
Abstract
In spring 2011, the Centers for Disease Control and Prevention (CDC) released Public Health Preparedness Capabilities: National Standards for State and Local Planning. The capability standards provide a framework that supports state, local, tribal, and territorial public health agency preparedness planning and response to public health threats and emergencies. In 2017, a project team at the CDC Division of State and Local Readiness incorporated input from subject matter experts, national partners, and stakeholders to update the 2011 capability standards. As a result, CDC released the updated capability standards in October 2018, which were amended in January 2019. The original structure of the 15 capability standards remained unchanged, but updates were made to capability functions, tasks, and resource elements to reflect advances in public health emergency preparedness and response practices since 2011. When the number of functions and tasks in the 2018 capability standards were compared to those in the 2011 capabilities, only 20% (3/15) of the capabilities had a decrease in function number. The majority of changes were at the task level (task numbers changed in 80%, or 12/15, capabilities) in the 2018 version. The capability standards provide public health agencies with a practical framework, informed by updated science and tools, which can guide prioritization of limited resources to strengthen public health agency emergency preparedness and response capacities.
In 2011, the CDC released public health preparedness standards, which provide a framework for state and local preparedness planning and response to public health threats and emergencies. They have since been updated and provide public health agencies with a practical framework, informed by updated science and tools, that can guide prioritization of limited resources to strengthen public health agency emergency preparedness and response capacities.
The public health emergency preparedness and response capability standards (hereinafter referred to as capability standards) have strengthened our nation's ability to prepare for and respond to public health emergency incidents. 1 Recent public health crises, such as the Ebola and Zika virus outbreaks, and other incidents, such as wildfires and hurricanes, underscore the need for public health agencies to adapt to an ever-expanding list of public health threats and emergencies. 1 Improved practices should be implemented before the infrastructure becomes overwhelmed or mortality rises. Implementing improved public health emergency management practices, aligned with criteria supported in the capability standards, has the potential to mitigate the adverse consequences of emergency incidents, such as an increase in morbidity and mortality, and to promote community resilience.
In 2001, the US government recognized that the nation's public health system was unprepared for man-made or natural catastrophes of a large magnitude.2,3 (A timeline of key events is shown in Figure 1.) In 2002, the Centers for Disease Control and Prevention (CDC) provided guidance and funding to 50 states, 4 cities, and 8 US territories or freely associated state public health agencies to improve public health preparedness and response capacity.3,9 Initially, focus areas were preparedness planning and readiness assessment, surveillance and epidemiology capacity, laboratory capacity for biological and chemical agents, the Health Alert Network 10 as a component of communications and information technology, risk communication and health information dissemination, and education and training. In subsequent years, CDC transitioned funding priorities from specific “focus areas” to a capabilities-based framework. 11

In 2005, the US Department of Homeland Security (DHS) released the Target Capabilities List, an all-hazards preparedness framework to guide operational readiness planning, priority setting, and program implementation nationwide.4,12 This DHS framework, along with the 2006 Pandemic and All-Hazards Preparedness Act (PAHPA), the 2008 Institute of Medicine report (to identify focus areas for systems research), 13 and the 2009 National Health Security Strategy (NHSS), provided the foundation for the development of CDC capability standards for state, local, tribal, and territorial preparedness and response. 12
In spring 2011, CDC's Division of State and Local Readiness released Public Health Preparedness Capabilities: National Standards for State and Local Planning; a novel set of capability-based planning standards for public health agencies. 12 Nine of the original 15 capability standards were designated as Tier 1 capabilities, which are foundational to public health. 12 The remaining Tier 2 capabilities generally rely on having established Tier 1 capabilities in place to achieve cross-cutting preparedness and response activities. 12 However, in subsequent years, all 15 capability standards were incorporated into jurisdictional public health agency emergency preparedness programs for capacity building, as requested by the CDC cooperative agreement during funding allocations.1,11,12
Over time, the original capability standards emerged as a broader framework that helped public health agencies prioritize emergency preparedness planning, define jurisdictional preparedness and response roles, provide suggestions for partner and stakeholder collaboration, standardize nomenclature and terminology, and integrate exercise and evaluation planning.12,14 Since the standards were developed, CDC has actively encouraged public health agencies to incorporate routine activities into capability-based demonstration projects (in addition to preparedness training, drills, and exercises) as a way to test and evaluate jurisdictional public health emergency preparedness and response capacities.11,15
The practice of public health emergency preparedness and response has continued to mature since 2011, highlighting the need to update the capability standards as a result of advances and increased knowledge in the field of preparedness. 16 For example, Savoia et al conducted a 2009–2015 systematic review that provided additional support to the Institute of Medicine report findings—that is, training, communications, response systems, and effectiveness criteria and metrics are the 4 focus areas for public health emergency preparedness system research. 17 Other evidence, including research outcomes from preparedness emergency response research centers, 18 similarly suggested that the capability standards be researched to assist in filling preparedness practice knowledge gaps.1,17,18
In spring 2017, CDC initiated a comprehensive review of the 2011 capability standards. 1 Principal goals for updating the capability standards were to revise emergency preparedness and response content based on perceived gaps and to account for scientific and practice advances developed since 2001. 19 In October 2018 (amended in January 2019), CDC released the updated capability standards and retitled the document Public Health Emergency Preparedness and Response Capabilities: National Standards for State, Local, Tribal, and Territorial Public Health. 19 Here we describe the processes used to update the CDC capability standards.
Methods
Definitions
The capability standards are intended to build and advance public health capacity. This is accomplished by collaborating with partners and stakeholders to strengthen the security and resilience of the United States. 19 The capability standards provide a framework to enable jurisdictions to prepare for and respond to any public health emergency by means of recommended functions, tasks, and resource elements. Capability functions define critical elements of a capability that must occur to achieve each capability standard; capability tasks are action steps that relate to implementing 1 or more capability functions; and capability resource elements are resources, such as skills and training, equipment and technology, and operational procedures, that jurisdictions need to have (or have access to) to accomplish capability tasks associated with capability functions. 19
Update Process
The Division of State and Local Readiness designated a project team to coordinate and oversee updates to the capability standards. The project team reviewed literature published since 2011 (eg, the core capabilities by the Federal Emergency Management Agency, or FEMA 20 ), the National Response Framework (Emergency Support Functions #8), 21 the Public Health Accreditation Board Standards and Measures, Version 1.5, 22 the Project Public Health Ready criteria, 23 and numerous other guidance and policy documents. In addition, the project team reviewed existing Tier 1 and Tier 2 capability designations, performance measure data, suggested training resources and web links, an internal staff survey, and an assessment conducted by Avar Consulting (Rockville, MD) 1 to scope potential updates to the capability standards. The Avar report findings, later published by Horney et al, concluded that the capability standards should be updated but their structure should essentially remain the same. 1
As a result, 15 work groups were formed, 1 for each capability standard, to review and recommend content changes. Four additional work groups were established to address the cross-cutting topics of pandemic influenza, tribal populations, vulnerable (at-risk) populations, and environmental health. Work groups included experts from CDC (various centers and program offices), FEMA, and the Office of the Assistant Secretary for Preparedness and Response (ASPR) at the US Department of Health and Human Services (HHS) (Figure 2). A 3-phase project plan was organized: phase 1, subject matter expert engagement; phase 2, national partner and stakeholder engagement; and phase 3, dissemination of the final version (Figure 2).
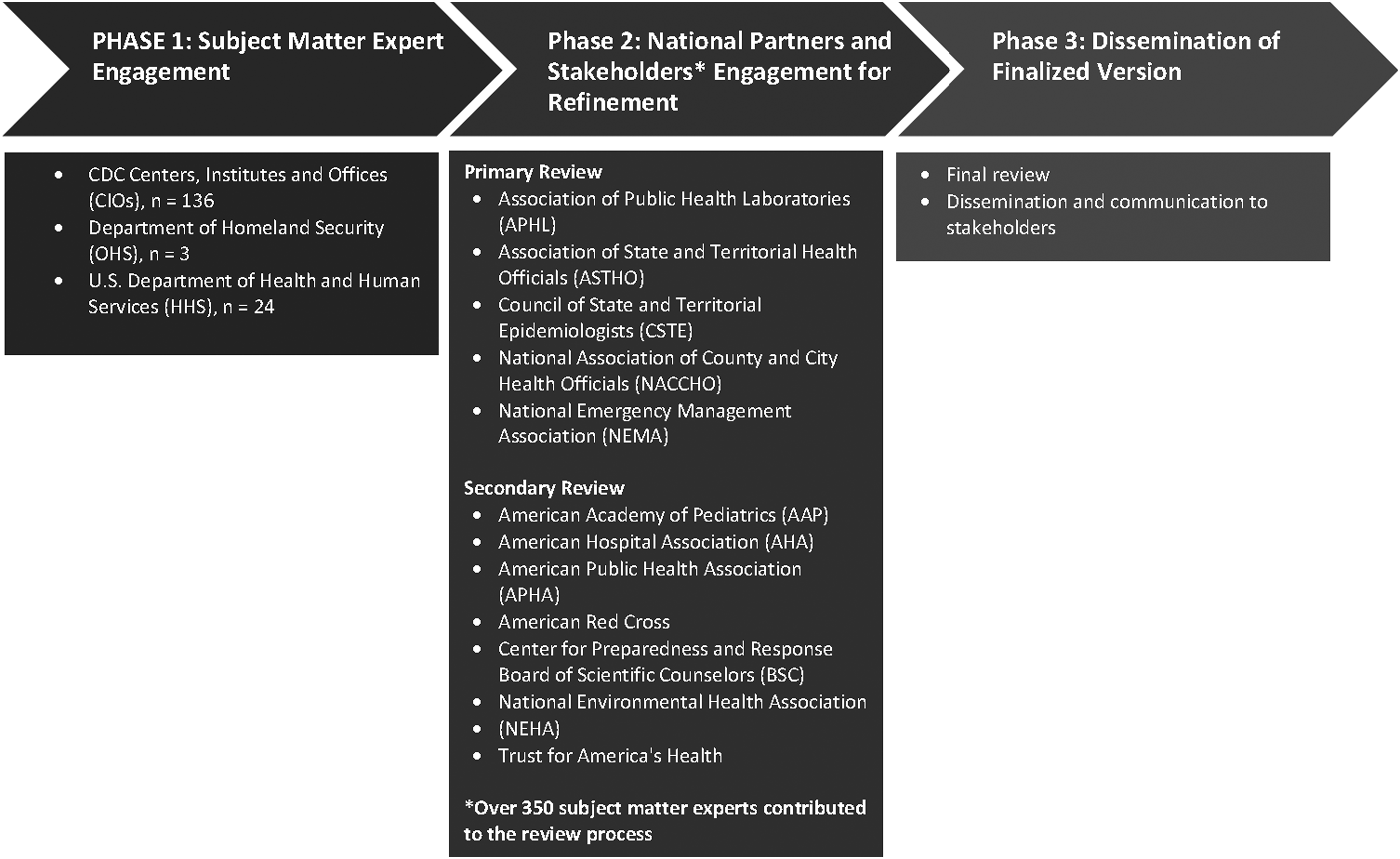
Process and major informants used to update the capability standards
Phase 1. Subject Matter Expert Engagement
The subject matter expert work group consisted of preparedness and response practitioners and experts from various federal agencies, such as CDC, FEMA, ASPR, and HHS. They reviewed the 2011 version of the capability standards, funding, recipient performance measure data collected by the Division of State and Local Readiness, existing preparedness training and education resources, and other relevant content to identify gaps in public health preparedness and response planning. For approximately 2 months, work group members participated in weekly or biweekly sessions to adjudicate and deliberate on findings and to recommend updated content for each capability standard. Subject matter expert input ensured that updated content aligned with current practices and standards, including those pertaining to the discipline of public health emergency management.
The workgroup included experts in at-risk populations, community preparedness, community recovery, cybersecurity, data exchange, environmental health, emergency management and operations, epidemiology, global migration, healthcare preparedness, health studies, infection control, infectious diseases, informatics, laboratory practice, surveillance, medical countermeasure dispensing and medical materiel management, occupational health, toxicology, vaccination, worker safety, and other public health topics.
Phase 2. National Partners and CDC Stakeholder Engagement
In phase 2, national partners and stakeholders reviewed draft updates of the capability standards. Reviewers were invited to provide input on the updated capability standards through a formal email soliciting participation, sent by leaders from the Division of State and Local Readiness. As a part of the process, selected national partners further redistributed the updated drafts for comment to numerous individuals in state and local organizations (Figure 2). The Association of Public Health Laboratories, the Association of State and Territorial Health Officials, the Council of State and Territorial Epidemiologists, the National Association of County and City Health Officials, and the National Emergency Management Association served as primary coordinating partners. Secondary coordinating partners included the American Academy of Pediatrics, the American Hospital Association, the American Public Health Association, the American Red Cross, the CDC Center for Preparedness and Response Board of Scientific Counselors, the National Environmental Health Association, and the Trust for America's Health. These partnerships helped CDC to identify and adjudicate recommendations for inclusion in the updated capability standards. Individual reviewers and partner organizations emailed recommendations to the CDC (no consensus was sought from individuals and/or partner organizations). More than 350 subject matter experts contributed to the secondary review process.
Phase 3. Dissemination of the Final Version
Following additional review by various levels of CDC leadership and subject matter experts, CDC published the updated capability standards in October 2018. 19
Results
The Division of State and Local Readiness project team updated the 15 public health emergency preparedness and response capability standards based on recommendations from partners, stakeholders, and subject matter experts. Primary update recommendations concentrated on incorporating current science and public health practice into the capability standards. The project team and subject matter experts aligned the capability standards with other national guidance—for example, FEMA's core capabilities, 20 FEMA's National Response Framework (ESF#8), 21 Public Health Accreditation Board Standards and Measures Version 1.5, 22 and Project Public Health Ready criteria 23 —while maintaining the existing capability organizational structure. Ultimately, capability definitions remained mostly unchanged, but significant revisions were made to functions, tasks, and resource elements. Table 1 describes overarching updates for each capability standard. Table 2 compares the number of functions and tasks in the capability standards from 2011 to 2018.
Updated themes included in the revised public health emergency and response capability standards, 2018
The tier designates the level of capacity building that CDC recommends to state, local, tribal, and territorial public health agencies. Tier 1 has the highest foundational level in public health management. The complete list of capability standards is available at https://www.cdc.gov/cpr/readiness/capabilities.htm.
Note. ADA = American with Disabilities Act; ASPR = Assistant Secretary for Preparedness and Response; CDC = Centers for Disease Control and Prevention; DMORT = Disaster Mortuary Operational Response Team; EMAC = Emergency Management Assistance Compact; ERHMS™ = Emergency Responder Health Monitoring and Surveillance™; ESF = Emergency Support Function; FM = fatality management; HPP = Hospital Preparedness Program; HHS = US Department of Health and Human Services; LRN = Laboratory Response Network; MCM = medical countermeasure; MS = medical surge; NDRF = National Disaster Recovery Framework; PPE = personal protective equipment.
Number of functions and tasks in the 2018 capability standards as compared with the 2011 capabilities

NA = not applicable.
Note. Bold designates Tier 1 capabilities. Light grey indicates a decrease in number of functions or tasks, and darker grey indicates an increase in either functions or tasks. The number of functions remained the same in most capabilities (3 to 6 functions per capability). Some capabilities had a decrease in function number (3 out of 15, or 20%, capabilities). Most task numbers changed in the 2018 version (12/15, 80%). When analyzed by capability tier, all Tier 2 capabilities had changes in the number of tasks, whereas only 67% of Tier 1 capabilities had a change in the number of tasks.
The Division of State and Local Readiness project team transitioned the emphasis of the capability standards from a planning focus (2011 version) to an operational focus (2018 version). To reflect this, content focus changed from writing plans in the 2011 version to operationalizing the execution and demonstration of the capabilities in the 2018 version (eg, “procedures in place …” rather than “written plans should include …”). The 2011 title of the document was changed from Public Health Preparedness Capabilities: National Standards for State and Local Planning to Public Health Emergency Preparedness and Response Capabilities: National Standards for State, Local, Tribal, and Territorial Public Health. The new title also takes into account tribal and territorial needs and conveys alignment with the FEMA Preparedness Cycle. 24
The title of capability 8 was changed from “Medical Countermeasure Dispensing” to “Medical Countermeasure Dispensing and Administration” to reflect that medical countermeasures (vaccines and antitoxins) might be administered rather than dispensed (oral antibiotics).
Cross-cutting content (ie, at-risk populations, environmental health, pandemic influenza, and tribal populations) was incorporated throughout each capability, and performance measure requirements previously embedded within the 2011 capability standards were removed, as measurement and evaluation criteria will be specified in future iterations of CDC Operational Readiness Review (ORR) guidance. 25 Currently, the ORR is an evidence-based tool for public health agencies to measure and evaluate preparedness and response planning and operational readiness. 25
Additionally, more than 300 training and educational resources were updated and migrated to CDC's Online Technical Resource and Assistance Center (On-TRAC), an online technical assistance support system. To ensure open access to these suggested resources, the information was also publicly posted on the CDC Division of State and Local Readiness website. 26
As part of an ongoing effort, revised capability standards will continue to be disseminated at national meetings, forums, and conferences, such as the ASTHO Director of Public Health Preparedness meetings, the NACCHO Preparedness Summit, the American Public Health Association's Annual Meeting and Expo, and the Council of State and Territorial Epidemiologists' Annual Meeting. Two webinar presentations to nearly 300 participants were conducted in November 2018, and a presentation hosted in partnership with the Rollins School of Public Health, Emory University, was provided in January 2019. Future presentations for schools of public health are being planned.
Discussion
The science and practice of public health emergency management has matured rapidly in recent years and remains a dynamic, new, and emerging community of practice. Our nation must continue to develop new strategies, technologies, and resources to protect our public health infrastructure and systems from 21st century threats. The nation's public health system and supporting procedures, plans, and practices must be adaptable to address continually evolving challenges. The continuous review of current science and the implementation of public health practices facilitate the provision of up-to-date guidance to jurisdictional public health agencies to improve preparedness planning and incident response.
The 2018 capability standards update information related to equipment acquisition, planning tools, policies, standards, practices, procedures, training, and educational resources and account for the cross-cutting and intersecting program areas of environmental health, pandemic influenza, at-risk populations, and tribal populations. Capability functions, tasks, and resource elements were significantly modified as a part of the capability update initiative to better inform operational planning, skills and training, and equipment and technology tools critical for successful implementation of the capability standards, 19 while the general structure of the 15 capabilities remained unchanged.
CDC's Public Health Emergency Preparedness (PHEP) program funds 62 state, local, and territorial health departments to build and sustain their capability standards. The PHEP program also uses the capability standards as a framework to support program accountability, organize work plans, measure performance, and inform evaluation and an overall research agenda for funding opportunities.11,23,26 Similarly, the 2018 capability standards support jurisdictional prioritization of public health emergency preparedness and response resources, identify opportunities to improve preparedness and response planning, and support implementation of accountability tracking and the development of evaluation criteria and metrics. It is essential that measures of day-to-day effectiveness, surge capacity exercises, and lessons learned from real incident responses be incorporated into routine public health agency activities. These efforts can improve the ability of public health agencies to prepare for, respond to, and recover from any type of public health threat or incident. In addition, conducting demonstration projects to evaluate and test jurisdictional public health capacity will ensure that opportunities to strengthen public health infrastructure and systems are identified.
Public Health Implications
A national public health preparedness and response framework to support preparing for and responding to public health threats and emergencies did not exist prior to 2002. For more than 15 years, CDC has established and advanced preparedness standards for state, local, tribal, and territorial public health agencies. 11 Before the implementation of the PHEP cooperative agreement in 2002, state health departments lacked written plans, resources, and national guidance for building and sustaining public health surveillance systems, laboratory testing functions, and other capabilities.11,27
The capabilities standards were initially designed as a framework to advance jurisdictional public health agency planning, and they evolved as a framework to advance public health preparedness and response. Public health agencies now have updated national guidelines to prepare for and respond to the next international or domestic public health emergency as a result of the completion of the capabilities update initiative. Implementation of the updated capability standards at the state, local, tribal, and territorial levels may improve jurisdictional organizational capacity to respond to public health threats and emergencies and save lives. CDC plans to improve and update the capability standards on a regular basis, with feedback from stakeholders, experts, and national partners, as exemplified by the January 2019 amendment. Improving jurisdictional capacity to prepare for and respond to a variety of incidents and events improves community resilience and strengthens the health security of the United States.
Footnotes
Acknowledgments
The authors thank subject matter experts from CDC centers and program offices who participated in the capability development work groups, including from the Center for Preparedness and Response, Office of Infectious Diseases, Office of Noncommunicable Diseases, Injury and Environmental Health, Center for Global Health, National Institute for Occupational Safety and Health, Office of Public Health Scientific Services, Office of Minority Health and Health Equity, Office of Public Health Scientific Services, Office of Safety, Security, and Asset Management, Center for State, Tribal, Local, and Territorial Support, and Agency for Toxic Substances and Disease Registry. The authors also thank subject matter experts from HHS/ASPR and DHS/FEMA. The authors thank CDC's Division of State Local Readiness capabilities project team: LaBrina Jones, Susan Farrall, Andrea Harris, Kate Agin, and Kevin Sevak. The authors thank the policy and communication team: Germaine Vazquez, Linda Tierney, and CDC Creative Services for ![]() . We also thank the support by Deloitte affiliates: Erin McGrath Keys, Meredith Cord, Ariel Powell, Berthine Njiemoun, Amalia Flecksteiner, and Arthur Anglin. The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
. We also thank the support by Deloitte affiliates: Erin McGrath Keys, Meredith Cord, Ariel Powell, Berthine Njiemoun, Amalia Flecksteiner, and Arthur Anglin. The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.