes of LAIs
Incident Reporting
Data regarding activities that resulted in suspected LAIs reveal that 5 of the individuals received an LAI by needlestick injury and 1 from subculturing in a microbiology lab. In 5 individuals it was proven that the infection was work-related based on an investigation done in their respective laboratories. In the case of 26.6% suspected LAIs, the infection was not transmitted to another person, while for 73.3% it was not known whether it was transmitted to another person or not.
Pathogenic strain was identified in only a few cases of inhalation as Mycobacterium tuberculosis. Percutaneous infections were mainly hepatitis C; others were not identified, because for LAIs there was no protocol in place for incident reporting and further investigation up to the level of organism identification. This needs to be addressed properly to ensure the safety of people working in laboratories and to examine the risk group for that organism, which will help in developing proper preventive and treatment modalities for a functional and effective medical surveillance program.
In 12.5% of the R&D laboratories, there is no policy for incident reporting. However, 26.7% of clinical laboratories, 60% of the university hospital laboratories, and 25% of the R&D laboratories have procedures for incident reporting, but they are not strictly followed. In 73.3% of the clinical laboratories, 40% of the university hospital laboratories, and 62.5% of the R&D laboratories, there is a strict policy for incident reporting (Figure 6).
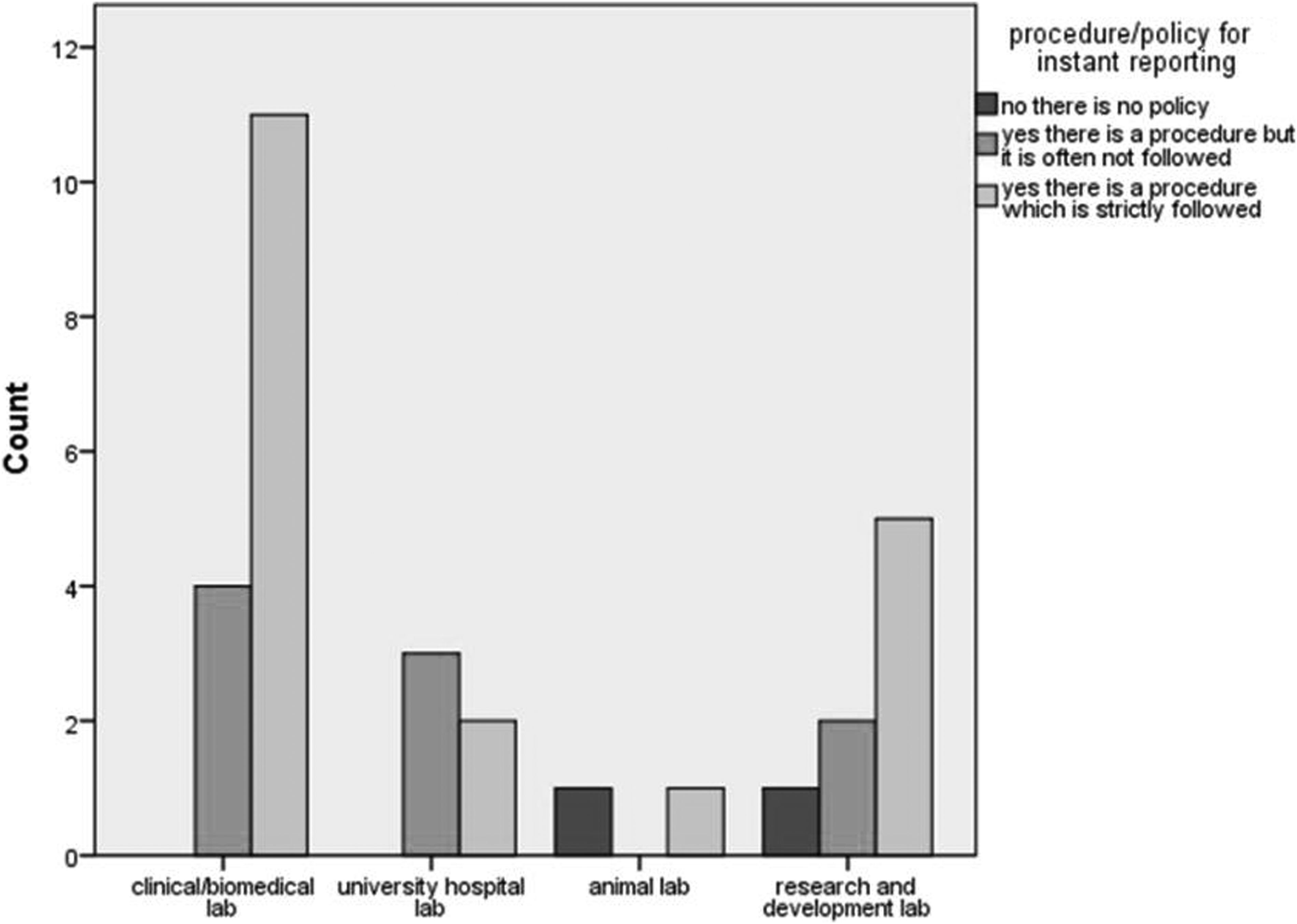
Procedure/policy followed by institutes for incident reporting
Individual Vulnerability
The most vulnerable individuals identified in the laboratory environment in this survey were pathologists, laboratory technicians, researchers, and housekeepers (Table 8).
Healthcare Professionals Infected with LAIs
Exposure
In 16.6% of the LAIs, there were no reported physical disabilities or severe illnesses in the infected individuals, while 10% of the LAI cases caused a reported physical disability or severe illness for more than 20 days. No fatalities have been reported in relation to LAIs in any institute. In 10% of the facilities, exposure to LAIs has been reported, while in 26.7% of the laboratories, infection was reported postexposure, which may be due to inappropriate biosafety measures resulting in inadequate reporting of incidents (Figure 7).
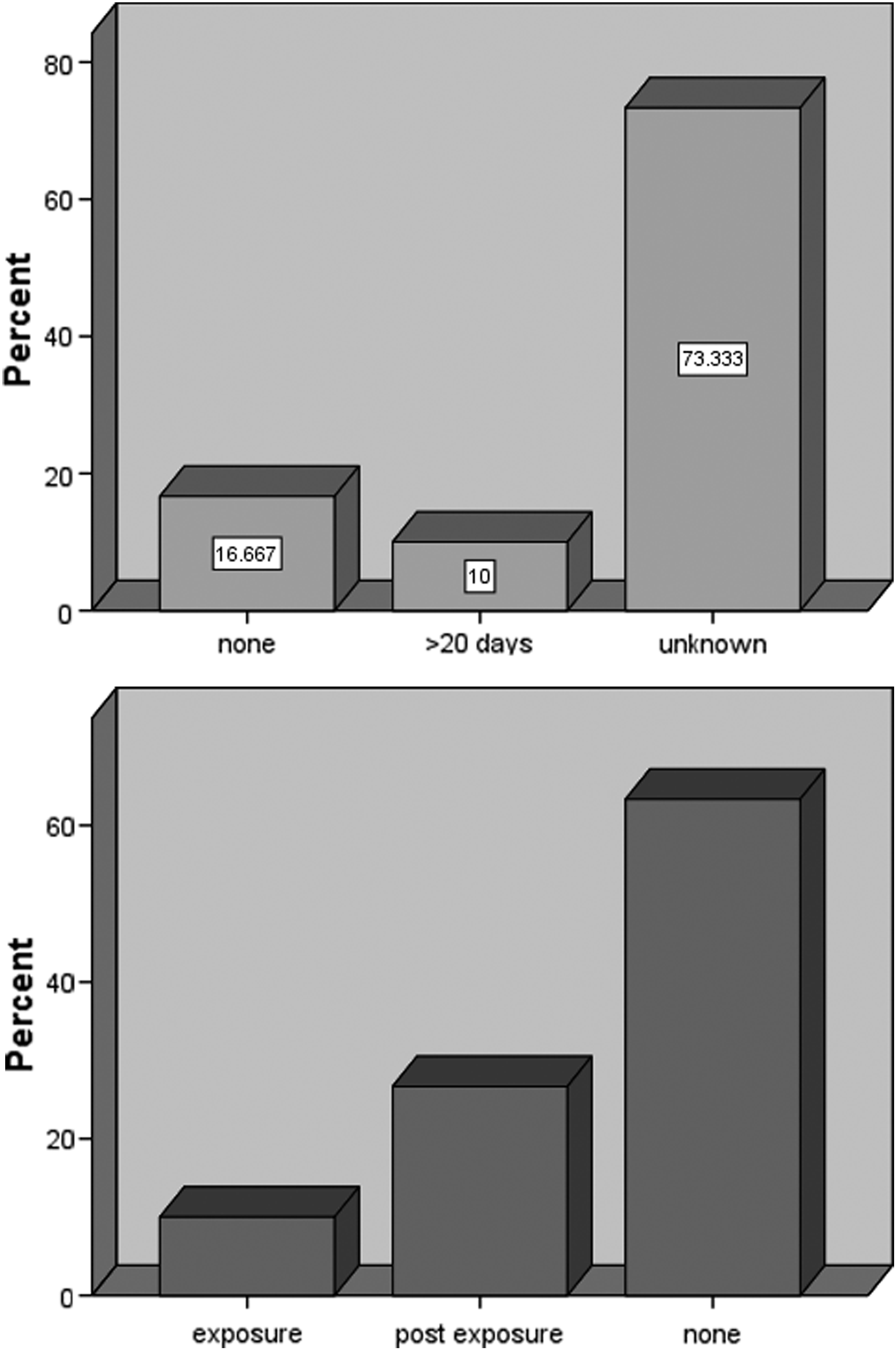
Days of disability and reporting of exposure in institutions
Medical Surveillance
Overall, 40% of the clinical laboratories, 60% of the university hospital laboratories, and 12.5% of the R&D laboratories have functional medical surveillance programs, while none of the animal facilities have any medical surveillance program in place (Figure 8).

Existence of functional medical surveillance program in the surveyed laboratories
Discussion
Laboratory-acquired infections can occur is any facility that deals with biological agents. However, determining the source of LAIs can be difficult without an effective system in place to investigate LAIs, 14 which is also the case for our surveyed facilities, since most of them do not have effective protocols to determine LAIs. Laboratory-acquired infections are an important public health concern globally, since infected workers can further spread an infection into the community and become the source of future outbreaks.
Laboratory-acquired infections are often not reported or are underreported, because having an incidence of LAI can affect the reputation of the organization, and the organization could face negative consequences. 15 This is also reflected in our results, as this study identified only a few reported LAIs. Another reason for underreported LAIs could be that the organizations we surveyed were dealing with risk group 2 organisms in most of the labs, in contrast to the facilities studied by Pike et al, 3 where most of the organisms were from risk group 3—that is, the LAIs from risk group 2 had occurred but they were not documented since these infections cause mild to moderate diseases that sometimes do not show obvious clinical manifestations or are delayed. The signs and symptoms often go unnoticed, because the laboratory professionals are mostly not educated about the signs and symptoms of the diseases caused by the pathogens they are working with.
In addition, risk assessment is a joint effort and needs input from different stakeholders in the lab, while our results show that only 1 individual at a time was involved in risk assessment; this compromises risk assessment by limiting it to a single person's knowledge and experience rather than the actual risk. It was also noted that the presence of SOPs did not ensure compliance, which reflected gaps in administration and leadership. Thus, when an infection occurs, it fails to be linked with the pathogens in the labs. It is evident that some of the LAIs, especially those that do not cause severe diseases, remain unnoticed and are not reported due to inadequate biosafety protocols in the laboratories. 13
The most common routes of LAIs are percutaneous inoculation (needlestick, broken glass, animal bites or scratches), inhalation (aerosols), ingestion (eg, by smoking, eating, aspiration through a pipette), direct contact between contaminated surfaces (gloves, hands), and through mucous membranes. 16 Therefore, the route of transmission and minimal infective dose for infection should be the focuses while doing the risk assessment to prevent and control infections in laboratory workers. 17 Historically, inhalation has been the most common route for transmission of LAIs. 3 However, in our study transmission routes for most of the LAIs were unknown, which may indicate an inhalation route, while for a few cases, inhalation and percutaneous inoculation by needlestick injury were identified as a result of lack of biosafety compliance and training.
In our surveyed laboratories, most of the LAIs were reported from the microbiology labs, while many surveys have been conducted that reported various LAIs from different bacteria, viruses, and parasites and fungi. In the United Kingdom, enteric infections such as shigellosis and tuberculosis have been found to be the most common LAIs in clinical laboratory workers.4,5 Another survey from 1994-95 reported the predominance of gastrointestinal infections (shigellosis). 18 A clinical laboratory survey in Utah from 1978 to 1992 also reported shigellosis as the most common LAI. 19 These reports show a changing pattern of LAIs from early reports with the predominance of enteric infections. A 2000 study reported Brucella spp., Mycobacterium tuberculosis, Salmonella spp., Shigella spp., Escherichia coli 0157:H7, Francisella tularensis, hepatitis B virus (HBV), human immunodeficiency virus (HIV), hepatitis C virus (HCV), and the dimorphic fungi as the most common organisms involved in LAIs. 20 The American Society for Microbiology (ASM) sponsored an online survey in 2002-2004 of clinical laboratories; 33% of the participating laboratories reported at least 1 LAI. They also reported shigellosis, salmonellosis, and brucellosis as the 3 most common organisms for LAIs. 21 The Baron and Miller survey in 2008 also reported Shigella, Brucella, Staphylococcus aureus, and Salmonella as the main agents of LAIs. 20 In 2009 Singh et al reviewed the previous surveys and found that among bloodborne pathogens, HIV, HBV, and HCV are the major causes of LAI among viral infections, while dimorphic fungi caused the largest number of LAI in fungal infections. 20 However, the LAIs reported in our study are not from these enteric bacteria. The difference could be the ineffective system for the determination of LAIs as described. This study provides the pilot data to identify the gaps for implementation of a biorisk management system to safeguard laboratory workers from LAIs and highlights the critical need for reporting and investigating infections in lab professionals.
Conclusion
We believe that this was the first-ever study focused on LAIs in Karachi, Pakistan. This study has identified the gaps in the biosafety and biosecurity practices in various laboratories, including human, animal, and research, biomedical, and university hospital laboratories. These data will help us to focus on standard microbiological practices, special practices, use of PPEs, primary barriers, and facility design in identifying the root causes of LAIs and why they have not received enough attention in Pakistan.
In this survey most of the laboratories were affiliated with academic or university facilities and are dealing with bacteriology. Most of the laboratories have started a commitment to the implementation of biosafety in the facility and are following WHO or BMBL as guidelines. However, commitment to laboratory biosecurity is extremely low in most of the facilities, and they lack proper occupational health and medical surveillance programs. There is a serious gap in the risk assessment strategy that must be addressed before adopting any diagnostic/research processes in the laboratories surveyed.
We have also found serious gaps in effective SOPs to determine and regulate LAIs. Inhalation and percutaneous inoculation were found to be the major source of LAIs, and most of the LAIs were caused by HCV and Mycobacterium tuberculosis, which is highly endemic in our country. Most of the clinical and university hospitals have BSL-2 laboratories. University hospital laboratories were found to be the most committed to biosafety management. The WHO biosafety manual was followed in most of the clinical laboratories, while most of the university hospitals follow BMBL guidelines for biosafety. In light of our findings, we would recommend the following:
Develop and implement guidelines for labs to implement a medical surveillance program for staff. Use a data driven approach to making policy and smart investments to lab biorisk management capacity and biosafety competence of lab professionals. Formulate and carry out a national-level program so that sensitization with reference to LAIs is prioritized, and conduct workshops at frequent intervals to bridge this gap.