
Abstract
In August 2014, the World Health Organization declared the Ebola virus disease epidemic in West Africa a public health emergency of international concern. After 2 imported cases of the disease were identified in the United States in autumn 2014, the Centers for Disease Control and Prevention recommended that all jurisdictions begin active monitoring of travelers at risk of developing Ebola virus disease for 21 days from the last day of a potential exposure to minimize the risk of disease transmission. Here we describe the infrastructure development, monitoring processes, total planned expenditures, and effects on the public health system in Georgia associated with active monitoring and illness response of all travelers from Ebola-affected West African countries from October 2014 to March 2016. We conducted qualitative interviews with Georgia Department of Public Health (GDPH) staff. We identified state active monitoring and illness response infrastructure investments and monitoring activities and state and federal funds spent in both areas. And, we evaluated whether active monitoring and illness response enhanced Georgia's ability to respond to future infectious disease outbreaks. Developing the infrastructure to support the monitoring and response required investment in information technology, training of public health and medical personnel, increasing laboratory capacity, and securing personal protective equipment. Estimated total expenditures were $8.25 million, with 76% spent on infrastructure and 17% on daily monitoring. The GDPH leveraged internal resources and partnerships to implement active monitoring and illness response. Infrastructure investment increased surveillance capacity, strengthened relationships between the GDPH and medical providers, and led to the creation of infectious disease transport and hospital networks. Active monitoring and illness response increased outbreak preparedness, but it warrants comparison with other possible responses to determine its overall value.
In august 2014, the World Health Organization declared the Ebola virus disease (EVD) epidemic in West Africa a public health emergency of international concern. 1 After 2 imported cases of EVD were identified in the United States in autumn 2014,2,3 the Centers for Disease Control and Prevention (CDC) recommended that all states and territories begin active monitoring of travelers at risk of developing EVD until 21 days from the last day of a potential exposure. 4 The goal was to minimize the risk of transmission in the United States. 5
While departments of public health are well versed in conducting communicable disease surveillance, active monitoring of and illness response to EVD presented a new, complex scope of work, which was particularly challenging given the uncertainty around the risk of EVD transmission and the number of potential exposures.6,7 Active monitoring and illness response protocols required public health departments to have daily contact with travelers from West Africa for up to 21 days and to maintain records of their temperatures, the presence or absence of other possible EVD symptoms, and any changes in jurisdiction.
States aimed to implement active monitoring and illness response protocols within 1 week of the CDC recommendation that required them to establish an infrastructure—physical and organizational structures and facilities—to support daily monitoring, along with traveler contact processes. 8 All states complied with CDC recommendations, but each state had discretion in how to implement active monitoring and illness response in the existing public health system. Most needed to build or expand on information technology (IT) systems to store longitudinal traveler data, establish quarantine facilities to house high-risk travelers, and train personnel in EVD management. Infrastructure to support daily contact was critical, because if contact could not be maintained over the 21-day period, active monitoring and illness response would be an ineffective way to reduce the risk of disease transmission.
The US Department of Homeland Security designated 5 international airports—in Atlanta, Chicago, Newark, New York City, and Washington, DC—to process these travelers. 9 The US Customs and Border Protection, in collaboration with the CDC, conducted an initial assessment of symptoms and exposure risk for all travelers and referred those with elevated risks to CDC personnel, who conducted an in-depth public health assessment. Travelers with symptoms consistent with EVD were referred to state-designated hospitals for further evaluation. The rest were referred to state departments of public health for monitoring.6,10,11
Traveler information was transmitted to public health departments through the CDC Epidemic Information Exchange (Epi-X), a secure web-based network established in 2000 for communications among CDC and public health officials. 12 The CDC also implemented the Check and Report Ebola (CARE+) program, in which trained social workers explained active monitoring and provided CARE kits, which included information on requirements to report symptoms to the state department of public health and a prepaid mobile phone. 11
Initially, states funded their EVD response activities internally. In December 2014, the US Department of Health and Human Services, through the CDC Division of State and Local Readiness, made approximately $4.7 million available to states that were receiving Public Health Emergency Preparedness (PHEP) funds and provided an additional $145 million in 2015 to support EVD preparedness activities. 13 The CDC Division of Preparedness and Emerging Infections also released $110 million through the Epidemiology and Laboratory Capacity (ELC) program, a small portion of which was used to fund active monitoring and illness response infrastructure.14,15 The Georgia Department of Public Health (GDPH) applied for funds from both of these sources.
To date, the literature on the costs of implementing active monitoring and illness response is limited. Several papers have described daily monitoring activities undertaken by states and monitoring outcomes, including Georgia.6,7,16-19 However, none have examined the total costs of active monitoring and illness response, including infrastructure investments, or the long-term public health system effects.20-23
This article describes the implementation of active monitoring and illness response, including infrastructure investments, its costs, and its effect on the public health system in Georgia. We focused on Georgia because Hartsfield-Jackson Atlanta International Airport was one of the airports designated for routing of travelers from West Africa. In addition, Emory University Hospital in Atlanta has a biocontainment unit capable of managing Ebola-infected individuals, and personnel from GDPH were willing to participate.
Methods
We collected data from October 2014 through March 2016 to describe active monitoring and illness response implementation, estimate associated costs, and identify any lasting effect on the public health system in Georgia. Beneficial effects were defined as physical infrastructure investments and changes in organizational relationships that would increase Georgia's ability to respond to future infectious disease outbreaks.8,24 We used a mixed-methods approach and relied on 2 primary data sources: qualitative interviews with GDPH staff and their partners and budgets from federal cooperative agreements awarded to Georgia.
After reviewing public health evaluation tools, we developed an interview script (see Appendix 1, Supplemental Material at https://www.liebertpub.com/doi/suppl/10.1089/hs.2019.0127) for qualitative data collection from GDPH with input from other CDC staff.25-31 Script topics included infrastructure development, monitoring processes, state spending on active monitoring and illness response, system modifications over time, outcomes, and implementation challenges. We then interviewed staff from the 3 units in the GDPH Health Protection Division, the Public Health Preparedness Program, the Hospital Preparedness Program and Office of Emergency Services, and the Georgia Poison Control Center, which assisted with daily monitoring.
Based on these interviews, we outlined possible traveler movements post-arrival that determined the infrastructure and partnerships needed to maintain 21-day contact with them. We then identified specific infrastructure investments undertaken to support monitoring and the components of daily monitoring itself. We then estimated the total costs of implementation. We identified expenses borne by GDPH based on staff reports and those supported by federal funds based on the line item budget descriptions of what was funded through the ELC and PHEP awards. From the CDC awards, we included only items directly supporting active monitoring and illness response (Appendix 2 provides sample allocations; see Supplemental Material at https://www.liebertpub.com/doi/suppl/10.1089/hs.2019.0127).
We classified spending as related to either active monitoring and illness response infrastructure or to daily monitoring. Within each category, we grouped spending by functional area: epidemiology and surveillance, emergency medical services, hospital preparedness, and laboratory services, then further disaggregated spending into personnel, IT, travel, supplies and equipment, training, and other costs. 32 We summed all items to calculate total costs. Staff interviews indicated that GDPH provided personnel for the monitoring period and handled quarantine arrangements for travelers with high-risk exposures. We identified 4 key GDPH staff from the Health Protection Division and 1 from the commissioner's office as central to implementation of active monitoring and illness response. We estimated the opportunity costs of staff time based on percentage of time spent on active monitoring and illness response multiplied by annual salaries. Wage values were drawn from publicly available state of Georgia salary schedules for epidemiologists and public health managers.
We assumed effort percentages of 100% for months 1 through 4, 60% for months 5 through 9, and 20% for months 10 through 18.33,34 We assumed effort percentages for the GDPH deputy commissioner general of 80%, 20%, and 10% for those periods. Effort percentages were graduated to reflect the hiring of additional staff to manage responsibilities entailed in active monitoring and illness response. We assumed that 2 GDPH staff and the deputy commissioner worked on active monitoring and illness response infrastructure and 2 staff worked on both infrastructure development and daily monitoring.
GDPH had to secure quarantines facilities and rented 2 houses to serve as quarantine sites. It paid substantial rental surcharges, bought appliances and furniture, and made special arrangements to collect trash and clean. Quarantine costs were estimated at 4 times the median house rental cost in the local area. 35 We conducted several sensitivity analyses related to costs. Given our assumptions about GDPH staff time spent on active monitoring and illness response, we varied GDPH staff base salaries and percent effort by ±20%. We also varied quarantine housing costs by ±50%, and we reduced infrastructure costs by 20%, given that most were based on our allocation of line-item descriptions from federal budgets.
We also collected data on the number of travelers monitored, referred for medical evaluation, transported, quarantined, and lost to follow-up. We then calculated the total and daily monitoring cost per traveler monitored. Based on interview responses and the definitions of short- and long-term infrastructure investments in the literature, 8 we identified long-term contributions to Georgia's emergency preparedness and challenges to implementing active monitoring and illness response.13,36,37
Results
GDPH Active Monitoring System
Figure 1 provides a flow diagram of possible traveler movements on arrival. Many infrastructure investments were required to ensure continuous traveler monitoring and minimize loss to follow-up, defined as having a gap in reporting of more than 48 hours.
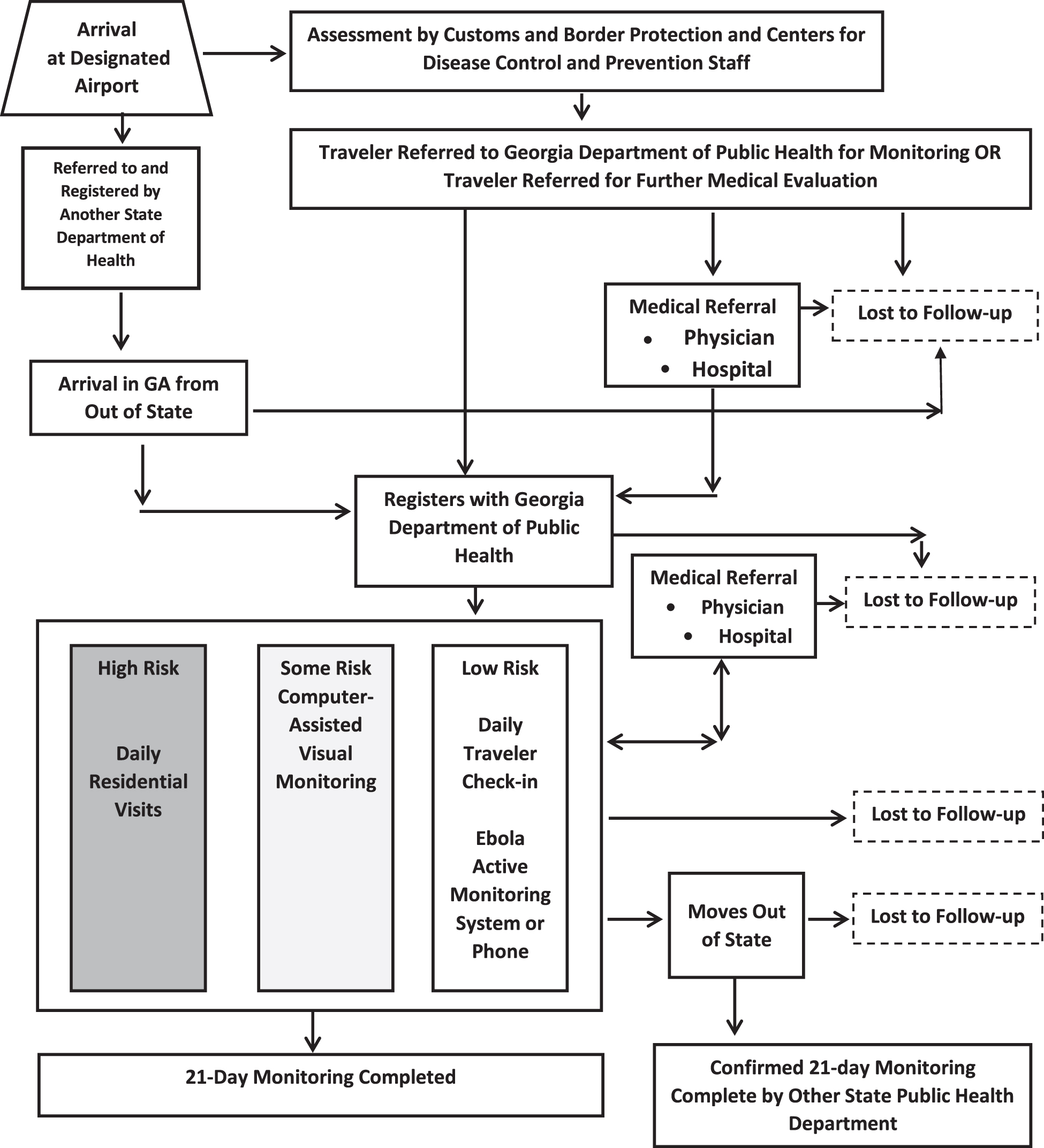
Schema for active monitoring and illness response in Georgia during the 2014-2016 Ebola epidemic, based on possible flow of travelers.
As the diagram shows, travelers initially referred by the CDC for immediate medical care could contact the GDPH on discharge or be lost to follow-up. Those directly referred to the GDPH could be lost to follow-up before establishing contact. Once registered, the GDPH classified travelers into 1 of 3 risk categories based on CDC recommendations: low, some, and high. 10 Low-risk travelers were those who had been in a country with widespread EVD transmission and were thought to have a greater than zero risk of exposure to Ebola virus; they were required to report daily.
Travelers at some risk were those who had been directly exposed to a person with symptomatic EVD while wearing appropriate personal protective equipment (PPE) or who had been within 3 feet of a person with EVD without wearing PPE. High-risk travelers were those with direct exposure to EVD virus. The GDPH monitored both groups daily for manifestations of symptoms, using computer-assisted video monitoring for travelers with some risk; high-risk travelers were quarantined and received in-person visits.10,11
Once in contact with the GDPH, a traveler in any risk group could be referred for medical evaluations, at which point the risk of being lost to follow-up arose again. Low-risk individuals could be lost to follow-up during the 21-day monitoring period. Local health departments were available to help locate those who failed to report their daily temperatures and symptoms. Being lost to follow-up was also possible if travelers left the state and did not report to another health department. Also, at-risk travelers could enter the state and not register with the GDPH.
Infrastructure Development, Daily Monitoring Processes
The GDPH Health Protection Division, Epidemiology Section, led the implementation of active monitoring and illness response. It set up 2 systems for daily monitoring of low-risk travelers. The first was a dedicated call-in line. The GDPH partnered with the Georgia Poison Control Center to handle calls from travelers who preferred to report by phone. Center staff recorded information and transmitted it to the GDPH, normally by email, for entry by GDPH personnel into the internet-based Ebola Active Monitoring System (EAMS). If a caller was symptomatic, Center staff immediately alerted the GDPH medical epidemiologist on call.
The GDPH Epidemiology Section set up the internet-based system data collection system, EAMS, as a separate module within the homegrown State Electronic Notifiable Disease Surveillance System (SendSS) used for disease surveillance. EAMS provided the capacity to register and track individuals over time. It included interactive capabilities whereby travelers could log in and update their records and receive a daily email reminder to record their symptoms. 7
GDPH staff, with the support of personnel hired through supplemental funds, established other parts of the active monitoring and illness response infrastructure. For example, they developed monitoring protocols, acquired video-based monitoring and PPE, and set up quarantine locations. They trained personnel from hospitals, emergency medical services (EMS), local public health departments, and the Georgia Public Health Laboratory on EVD, infection control, use of PPE, protocols for active monitoring and illness response, and EAMS. They also supported coordination efforts among these organizations.
GDPH staff also conducted daily monitoring, including video for travelers with some risk or face-to-face contact with high-risk travelers. Staff also collaborated closely with the CDC regarding monitoring Georgia-based CDC employees returning from West Africa.
EMS and Hospital Preparedness
The GDPH's Office of Emergency Medical Services established a system capable of transporting symptomatic individuals with potential exposure to EVD safely to medical facilities, while the Hospital Preparedness Program (HPP) worked to ensure hospitals were prepared to admit them. The programs, in concert, created 2 interactive networks to manage travelers and others at risk of EVD infection: (1) an infectious disease hospital network and (2) an infectious disease transport network. 37
At the initiation of active monitoring and illness response, the Office of EMS and the HPP held an infectious disease summit to bring partners together for a coordinated response. The networks followed the model established for handling patients with myocardial infarctions (MI), the ST-elevation myocardial infarction (STEMI) system, whereby EMS triages patients suspected of having an MI to STEMI-certified hospitals, where specific treatments protocols are in place.
The Office of EMS focused on building the Infectious Disease Transport Network (IDTN), and it developed transport protocols and trained medics in infection control procedures, the appropriate use of PPE, and traveler privacy and safety. The Office of EMS also trained state 911 operators to identify suspect cases. Private providers, such as taxi services, were not part of the IDTN.
Simultaneously, the HPP identified hospitals that were willing to receive patients at risk for EVD to establish the Infectious Disease Hospital Network (IDHN). The GDPH provided training on EVD infection control and the use of PPE, while HPP developed internal protocols for accepting patients from EMS and the management of at-risk patients once they were admitted. Twelve hospitals became part of the network, with 8 designated for assessment and 4 designated as treatment hospitals. 37
A GDPH medical epidemiologist served as the EMS provider incident commander. Once an at-risk patient was identified, network EMS providers called the GDPH, which then contacted IDHN hospitals to determine which facility could accept the patient. Incident command then coordinated with EMS providers for immediate transport.
Expenditures and Outcomes
Table 1 provides information on the total costs of implementation of active monitoring and illness response. In total, an estimated $8.25 million was spent on active monitoring and illness response, with infrastructure costs constituting 76.1% ($6.28 million), daily monitoring costs 16.9% ($1.40 million), and overhead 7.0% ($570,000).
Active Monitoring and Illness Response Expenditures by Category, Functional Area, and Spending Type a
All costs in US 2016 dollars.
District health planners, medical epidemiologists for infection control oversight, hospital certification oversight, Ebola outbreak response planning and training across the state; infection control nurse to certify hospitals and EMS providers; and epidemiologists (25%) to provide oversight for linking hospital targeted action plans for Ebola; and SendSS for reporting and feedback.
Most of the indirect costs were embedded in the contractual agreements and not disaggregated.
Overall, personnel was the largest expense, constituting 54.4% of the total costs, while 11.4% was spent on supplies and equipment; similar levels were spent on housing (8.4%), IT (8.1%), and communications (8.0%). The GDPH spent $620,533 on staff who were redirected from ongoing notifiable disease surveillance activities, HIV/AIDS, influenza, and measles, and $689,784 on quarantine housing, thus adding up to 15.9% of total costs for active monitoring and illness response. Most indirect expenses were embedded in contractual expenditures, while $577,256 was listed separately as the balance of indirect costs, or 7.5% of the total. In terms of infrastructure costs, personnel expenditures constituted 49.8% of spending, with 77.8% of this amount dedicated to epidemiology and surveillance staff. This included a district health planner, medical epidemiologists for EVD infection control oversight and EVD outbreak response planning and training across the state, and infection control nurses to certify hospitals and EMS providers in EVD management.
Supplies and equipment constituted nearly 14.7% of expenditures, with 57.4% of the supply monies going to labs for disinfection units and diagnostic reagents related to EVD testing. Lab costs borne by the GDPH totaled $876,711 and related to reagent supplies and training of personnel in safe handling of sample and testing techniques. IT investment, primarily dedicated to building and maintaining EAMS and securing housing for quarantine, made up 10.7% each, while training constituted 10.0%. Daily monitoring costs were approximately $1.4 million, with 97% of funds supporting personnel.
Sensitivity Analyses
We conducted sensitivity analyses on GDPH staffing costs, quarantine costs, and infrastructure costs (Table 2). Reducing GDPH staff salaries and percent effort by 20% lowered total costs by $223,392, and, when those costs were increased 20%, costs rose by $489,726. Varying quarantine costs by ±50% changed total costs by $138,000. Reducing fixed costs by 15% decreased total costs by $1,255,297. Adjusting for all cost reductions and increases simultaneously produced a total cost range of $6,634,365 to $8,878,780.
Sensitivity Analyses of Georgia Department of Public Health Personnel, Quarantine, and Infrastructure Costs on the Total Cost of Active Monitoring and Illness Response
Outcomes of Daily Monitoring
As shown in Table 3, Georgia monitored 2,257 travelers. Of those, 113, all of whom were low risk, were permanently lost to follow-up. Of travelers completing monitoring, 98.5% were designated low risk, while 1.5% were identified as having some risk or high risk. CDC employees constituted more than half of those monitored, all of whom were at low risk. Of travelers completing monitoring, 60% used EAMS; the remainder called in for daily check-ins. Forty travelers were referred for medical evaluation; 72.5% were evaluated for EVD, and none was positive. Most symptomatic travelers used private transport, not the IDTN, to get to medical facilities. No traveler referred for medical evaluation was lost to follow-up. Overall, Georgia's cost per traveler monitored was approximately $3,656, with direct monitoring costs of $619 per traveler.
Outcomes of West African Travelers Monitored in Georgia during the 2014-2016 Ebola Epidemic
Non-Ebola virus disease, discharge diagnoses were: gastrointestinal illness (9), influenza (9), respiratory infections (10), malaria (4), other infections (5), pregnancy complications (2), and diabetic complication (1).
Long-Term Effects and Challenges
GDPH staff identified numerous challenges related to implementation of active monitoring and illness response. First, active monitoring and illness response was outside the department's historical scope of work, and the CDC provided little guidance on how it should be conducted. Second, federal monies to support active monitoring and illness response were not immediately available. States and their partners thus faced considerable uncertainty about financial liabilities for active monitoring and illness response, along with the duration and scope of the program.
Hiring qualified staff on short notice was difficult, particularly given that the GDPH had to compete with the CDC, headquartered in Georgia. Maintaining trained staff throughout the system established for active monitoring and illness response over time proved to be difficult for the GDPH to remain a competitive employer.
Data transfer was not seamless. Initial traveler referrals from Customs and Border Protection and the CDC contained misspelled names and incorrect telephone numbers. Call centers could not enter data into EAMS, so information was passed by fax. Some travelers did not speak English, and GDPH staff and partners did not speak a language they knew.
While states communicated through Epi-X about travelers known to be changing jurisdictions, maintaining contact with travelers crossing state lines was problematic. It is unknown if travelers from other states entering Georgia registered with the GDPH. It is also unclear whether travelers leaving the GDPH registered with the department of public health in their destination jurisdictions.
Finally, securing quarantine facilities for high-risk individuals proved extremely challenging, because landlords were reluctant to rent properties to individuals exposed to any degree to EVD.
Discussion
This evaluation describes active monitoring and illness response as implemented in Georgia, along with the costs, outcomes, and public health system benefits. The estimated total cost of active monitoring and illness response was $8.25 million, ranging $6.63 to $8.89 million, with two-thirds spent on infrastructure. Overall, personnel constituted 54% of the total cost. Significant personnel time was required to establish monitoring infrastructure, while 98.5% of monitoring expenses were for personnel. The GDPH bore 15.9% of the costs of active monitoring and illness response, split between quarantine costs (52.6%) and redirected staff time (47.4%). Federal cooperative agreements funded the remainder.
We view the GDPH's program as successful in that 95% of at-risk travelers completed 21-day monitoring. No individuals at some risk or high risk in Georgia were lost to follow-up. Maintaining contact also likely avoided unnecessary hospital visits, as concern over symptoms could be discussed with the health department.
Georgia's ability to maintain contact with travelers was similar to that of New York City, where 5% of travelers were lost to follow-up. 38 Nationwide, only 1% of travelers were lost to follow-up, but that figure likely reflects the fact that most states had far fewer travelers to monitor than Georgia and likely higher staff-to-travelers-monitored ratios. CDC also provided loaded mobile phones to all arriving travelers to facilitate contact with the public health department.
Georgia had a relatively high volume of travelers, as Hartsfield International was a destination airport. By December 2015, a total of 29,789 travelers had been monitored through the US entry Ebola-screening program. Of this total, 53% were monitored in 5 jurisdictions: Georgia, Maryland, New York, Pennsylvania, and Virginia. Georgia monitored 14% of travelers arriving through the 5 major jurisdictions. All 50 states plus the District of Columbia, New York City (NYC), Puerto Rico, and the US Virgin Islands monitored people, all at low risk, while 44 states, the District of Columbia, New York City, and Puerto Rico monitored 1 or more individuals at some risk or high risk. Three territories and 3 freely associated states had no people being monitored. 6
Some metrics are available on which to compare Georgia to other states. 17 For example, like two-thirds of states, the GDPH operated a centralized system, as opposed to monitoring responsibilities being passed on to local agencies. Similar to 86% of states, Georgia built on established surveillance systems and used high-tech surveillance, such as video monitoring, as did 22% of other states.
New York City estimated the costs of daily monitoring alone to be approximately $1.9 million, compared to Georgia's $1.4 million. However, NYC's number is not comparable to Georgia's as it appears to represent the cost of contracted labor only. 39 An in-depth comparison of state models of active monitoring and illness response is beyond the scope of this article, but it is an important area for further research.
The state's response and investment choices increased Georgia's ability to respond to future infectious disease outbreaks. The GDPH now has an IT system capable of recording longitudinal data on individuals, which hospitals can access. It has protocols in place for conducting continuous individual monitoring of complex populations, EVD lab testing, and use of PPE, and a required EMS certification, built on GDPH's initial training, on the transport of people with possible infectious diseases. Interactive hospital and transport networks are functional, and new public health partnerships have been forged, particularly with medical providers.
While active monitoring and illness response led to system enhancements, concern exists regarding the ability to sustain these benefits. Future funds will likely be needed to support ongoing training to ensure trained personnel remain in place throughout the public health system. Equipment and lab supplies used during the outbreak also need to be replaced and/or maintained. EMS needs additional investment to expand transport capacity, as the majority of travelers transported themselves to medical facilities. Also, securing stand-by quarantine facilities that can be used in the case of a future infectious disease outbreak is critical. Communication systems between states should be improved.
These findings are subject to qualifications. Our estimates indicate the magnitude of expenditure rather than precise figures. GDPH expenditure information, derived from qualitative surveys with GDPH personnel, is subject to recall bias of unknown effect. We aimed for a conservative estimate of these costs and did not include costs of administrative or IT support, the GDPH commissioner's time, time costs for partners who participated in training, or any costs borne by travelers being monitored, particularly during quarantine.
We did not include any funds directly supplied to hospitals or laboratories, such as those provided through the Assistant Secretary for Preparedness and Response as part of the larger Ebola control effort.
Estimates of expenses of active monitoring and illness response, supported by federal dollars, were calculated from funded budget requests, formulated at the beginning of the outbreak. The GDPH was awarded $8.67 million from the CDC through cooperative agreements, of which 80% was spent on active monitoring and illness response.13,14 Federal monies were primarily spent on active monitoring and illness response infrastructure.
We identified federal infrastructure investments through line-item budget reviews and included only those costs associated with establishing the active monitoring and illness response network to support daily contact with travelers. For example, we excluded costs to conduct readiness exercises for network partners in Georgia's 14 hospital jurisdictions, as these were viewed as not directly related to active monitoring and illness response. If activities beyond the scope of active monitoring and illness response were included in our estimates, these would bias our results upward.
The state indicated that most awarded funds were spent; a small portion was allocated as continuing support for district health planners through a no-cost extension after active monitoring and illness response had ceased. Given that these funds were used to sustain/solidify active monitoring and illness response infrastructure investment, planned expenditures are likely a good estimate of actual spending. (In no way should this article be viewed as an audit of Georgia's spending.)
We argue that the GDPH minimized costs by leveraging existing relationships and building on the existing SendSS data platform. We do not know to what degree costs would have varied if the number of travelers was substantially larger. It is also possible that active monitoring and illness response could have operated more efficiently. Our results are unlikely to be generalizable, as each state had discretion in how to implement active monitoring and illness response.17,40
However, our case study provides a model for subsequent evaluations of other states. It also highlights issues likely to have affected other states, such as the significant investment in infrastructure required to support active monitoring and illness response, heretofore unreported, the costs imposed by the active monitoring and illness response approach on states, the need for improved coordination with CDC, and the difficulties of interstate movements.
Totals also reflect Georgia's indirect cost rate, 17.6% (PHEP) and 19.7% (ELC), which may be higher or lower than in other states. Emory University hospital is located in Georgia, and as a result the state received high-risk travelers from out of state who were quarantined. Further, CDC headquarters' location in Georgia influenced daily monitoring of most of the travelers arriving in Georgia, who were CDC personnel who participated in EVD control efforts in West Africa.
Active monitoring and illness response was an extreme response to a possible infectious disease outbreak, particularly one where the risk of transmission proved to be very low and screening of travelers occurred at several points prior to entry into the United States. While Georgia attempted to minimize costs through leveraging existing systems and relationships and accrued public health system benefits, we cannot comment on the value of active monitoring and illness response. Given that no cases of EVD occurred, we also cannot determine to what degree active monitoring and illness response would have affected the risk of transmission.
Alternative responses to the EVD outbreak, such as self-quarantine or a focus on high-risk travelers, were possible, and cost-effectiveness analyses comparing them to active monitoring and illness response would be needed to establish the cost-effective of active monitoring and illness response. Conducting a cost-benefit analysis that quantifies benefits in dollar terms would be necessary to provide information on a dollar-based cost/benefit ratio. However, it must include the costs borne by the states. Given that future infectious disease outbreaks are highly likely to occur, these are important areas for future research.
Implications for Policymakers
In October 2014, the CDC recommended 21-day active monitoring of travelers from West Africa at risk of EVD exposure, to minimize the risk of disease transmission in the United States.
The GDPH implemented active monitoring and illness response over an 18-month period at an estimated cost of $8.25 million for 2,257 travelers, most of whom had minimal exposure. The cost per traveler monitored was $3,656. The GDPH bore 16% of total costs.
Ensuring continuous contact with travelers required cooperation with Georgia's Poison Control Center, the Georgia Public Health laboratory, EMS and medical personnel, and hospitals.
The vast majority of spending, 76%, was on public health infrastructure to support continuous daily monitoring. Investments included building dedicated IT systems, creating extensive training and response protocols, and establishing EMS and hospital transport networks for people at risk of highly infectious diseases.
Active monitoring and illness response was successful in that only 5% of travelers, all of whom were low risk, were lost to follow-up. It also resulted in infrastructure investments that increased the state's preparedness for future infectious disease outbreaks.
Active monitoring and illness response was resource-intensive and needs to be evaluated against other possible responses to future infectious disease outbreaks.
Footnotes
Acknowledgments
The findings and conclusions presented in this article are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention or other institutions with which the authors are affiliated. Staff in the CDC Division of Global Migration and Quarantine and the Division of State and Local Readiness helped develop the proposal and interview scripts. Georgia Department of Public Health personnel Cherie Drenzek, Scott Minarcine, Michele Mindlin, Kelly Nadeau, Margaret Pence, and Wendy Smith, and Georgia Poison Control Center staff Stephanie Hahn and Gaylord Lopez, participated in multiple interviews. Brian Maskery provided significant helpful feedback on the manuscript. Any errors contained herein are solely the responsibility of the authors.
Appendix
Sample Allocations of Budget Line Items by Descriptions to Categories and Functional Areas by Funding Source
| Funding Source: Domestic Ebola Supplement to Epidemiology and Laboratory Capacity (ELC) | |
| Active Monitoring and Illness Response: Infrastructure | |
|
|
|
| Personnel | |
| Facility surveyor | Provide data to Georgia Department of Public Health (GDPH) and participate in GDPH training |
| Response planner | Outbreak response planner to work on scope of practice for Ebola and quarantine, oversee Ebola Active Monitoring System (EAMS), and work with district planners |
| Epidemiologist | Epidemiologist/physician; administrator for oversight of training, data collection as part of Ebola outbreak response, and reporting to GDPH |
| Epidemiologists 25% FTE | Link networks for Targeted Action Prevention, National Healthcare Safety Network, and SendSS for reporting and feedback reports for Ebola |
| Nurse | Infection control nurse to assess Ebola/non-Ebola facility certification |
| Information Technology | Development of notifiable disease modules; integration of disease and lab reporting into SendSS platform |
| Training | GDPH-sponsored Ebola virus disease (EVD) infection prevention training programs |
| Travel | GDPH training for outbreak management, meetings, and facility assessments |
| Travel to AMIR planning meetings and related conferences, such as Council of State and Territorial Epidemiologists | |
|
|
|
| Training | GDPH EVD biosafety training for Georgia Department of Public Health Laboratory Program |
| Funding Source: Public Health Emergency Preparedness (PHEP) | |
| Active Monitoring and Outbreak Response: Infrastructure | |
|
|
|
| Personnel | AMIR district planners |
| Information Technology | EAMS platform and integration with SendSS |
| Software license | |
| Telehealth build-out | |
| Training | Software training |
| SendSS user workshop | |
| Equipment | Telehealth equipment |
| Computers | |
|
|
|
| Information Technology | EMS SendSS module |
| Training | Training in use of personal protective and other equipment |
| Metro-Atlanta Ambulance Service training | |
| Fulton Country Hospital EMS training | |
|
|
|
| Training | Georgia Hospital Association training |
| Information Technology | Computers |
| Laboratory | Polymerase chain reaction supplies, reagents |
| Supplies | Computer software |
| Equipment | Equipment |
| Active Monitoring and Outbreak Response: Daily Monitoring | |
|
|
|
| Personnel | Medical epidemiologist |
| Ebola epidemiologist surveillance officer | |
| Ebola epidemiologist supervisory surveillance officer | |
| Weekend surveillance officer | |
| Weekend surveillance officer | |
| Manager | |
|
|
Fulton-DeKalb County hospitals call support |
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.