
Abstract
The purpose of this study was to characterize changes in and impacts on epidemiologic capacity in local health departments after the implementation of a state-funded epidemiologist program using qualitative data. The study used key informant interviews in Texas health departments, which were conducted and inductively analyzed to identify themes. Five predominant themes emerged from interviews on the impact of state-funded epidemiologists on the epidemiology capacity of local health departments. State-funded epidemiologists were seen as increasing overall epidemiology capacity in local health departments. Specifically, they improved timeliness of infectious disease reporting and quality and thoroughness of disease investigations. They also improved community stakeholder relationships with local health departments and communications across local, regional, and state public health agencies. Key informants at all levels described positive effects of the state-funded epidemiologists on disease surveillance. Local epidemiology capacity has increased, and, in turn, Texas public health surveillance capacity has improved at the local, regional, and state levels. Funding programs like this should be considered when public health capacity is low and in need of an increase.
The purpose of this study was to characterize changes in and impacts on epidemiologic capacity in local health departments after the implementation of a state-funded epidemiologist program using qualitative data. Key informant interviews were conducted in Texas health departments to identify themes. Key informants at all levels described positive effects of the state-funded epidemiologists on disease surveillance.
Epidemiology is both a core public health function and an essential component of public health response. 1 Epidemiology capacity refers to the ability to provide comprehensive epidemiology services to support essential public health services in nonemergent situations on a routine basis. The Council of State and Territorial Epidemiologists (CSTE) has documented the epidemiology capacity of state health departments in the United States since 2001, using the Epidemiology Capacity Assessment (ECA) tool.2-4 The ECA is distributed to all state and territorial health departments and enumerates the number of epidemiologists by program area. Staff are further classified by education, experience, competency, salary, and job role. In 2017, a total of 3,370 epidemiologists were employed by state health departments, the highest number reported since CSTE began conducting the ECA. However, the ECA includes only state health department data, which do not represent the entire public health system.
Local health department epidemiology capacity is also important, since these agencies are typically at the forefront of providing essential public health services to the populations they serve. This is particularly true in states with a decentralized public health authority, meaning that local jurisdictions (ie, cities and counties) have the responsibility to provide public health services in their jurisdiction. However, the ECA does not routinely capture information on local health departments in the United States, which means that local health department epidemiology capacity data are limited.
In their 2013 ECA, CSTE identified gaps in epidemiology capacity at the state level and provided recommendations to address them. 2 One recommendation called for state health departments to increase funding from state budgets for epidemiologists, rather than relying disproportionately on federal funds.
In response to increasing caseloads of foodborne illnesses and high-consequence infectious disease investigations, the Texas Department of State Health Services (DSHS) started the state-funded epidemiologist program, which was designed to improve local epidemiologic capacity in local health departments throughout the state. 5 Texas has 254 counties, 71 local public health departments or districts, functionally 8 health service regions, and a state health department operating as part of a decentralized public health system. In its 83rd and 84th sessions (2013 and 2015), the Texas legislature funded 45 epidemiologist positions collectively for local health departments or districts in Texas to increase epidemiology capacity in the state in general, and specifically to improve response to infectious disease threats.
The Department of State Health Services provides the funds to local health departments through contracts, and local health departments hire and employ the state-funded epidemiologist position. State-funded epidemiologists work closely with DSHS officials, who provide statewide notifiable disease investigation guidance. Each local health department in Texas is different in organizational structure, size, and population served, as well as in the ways that epidemiology or disease surveillance programs operate. It is difficult to capture the unique experiences and challenges among local health departments using quantitative data because of their wide variability. Therefore, key informant interviews were used to provide detailed insight into the function, role, and impact of the state-funded epidemiologist program through applied qualitative methods.6-8
Methods
Theoretical Framework
A systematic review of public health capacity research indicated several existing frameworks that have been used to understand capacity, including the social-ecologic model; capacity assessment theory; appreciative inquiry; Lewin's Freeze-Thaw model; strengths, weaknesses, opportunities, and threats (SWOT) analysis model; and others. 9
A specific framework to understand public health capacity in emergency response was developed by Hu and colleagues, to better describe and evaluate programs and efforts in this area and to address some of the shortcomings of the previously mentioned frameworks in a public health emergency response setting. 7 In this framework, 3 levels are used to describe the program and provide an evaluation tool: a systems level, an entity or organization level, and the individual level. In this study, we structured our sampling of key informant interviews and questionnaire development around 2 existing approaches: Hu et al's capacity framework and the SWOT analysis model (see Supplemental Figure at https://www.liebertpub.com/doi/suppl/10.1089/hs.2019.0083).
Population
The state of Texas public health system is comprised of local, regional, and state-level public health services, including epidemiologic services. Key informant interviews were conducted with local health department leaders (eg, epidemiology supervisors, division managers) in health departments that had a state-funded epidemiologist position, as well as with regional and state epidemiology staff that have frequent contact with state-funded epidemiologist positions. For this qualitative study, representatives from each level made up the study population.
In Texas, 31 local jurisdictions received state-funded epidemiologists. To collect local data on the impact of adding a state-funded epidemiologist, key informant interviews were attempted with 1 representative from each of the 31 local health departments that received a state-funded epidemiologist position. The local health department representative was an epidemiologist manager/supervisor or health department director who oversees state-funded epidemiologist duties.
Each health service region has an epidemiology and surveillance department or unit that oversees infectious disease surveillance in the region and works closely with local health department epidemiologists. For the regional level, each of the 8 health service regions' lead epidemiologists who interact with local health department state-funded epidemiologists was invited for an interview. The DSHS state-funded epidemiologist program operates in the Emerging and Acute Infectious Disease Branch (EAIDB), which has 6 disease control teams—foodborne diseases, healthcare-associated infections, high-consequence infectious diseases, invasive and respiratory infectious diseases, surveillance infrastructure, and vaccine-preventable diseases—all of which may interact with the state-funded epidemiologists. Each disease control team lead was targeted for inclusion in this study to provide input from the central office perspective on state-funded epidemiologists in local health departments. The total sampling frame was comprised of 31 local health department epidemiologist managers/supervisors, 8 regional epidemiology or surveillance staff, and 6 staff from DSHS, for a total possible sample of 45.
Data Collection
Contact information for key informants at the local, regional, and state levels was obtained from the DSHS state-funded epidemiologist program coordinator or the DSHS website. Once all contact information was compiled, an email invitation requesting a 30-minute telephone interview was sent to each potential participant. When multiple supervisors or points of contact were listed, an interview was first attempted with the initial name listed online or in the database provided by the state-funded epidemiologist program coordinator. Subsequent contacts were made if the first potential participant was unable to complete the key informant interview. Each key informant was contacted via email up to 2 times to set up a mutually agreeable time for a telephone interview.
All interviews were recorded, with verbal consent, to ensure that accurate information was collected and reported. A semistructured questionnaire was used, which included the following components: strengths and weaknesses of state-funded epidemiologists, benefits to program areas, impact on disease surveillance, roles and responsibilities, and barriers to adding state-funded epidemiologists in local health departments or in different regions or the entire state.
Analysis
Audio recordings were transcribed using ATLAS.ti Version 8.0 (Berlin, Germany). Transcripts of the key informant interviews were then content analyzed for key themes using inductive coding, meaning that there were no predetermined themes but that themes emerged from the data through review and comparison. Themes were categorized to increase the reliability of coding, content was coded independently by 2 researchers, and themes identified were compared, reconciled, and compiled. 10 Reconciled themes and summary statements were copied into a Microsoft Word document for analysis. Themes were reported in categories based on the initial frameworks of different levels of the entire state-funded epidemiologist program and by strengths and weaknesses.
Results
Of the 45 key informants identified, 20 (44%) participated in a telephone interview: 42% (13 of 31) from local health departments, 50% from health service regions (4 of 8), and 50% from EAIDB (3 of 6) (Figure 1). Respondents reported a range of professional experience in public health or epidemiology, ranging from 18 months to 36 years (mean = 6.8 years; median = 4 years). Job titles of respondents included epidemiologist, lead epidemiologist, chief epidemiologist, surveillance coordinator, program coordinator, manager, and public health director. Local health department nonrespondents were similar to respondents across several categories, including department size, being in a rural or urban jurisdiction, receiving state-funded epidemiologists in the first or second phase of the program, and number of infectious disease case investigations. Five themes were identified from the inductive coding of the key informant interview transcripts:
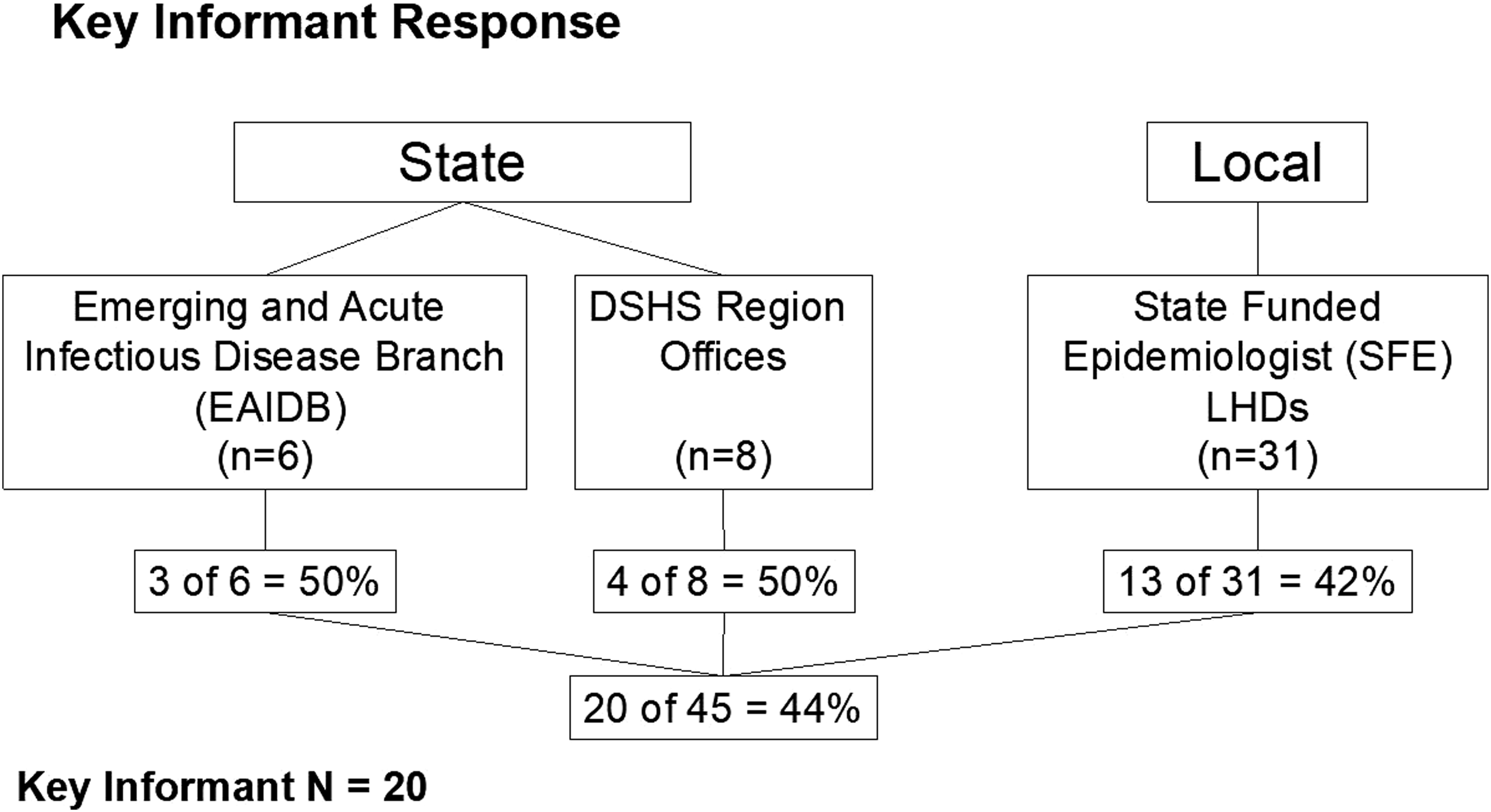
Key informant response from state and local participants
Increased overall epidemiologic capacity;
Timeliness in disease reporting;
Quality and thoroughness of disease investigation;
Reporting relationships; and
Communication across state.
Each theme is described in detail below with specific supporting quotes. A list of summarized weaknesses and recommendations for the state-funded epidemiologist program is also included.
Increased Overall Epidemiologic Capacity
All participants in local, regional, and state health departments described ways in which the state-funded epidemiologists have increased epidemiology capacity in local health departments in Texas. State-funded epidemiologists in local health departments do the bulk of infectious disease surveillance activities, from case investigation to data entry to outbreak response. Other staff, including existing local health department epidemiologists, are now able to expand the overall amount of epidemiologic work done by the local health department by reporting data and supporting analysis for other health department programs (eg, chronic disease, maternal and child health). For example, one local health department participant said,
“Having a dedicated person for infectious disease, it grows our overall epidemiology capacity with data reports and data analysis for other [local health department] programs.”
Another participant noted,
“The position has enabled other staff members to do more of their primary roles.”
Outbreak response capacity was also noted as being significantly improved by the addition of these positions. State-funded epidemiologists offer local health departments the resources to respond to outbreaks through fieldwork, such as conducting active surveillance and case finding.
Since most state-funded epidemiologists have at least master's-level training in epidemiology, the program has brought additional skills and expertise to local health departments. Several departments mentioned that state-funded epidemiologists have either started or assisted in starting new surveillance systems, such as for Zika virus infections. Data analysis and report writing were noted as strengths of the state-funded epidemiologist, and they also provide technical expertise by constructing outbreak detection systems and mapping disease in local jurisdictions using geographic information systems (GIS).
Timeliness in Disease Reporting
All participants in this study agreed that timeliness in disease reporting had improved with the addition of state-funded epidemiologists in local health departments. Local-level respondents articulated how having dedicated staff for disease surveillance had improved timeliness. Having required deliverables for the state-funded epidemiologists included in the contracts from DSHS was seen as contributing to improving timeliness in local health departments. For example, one of DSHS's deliverables was to complete a disease investigation and report to DSHS within 30 days. Prior to these contracts and the addition of the state-funded epidemiologist positions in local health departments, the 30-day requirement was not in place. One local health department manager said:
“The contract deliverables have helped us standardize our systems, so it's helped in that department; we are doing a good job meeting those deliverables. Without the contracts, we wouldn't have put as much focus on these.”
Regional and central staff indicated that disease reports come to the regional offices more quickly and that local health departments have better response times now with state-funded epidemiologists, especially in departments that had no epidemiologist prior to the state-funded epidemiologist position. One regional epidemiologist said:
“We've always had these timelines written into our guidance and trainings for [local health departments], but these contracts having them as a deliverable helps motivate the timeliness of getting the reports in. It is not just the deliverable; it is mainly because they now have a dedicated person to do it.”
Quality and Completeness of Disease Investigation
The quality and completeness of disease investigation in local health departments was improved according to most participants from each level of government. Health service region staff emphasized how disease investigations from local health departments have improved since the program was initially funded. One health service region participant stated:
“[State-funded epidemiologist] positions provide the ability and strength to keep up with changing case definitions and make time for follow up and confirmation of cases.”
All local health department participants agreed, describing how their public health surveillance and disease investigations were now of higher quality and more exhaustive. One department staff member mentioned that with the state-funded epidemiologist position:
“We are far more proactive, we have additional staff to do the work. We have more opportunity to do thorough surveillance.”
Reporting Relationships
By increasing local epidemiology and surveillance capacity, local health department staff noted the positive impact state-funded epidemiologists have had on building community relationships, especially with disease reporting entities such as healthcare providers. One health service region staff member said:
“The strengths of having local epidemiologists is making local relationships, a bigger impact in the small and medium health departments by building the relationships with reporting and surveillance and building capacity locally.”
Another way state-funded epidemiologists have improved reporting relationships with health providers locally is the dissemination of disease data reports. Providing stakeholders with outputs from their reports supports stronger relationships as providers see that the data they report are being used in a meaningful way. Local health departments also reported that state-funded epidemiologists were training and conducting outreach to reporting providers other than health care, like schools, daycare facilities, and long-term care facilities. Overall, state-funded epidemiologists are able to interact more closely with local stakeholders and healthcare providers, helping put a face on the local health department when reporting questions arise. One department staff member said:
“Our [state-funded epidemiologist] came in and started rubbing shoulders and really getting the health department outside of our walls and into the hospitals and community clinics; it has been great.”
Communication Across State
Participants from local, regional, and state public health agencies explained how having state-funded epidemiologists employed locally provides more points of contact for both the regional offices and DSHS. Because state-funded epidemiologists work closely with both health service regions and EAIDB, they provide quick access to what is going on locally with infectious disease–related work. They also increase the reach for health advisories issued by DSHS through the strength and breadth of their local relationships. For example, when DSHS issues a health advisory, state-funded epidemiologists can relay those messages to their local networks of providers. One regional staff member said:
“More providers are now reached with information and reporting. The network has increased in the region for health advisories.”
Difficulties, Weaknesses, and Recommendations for Improvement
Overall, nearly half (40%) of participants reported weaknesses or difficulties with the state-funded epidemiologist program. Of those who did report weaknesses, there were several themes. First, the state-funded epidemiologist program provides contract-based funding for positions in local health departments. This type of funding brings uncertainty to some of the departments about the program's stability and concern about whether or not the positions will continue to be funded. However, several local health departments that received a state-funded epidemiologist disagreed, stating that the contract funds are actually more secure and reliable than some of the local funds available for epidemiologists, making the state-funded positions more desirable locally.
Even with the state-funded epidemiologist program's contract funds, small and medium-sized local health departments may still struggle with the recruitment and retention of qualified epidemiologists. Each local health department has different compensation packages, and those that offer lower wages and benefits due to local administrative constraints have a difficult time recruiting qualified applicants for their departments. Once recruited, it can also be difficult to retain highly qualified individuals in these positions. One local health department explained that, due to their small size and rural location, newly minted epidemiologists they hire into their state-funded epidemiologist position do not stay with the department after 1 year; they move to less rural areas of the state once they have work experience as an epidemiologist.
The onboarding process of a new state-funded epidemiologist in small and medium-sized local health departments is time consuming and demanding on human resources for training and familiarizing these new staff with the department. The state-funded epidemiologists have epidemiology-specific training from a formal education, which provides them with foundational knowledge and skills, but they do not have the practical and working skills necessary to be a well-equipped and trained epidemiologist. This was only mentioned in the small and medium-sized local health departments, as large departments have the infrastructure and personnel to get new state-funded epidemiologists up to speed quickly.
In addition to these specific challenges, key informant interviews provided 4 recommendations for overall improvement of the state-funded epidemiologist program locally, regionally, and statewide. These were:
Keep current funding of program and add funding for more local and regional state-funded epidemiologists. Make workforce development a priority. Provide more applied training to state-funded epidemiologist workforce. Improve coordination and training between health service regions and the state-funded epidemiologists located in local jurisdictions in their regions. Consider restructuring current contract deliverables to more closely monitor the day-to-day work of state-funded epidemiologists to provide a more complete representation of their impact.
Discussion
Contract epidemiologist programs are not new, but they have traditionally been used at the local, state, and federal levels to address specific disease control efforts or newly emerging threats to public health. The Texas state-funded epidemiologist program is unique in that state funds were allocated to build local epidemiology and surveillance capacity for a broad spectrum of infectious diseases within a decentralized state public health system where local jurisdictions offer the majority of essential public health functions.
Local health departments struggle due to inadequate organizational capacity and financial resources to offer all 10 essential public health services (EPHS) effectively. 11 Four of the 10 EPHS (1, 2, 9, and 10) are linked to epidemiology capacity. EPHS 1 relates to the monitoring of health status to identify and solve community health problems. EPHS 2 includes diagnoses and investigations of health problems and health hazards. EPHS 9 evaluates effectiveness, accessibility, and quality of personal and population-based health services. EPHS 10 focuses on using research to find innovative solutions to health problems. Since epidemiology capacity is linked to 4 of the 10 EPHS, an emphasis on building this capacity is reasonable, and based on the qualitative findings in this study, the Texas SFE program has had an impact on each of these areas.
The advantages of the state-funded epidemiologist program to local health departments were described by participants in this study from each level of government—local, regional, and state. One recommendation from key informants at all levels is to keep funding the program and, if possible, increase funding for additional positions locally and new positions regionally. In a 2017 report on local health departments across the United States, the National Association of County and City Health Officials (NACCHO) found that local health departments have eliminated 55,590 jobs since 2008. 12 In the NACCHO report, medium-sized local health departments were more likely to experience job losses in the coming year, while large local health departments were least likely to have such losses. Our key informant interviews supported these findings, stating that without the state-funded epidemiologist program, the work that these positions do would simply not be done because of the lack of resources and capacity locally.
Another possible reason behind respondents' unanimous recommendation to keep funding the program is that it is estimated that one-third of all local health departments anticipate budget cuts from local sources in the upcoming year. 12 These results and data are from one largely decentralized state in the United States, but 26 other state health departments have a decentralized structure and so could have similar outcomes from such a program aimed at increasing epidemiology capacity locally. 13
In this study, one difficulty consistently identified by small and medium-sized local health departments was the recruitment of qualified epidemiologists. This is especially true in rural jurisdictions. 12 Contributing factors include a lack of competitive pay, location, and size of the local health department. Large departments allow epidemiologists to specialize if they desire and work with large, highly trained teams, and they provide infrastructure for career advancement. Local health department participants mentioned that pay was a barrier but only part of the challenge of finding qualified applicants in general. According to NACCHO, over 50% of all local health departments have difficulty in hiring specialized positions because of insufficiencies in the candidates or not having qualified applicants. 12 One respondent pointed out that local residents and existing local health department staff who applied for the state-funded epidemiologist position were not eligible because they lacked the recommended academic qualifications.
Respondents at all levels pointed to turnover as a challenge to staffing the state-funded epidemiologist positions in local health departments. Large departments had less turnover compared to small to medium-sized local health departments, and turnover was especially prevalent in departments where the state-funded epidemiologist was the only epidemiologist on staff.
It is widely recognized that recruitment and retention of healthcare workers is more difficult in rural settings compared to urban areas. 14 According to a 2013 CSTE report, state health department epidemiologists with at least a master's degree had an 11% turnover rate per year, while in a 2017 CSTE report, retention was listed as a major epidemiologic capacity concern.2,4 Although we do not have an estimate for the current turnover rate per year in epidemiologists, a 2017 public health workforce study reported that up to 25% of public health workers plan to leave their jobs in the next year, an increase of 41% from the last workforce study in 2014. 15 The qualitative findings of from this study agree with the results of the workforce study, highlighted by respondents reporting retention issues. Retention can affect public health response and preparedness as well. Vacancies and new staff that are not fully trained and have little experience strain local health departments' overall epidemiology capacity, in turn affecting response capacity. Despite turnover in the state-funded epidemiologist positions, it was noted that local health departments have adapted and put systems in place to keep surveillance activities going during staff transitions by cross training other staff and developing procedures for training and bringing in new state-funded epidemiologists.
Jurisdictions can use these findings to streamline and remove modifiable barriers mentioned by respondents in this study if they are looking to increase their epidemiology capacity through adding positions. Small and medium-sized jurisdictions, especially those in rural settings, should consider streamlining the time it takes to get new positions operational. One way to ease the burden of practical field training is to partner with larger jurisdictions who have expertise and the infrastructure to help train and share resources.
This may look different from state to state and jurisdiction to jurisdiction, but the principle remains: Public health is system wide, and disease outbreaks do not follow jurisdictional boundaries. Therefore, partnering to improve surrounding capacity helps the entire public health system's capacity. One way to counter epidemiologist turnover and keep capacity is to partner with CSTE or similar epidemiology organizations that offer continuous competency-based training with the goal of keeping the epidemiologic workforce equipped. Respondents in this study recommended providing greater workforce training. Examples included data and spatial analysis, database management and programming, and online survey development.
This study has several limitations. The information collected from key informant interviews represents only the qualitative impressions of a sample of participants in the state-funded epidemiologist program and may not represent the thoughts and experiences of all who are associated with the program or the public health system it affects. In an effort to mitigate this, we invited informants who represented a range of experience and public health roles to ensure that the qualitative information can still be of value to a broader audience of public health managers and decision makers. Twenty of 45 key informant interviews were attempted with local health department representatives who manage the state-funded epidemiologist contracts with DSHS, presenting the potential for response bias. To address this, participants from health service regions and EAIDB were also included and completed the same semistructured questionnaire.
In this study, the themes identified in local health department interviews were consistently included in regional and state-level responses, providing a confirmation of the perceptions of local health department staff. Another potential limitation is the difference between respondents and nonrespondents. Although local health department respondents were similar in terms of department size, being in a rural or urban jurisdiction, first or second phase state-funded epidemiologists, and number of case investigations, respondents and nonrespondents from the regional and state levels differed. Regions and state program areas that had higher total population served and volume of case investigations participated in the study, presenting potential bias in their responses. Only local health departments that received a state-funded epidemiologist were included in this study, leaving the impressions and information from local health departments without a state-funded epidemiologist out of this study. Local health departments in the state-funded epidemiologist program were sampled to best understand each department's experience with its state-funded epidemiologist, which is why local health departments without a state-funded epidemiologist were not approached. The semistructured questionnaire based on Hu et al's capacity framework 7 and the SWOT analysis model 8 may have not captured all qualitative data relevant to this specific project.
To our knowledge, this is the first qualitative study to examine the impact of a contract epidemiology program in local health departments. These interviews provide the type of indepth information typically not found in a structured questionnaire, and similar types of interview data have been used to identify potential shortfalls in health delivery or modifiable procedures along with program strengths and benefits.6,16,17 These interviews also fill a gap in the existing assessments of public health and epidemiologic capacity in the United States, which do not collect data at the local level, and findings are consistent with state epidemiologist workforce assessments conducted by CSTE.
Other state public health systems can look to this program as a model for improving epidemiology capacity through funding epidemiologist positions and locating them throughout their state's system, depending on their structure (centralized vs decentralized). These findings highlight the difficulties small and medium-sized local health departments have in keeping epidemiology capacity and report suggestions from local, regional, and state respondents. Overall, findings from this qualitative assessment indicate consistent agreement with the hypothesis that local health departments have improved epidemiology capacity through a contracted epidemiologist program in Texas.
Footnotes
Acknowledgments
The authors acknowledge Eric Garza with the Texas Department of State Health Services for his technical support and subject matter expertise during data collection of this project. All materials were reviewed by the Texas A&M University Institutional Review Board (IRB#17-0366M) and determined to be exempt. The authors of this article have no competing interests to disclose. This project had no funding source.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.