
Abstract
The ability to prevent, promptly detect, and appropriately respond to a public health threat is essential for health security. Field epidemiology training has helped increase the quality and quantity of the public health workforce to strengthen disease surveillance, outbreak preparedness and response, and general public health capacity. We conducted a desk review on the status of the Field Epidemiology and Laboratory Training Program model in 16 countries in West Africa. We also developed a questionnaire and shared it with West African Health Organization (WAHO) member states to document their experiences and the status of training in their countries. WAHO organized a regional 3-day consultative meeting with major stakeholders in the region to examine progress, gaps, and challenges, and outline a roadmap to strengthen the Field Epidemiology and Laboratory Training Program. Stakeholders shared their experiences, engaged in discussions to identify strengths and gaps, and made plans on a way forward. Member states are at different levels of implementing field epidemiology and laboratory training programs in their countries, and, therefore, major gaps remain in the number and distribution of trained epidemiologists throughout West Africa. Member states implement different variants of the program and in some instances the same cadre of health workers are trained in different but comparable programs with different funding streams. Two member states had not begun implementing the training program. Developing regional centers of excellence was recommended in the long term while collaboration among member states to train the required number of epidemiologists to fill the acute needs could be helpful in the short and medium term. Curriculum harmonization and expansion, deployment and use of trained epidemiologists, accreditation of training institutions, and generation of indigenous funding streams are recommended to improve the Field Epidemiology and Laboratory Training Program in West Africa.
Introduction
West africa has suffered from the effects of weak health systems resulting from a shortage of trained human resources, inadequate health infrastructure, inadequate cross-border collaboration, and other factors. In December 2015, the 75th session of the Council of Ministers of Economic Community of West African States (ECOWAS) mandated the establishment of the ECOWAS Regional Center for Surveillance and Disease Control (RCSDC) as the regional collaborative center of the Africa Centres for Disease Control and Prevention (Africa CDC). 1 Among other things, the RCSDC was tasked with focusing on disease surveillance; early warning and emergency preparedness response, including developing and functionalizing the ECOWAS regional rapid response team; public health laboratories systems and networking; training and research; and institutionalizing measures to ensure an adequate public health workforce in the region.
The Field Epidemiology Training Program (FETP) model was introduced in Africa as Public Health Schools Without Borders in Zimbabwe in 1993 to address workforce needs for disease surveillance and response. At its inception, FETP focused on medical epidemiologists, but as the need to address health threats in a more holistic manner using the One Health approach grew, other professionals, such as laboratorians and veterinarians, were included in the program. Consequently, the program was renamed the Field Epidemiology and Laboratory Training Program (FELTP) to reflect the laboratory component. Since 1993, other countries have adopted various field-based epidemiology training models focused on public health system strengthening through mentored field-based training. To address the human resource gaps at all levels of the public health system, FELTP includes frontline, intermediate, and advanced levels of training.2,3 FELTP hands-on training for the public health workforce is aimed at strengthening capacity in surveillance, data management, outbreak response, leadership, transborder disease control, and overall strengthening of the health system. 4 From their inception, FELTPs have contributed remarkably to improving the public health workforce in both quantity and quality. 5 As a result, these programs have been successful in strengthening public health and global health security.4,6 Figure 1 illustrates the 3 levels of field epidemiology training.
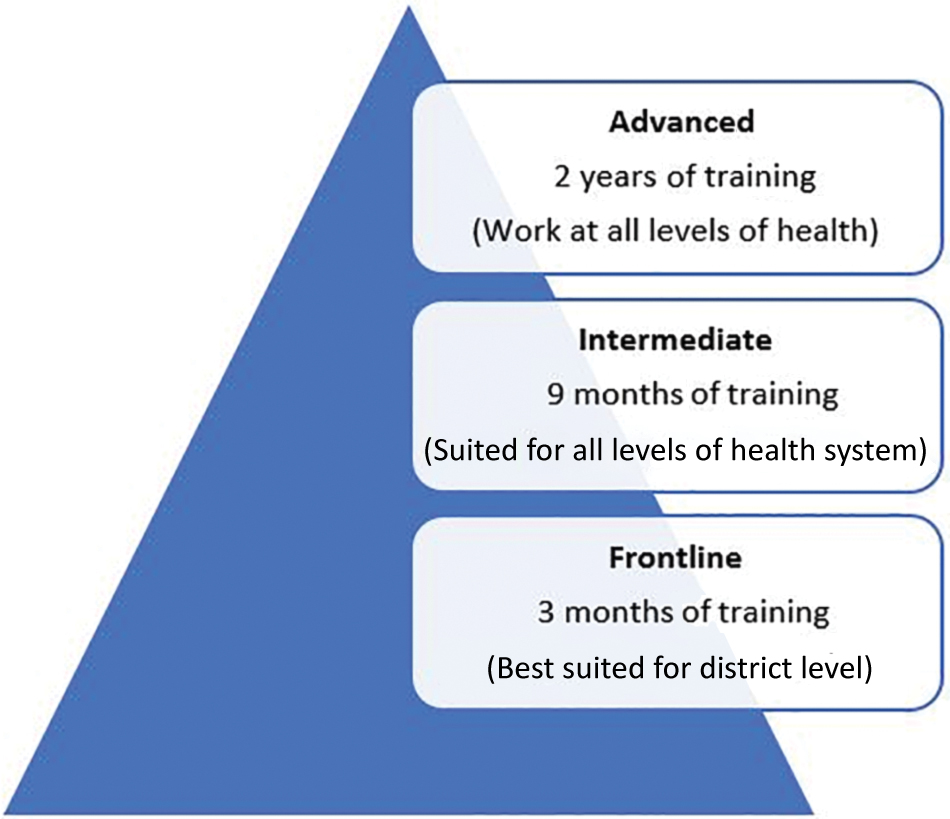
Three levels of field epidemiology training. Color images are available online.
The West African Health Organization (WAHO), as part of its role in strengthening workforce capacity across the region, organized a regional consultative meeting of ECOWAS member states (including Mauritania) in Abuja, Nigeria, to share experiences, identify gaps, and discuss strategies for strengthening and sustaining FELTPs in West Africa. The meeting was funded by the World Bank through the Regional Disease Surveillance Systems Enhancement project.
This article presents the status of applied epidemiology training programs in West Africa. It documents innovative approaches; discusses gaps, challenges, and opportunities; and provides a way forward for strengthening field epidemiology training to enhance health security in the region.
Methods
Desk Review
To describe the status of FELTPs in West Africa, we conducted a desk review of country-level program reports, the Global Field Epidemiology Roadmap report, 5 World Health Organization (WHO) Joint External Evaluation reports, and National Action Plan for Health Security documents. We also reviewed journal articles on FELTPs in the region. According to the WHO Joint External Evaluation tool, 7 the optimal target for surveillance is 1 trained epidemiologist (or equivalent) per 200,000 people who can systematically cooperate to meet relevant International Health Regulations (IHR; 2005) 8 and Performance of Veterinary Services core competencies. One trained epidemiologist is needed per rapid response team. Using the 2019 mid-year population projection by United Nation Department for Economic and Social Affairs 9 we determined the number of required epidemiologists (intermediate and advanced training) for member states and the region as recommended by the IHR.7,8
Questionnaire and Stakeholder Consultation
Member states and partners received a questionnaire by email that asked about data on national context; history of FELTP in their country; and current FELTP situation, funding, monitoring and evaluation, gaps or challenges, innovations, and lessons learned. The questionnaire did not include questions about names and contact details of respondents, and, therefore, it was not possible to identify who provided information on behalf of the country. Anonymity was not guaranteed, but confidentiality and privacy were maintained, and consent was implied.
Lastly, WAHO organized a 3-day regional consultative meeting on field epidemiology training in Abuja, Nigeria, on July 23-25, 2019. Meeting participants included heads of national public health institutes; heads of FELTP training programs, universities, and other institutions involved in the training; and partner institutions—including the US Centers for Disease Control and Prevention (US CDC), Africa CDC, African Field Epidemiology Network, Fondation Mérieux, Centre de Coopération Internationale en Santé et Développement, Food and Agriculture Organization, and Regional Animal Health Center. During the meeting, member state representatives shared how they have been running the FELTP programs and the resulting challenges, best practices, innovations, and recommendations. Question and answer sessions enabled participants to learn more.
Participants were divided into groups to brainstorm about the challenges and make recommendations for consideration by member states. Group work also provided opportunities for in-depth discussions about challenges and ways forward for FELTP training in the ECOWAS region. The plenary and discussion sessions were used to build consensus on the best regional approach to strengthening field epidemiology capacity for health security. Participant discussions resulted in several recommendations on a wide range of issues that arose during the 3-day deliberations. These recommendations were targeted at different stakeholders.
Results
Field Epidemiology Training Status in ECOWAS Region
The desk review revealed that FELTPs had not yet been implemented in all ECOWAS member states. Countries that had started FELTP were implementing the level of training most suitable to their immediate needs (Table 1). The frontline training, which focuses on training surveillance officers at the district level, seemed to be the most common tier currently being implemented in most countries, followed by the advanced-level training.
Status of Field Epidemiology and Laboratory Training Program Implementation by Level of Training, West Africa, July 2019
Mauritania is not an ECOWAS member state but is included in the Regional Disease Surveillance Systems Enhancement Project √ Program currently ongoing in the country.
Abbreviation: FELTP, Field Epidemiology and Laboratory Training Program.
The WHO Joint External Evaluation requires a minimum of 1,957 epidemiologists for the region; however, only 450 epidemiologists (graduates of intermediate- and advanced-level FELTP) had been trained in the region as of December 2018—23% of the target. The number of epidemiologists, however, varies greatly within the region. For example, Liberia met the required number of epidemiologists, but Cabo Verde, Niger, and Mauritania had not reported any trained epidemiologists. Nigeria, with the highest number of trained epidemiologists, achieved only 27% of its national target (Table 2). Nigeria has the greatest need for epidemiologists in terms of absolute numbers (Figure 2). Other key indicators in the WHO Joint External Evaluation include an updated multisectoral workforce strategy in place, availability of human resources to effectively develop IHR core capacity requirements, availability of in-service trainings, and a FELTP or other applied epidemiology training program.

Gaps in the number of frontline-level epidemiologists per 100,000 people by country in West Africa. Frontline FELTP gab/100,000 means the number of frontline FELTP graduates needed to meet the basic requirement of these workforce at district level. Color images are available online.
Distribution of FELTP Graduates in Countries by Level and Percentage of Target Reached, August 2019
Estimates based on United Nations Department of Economic and Social Affairs population estimate for each country. 9
The expected minimum number of epidemiologists in each country based on the Joint External Evaluation criteria of 1 epidemiologist (intermediate- and advanced-level FELTP graduates per 200,000 people). The percentage coverage estimates how many of the minimum target number of epidemiologists have been trained.
Abbreviation: FELTP, Field Epidemiology and Laboratory Training Program.
A huge gap exists between the number of properly trained public health workers available and the number needed to promptly detect and effectively respond to public health threats in every district in the region. These gaps are due to difficulties in recruiting suitable candidates, engaging and retaining qualified mentors, and funding challenges, among other factors. The distribution and use of trained epidemiologists is also suboptimal.
ECOWAS member states unanimously agreed during the meeting that there was a need to quickly strengthen the capacity of the existing workforce in the short term, while expanding the number of trained epidemiologists in the medium to long term. The member states were encouraged to progressively build their human resources in the immediate areas of need, while planning to attain and sustain the optimum quality and quantity of the health workforce in the long term. In the short term, collaborating with other countries might be more cost-effective in strengthening the public health workforce. Successful training programs abound in the region and resources could be pooled in countries that have already developed programs to help other countries rapidly strengthen their public health workforce. For example, Ghana, Nigeria, and the West African FELTP in Burkina Faso have successfully run advanced training programs for several years, resulting in a pool of graduates who are already integrated in the public health system in the region as well as a pool of trainers and training facilities. These countries have trained public health workers from other countries that do not have training programs and could serve as centers for regional training. Graduates from these countries could also be engaged in developing new training programs in the region. Pooling resources is not only a cost-effective approach but also bolsters regional collaboration and networking.
Training Package
FELTP is a service-based training program with the purpose of training public health workers in the principles and practices of field epidemiology as they provide service to their countries. It offers 3 levels of training: frontline, intermediate, and advanced. FELTPs help countries develop and implement dynamic, cost-effective public health strategies to improve and strengthen their public health systems and infrastructure. 10 These training programs offer competency-based training, comprising field epidemiology, health services management, disease control, health communication, and prevention effectiveness. 10
All of the countries that reported implementing the FELTP training package adapted the global curriculum with some modifications for their own local context. For example, some countries implemented the In-Service Applied Veterinary Epidemiology Training program, which emphasized veterinary and laboratory components of the curriculum at the district level, while other countries included environmental health components in their curriculum. Nigeria expanded the frontline FELTP curriculum to include previously standalone trainings offered by different partners to the surveillance officers at the district level in what is now called Integrated Training of Surveillance Officers in Nigeria. Table 3 shows the status of FELTP implementation by country.
Status of Field Epidemiology and Laboratory Training Program Implementation in West African Countries
Abbreviation: FELTP, Field Epidemiology and Laboratory Training Program.
Frontline
The focus on training frontline healthcare workers at the district level is to improve surveillance and response to priority diseases as part of the Global Health Security Agenda and IHR core capacity requirements. The goal of frontline-level training programs is to improve timely detection and prompt response to disease outbreaks and other public health threats by strengthening the epidemiological workforce capacity, thereby protecting the health of people locally and ensuring global health security. Trainees rely on data for monitoring the health of the community and improving basic surveillance data collection, analysis, interpretation, and communication; the quality and use of surveillance data for disease and outbreak detection and response, including case investigation and outbreak investigation; and the sharing and dissemination of health information.
Intermediate
Intermediate-level FELTP was generally introduced with the aim of training supervisors in managing disease response, strengthening public health surveillance, and providing mentorship. It is a 9-month intensive program that includes both classroom didactic lectures and a hands-on component in the field. This level of FELTP training produces a mid-level public health workforce—for both the national and subnational levels—that is able to take on a greater leadership role. This level of training requires a higher level of manpower and more stringent entry requirement compared to the frontline program. In some countries, having successfully completed frontline program with some years of field experience is a prerequisite for admission into the program.
Advanced
The advanced-level FELTP is a 2-year applied training program on the practice of epidemiology in a mentored environment, with a focus on “learning by doing.” Each trainee in the advanced program selects 1 of 3 tracks for study: medical epidemiology, laboratory epidemiology and management, or veterinary epidemiology. The veterinary epidemiology track focuses on addressing the ever-increasing threat of zoonotic infectious diseases and strengthens the collaboration between the human and animal health sectors—known as the One World, One Health concept.
All advanced FELTPs in West Africa have links with a university (Table 4) and grant master's degrees if a participant fulfills the university requirements, which usually includes successfully defending a master's dissertation. This is a common key requirement of all FELTP steering committees, mainly to enhance the career prospects of graduates. Universities also provide an academic anchor for the training program, which leverages the credibility of universities as the program starts up. The university faculty assists in teaching the didactic components of the course and FELTP staff strengthen the capacity of university faculty by showing them how the field-based training model works, thereby creating shared values between FELTP and the university. Each FELTP student has an academic supervisor or mentor from the university in addition to the program and field site supervisors. Involvement with the universities ensures that courses are offered on time every year through a competitive selective process, which also helps improve sustainability.
Field Epidemiology and Laboratory Training Programs in West Africa by Country and Level
Stakeholders
The framework for the implementation of the One Health approach generally involves the ministries of health, agriculture and livestock, and environment. National public health institutes, where operational, play a primary role in coordinating the various ministries. Each of these ministries serves as a source of trainees and provides field sites for hands-on training experience. Graduates of the program are reabsorbed into the government ministries, departments, and agencies to strengthen their core functions relating to health security.
International partners, including the US CDC, WHO, the World Bank, and Food and Agriculture Organization, were identified as providing strategic funding and technical support to FELTPs. Nongovernmental organizations such as African Field Epidemiology Network and the Centre de Coopération Internationale en Santé et Développement also provide technical support to member states in establishing and implementing the training programs. They support member states in quality improvement, preparing for accreditation.
Civil society organizations also support governments in strengthening the health workforce capacity. For example, Health Africa supports the government of Sierra Leone with logistics and operations of workshops and mentorship activities and provides technical assistance in public health workforce development.
Recruitment, Retention, and Use
The recruitment of trainees into different FELTP tiers varies among member states. In some countries, completion of the lower tier of the program is a prerequisite to be considered for the next higher tier. In other countries such as Ghana and Nigeria, however, trainees can be considered for the advanced-level program if they meet the requirements, without necessarily passing through frontline or intermediate programs. Each of these approaches has its merits and challenges. In some countries, the training functions as an in-service training, meaning the trainee is already working in the public health sector of the country. In other countries, it functions as a preservice training for anyone who is interested and meets the requirements. Some member states also reported an insufficient number of mentors and field supervisors.
We define retention as graduates staying and working within their home countries for at least 5 years after graduation. Member states reported challenges related to engaging and retaining graduates in various public health institutions. These challenges largely result from a lack of understanding in the health system about the role of FELTP graduates, an absence of clearly defined career paths for graduates the various ministries, and nonrecognition of the training in the statutory scheme of services of member states.
Accreditation and Continuous Quality Improvement
Accreditation is a process to ensure that FELTPs align with common standards that support quality training and increased recognition of their value in support of national public health priorities. 5 Thus far, only advanced-level FELTPs are accredited by the Training Programs in Epidemiology and Public Health Interventions Network (TEPHINET). Only 2 programs in the region are currently accredited by the TEPHINET Global Accrediting Body.
There is a lack of clarity about who should regulate the training in various member states—whether it should be regulated by universities, regional training bodies such as the West African College of Physicians, national regulatory bodies, or ministries of health and agriculture. This gap in clarity was noted during the consultative meeting in Abuja. Gaps related to the continuous quality improvement process for the program were also noted. There are currently no tools, indicators, quality benchmarks, or processes in place for continuous quality improvement.
Funding and Sustainability Issues
Funding for FELTPs is largely driven by donors, which is a major sustainability challenge for the ECOWAS region and many other regions and countries implementing the program. Major donors include the US CDC through the African Field Epidemiology Network, the US Agency for International Development, the US President's Malaria Initiative, and the World Bank through the West Africa Regional Disease Surveillance project and the Regional Disease Surveillance Systems Enhancement project. Other funders include the Bill & Melinda Gates Foundation and the Korea International Cooperation Agency. Host country ministries of health (and ministries of agriculture for programs with veterinarians) also contributed significant resources, usually as in-kind contributions (eg, space for the program, ancillary facilities, and field sites).
Almost all West African countries face challenges with dwindling donor funding. Programs in some countries, such as The Gambia, Mauritania, and Côte d'Ivoire, stopped their programs due to the lack of funding to sustain it. Other sustainability challenges reported by member states included shortages of technical staff for the training and mentorship.
The costs associated with implementation of FELTP include trainee costs in the form of university tuition, stipends, books, computers, and research support as well as program costs such as emergency response, local and international travel, office operational costs, field supervisory visits, field site support and technical assistance, and resident advisor salary and support.
Discussion
A successful FELTP helps the country and the region to meet IHR core capacity targets for the public health workforce in order to effectively prevent, detect, and respond to public health threats. It is a sustainable, accredited program with a holistic curriculum.
Meeting Workforce Capacity Building Targets
Increasing the quantity and quality of epidemiologists in the region is a priority in the short term. The deficit of epidemiologists (intermediate- and advanced-level FELTP graduates) in the region is huge. There are 3 advanced programs in West Africa: (1) the Burkina Faso FELTP, a regional program serving francophone and lusophone countries in West Africa; (2) the Ghana FELTP; and (3) the Nigeria FELTP. The capacity of these programs is limited, however. To meet the WHO Joint External Evaluation target for public health workforce capacity in the near future, there is an urgent need to increase the number of trainees who could be trained by these programs while maintaining the quality of both the training and trainees.
There is also a need for countries in West Africa to collaborate in the training of different cadres of human resources for health, contribute actively to the funding of training, and develop a roadmap for the active engagement of FELTP graduates in order to strengthen the regional health workforce. This collaboration is especially critical for providing mentoring opportunities, which will help bridge the gaps in countries where availability of mentors has been lacking. The shortage of human resources to mentor trainees is not limited to the ECOWAS region, and has been reported in other West African regions as well.11-13
Establishment of regional centers of excellence was recommended as a strategy for developing workforce capacity. A regional center of excellence is a technical organization established by a community of states with the mandate to provide specific services to member states. Such centers will have the support of the regional body in funding the training of the regional workforce. However, due to the rigorous and slow process involved in establishing such centers of excellence, it should be pursued in the medium to long term while exploring other strategies. A comprehensive workforce strategy should also be developed for the region to frame the various health workforce needs.
Recruitment, Retention, and Deployment
Some member states reported challenges with the recruitment of suitably qualified trainees for the programs, whereas others reported difficulties in retaining graduates within the public health sector and deploying them to solve immediate needs in the country. These challenges are not limited to the member states, as they have been reported by other countries implementing FELTPs. Retention rates ranging from 47% to 85% have been reported.2,15 High retention rates are not uniformly obtained across the different countries implementing FELTPs due to reported challenges in retaining the trained workforce. 16 These challenges are often associated with a lack of clarity in the career path after graduation. Countries often do not have a clear scheme of services and career paths for the field epidemiologists who have completed the training programs. Graduates, therefore, seek opportunities outside the public health sector (where their skills are most needed) due to the lack of integration between the training program and the health system. This lack of integration has limited the full use of trained epidemiologists and their subsequent retention in the health system. Some countries have made progress in this regard.17-19 South Africa 18 and England 19 have taken some steps to address the integration of trained epidemiologists by setting up a working group to highlight unmet needs and develop a distinct career path for applied epidemiology. In addition to developing a career path, they have also worked to standardize the curriculum, competencies, and accreditation process of the training program.
Mentorship is essential to the success of the program; however, member states have reported difficulties engaging and retaining mentors in the training. 20 Different models of mentorship exist in the region, and the meeting encouraged the use of a mix of strategies. For example, intermediate- and advanced-level graduates can serve as mentors for the frontline-level training programs, part-time mentors could be engaged to serve specific needs (where applicable), and mentors could be integrated into the rapid response teams or engaged in other activities that improve the interactions they have with mentees. Clear, measurable targets should be set for each mentorship relationship and there should be an objective assessment of the mentorship exercise.
Curriculum Harmonization and Expansion
Harmonizing and expanding the training program curriculum has been a topic of discussion among trainers, especially in regard to the expansive nature of applied epidemiology. Throughout the region, the different FELTP curriculums have their strengthens and challenges. However, member states called for an inclusive, yet universal curriculum for training the public health workforce in the region while allowing each country to adapt the curriculum to address local needs and national priorities. For example, the curriculum should include a basic minimum knowledge possessed by every graduate and yet it should be inclusive and adaptable to allow members states to incorporate other aspects to meet their needs. Having a harmonized regional curriculum for every level of FELTP, with a minimum irreducible standard, will help align these training programs and ensure standardization of the products. It will also help ease cross-border migration and collaboration. A universal curriculum is expected to include animal, environmental, human health, and laboratory components. An example is the recent effort in Nigeria to integrate standalone courses into the frontline-level training program. 14 RCSDC is expected to play a leadership role in ensuring this harmonization. The process will include all major stakeholders, bringing together all those implementing FELTPs or other similar training programs. The universal curriculum should also include emerging areas of public health such as public health informatics, injury epidemiology, and health systems research and knowledge translation.
Curriculum harmonization is also expected to help member states give proper recognition to the skill sets unique to field epidemiologists and to facilitate their integration into national public health systems. A standardized curriculum will also allow for easy transfer of trained public health workers to any part of the region. The ability of program graduates to work anywhere in the region will help increase surge capacity within the region and beyond.
Accreditation and Continuous Quality Improvement
There is an ongoing debate about whether every FELTP program should be accredited, whether the accreditation should be internal or external and whether it should be done by a regional or global accreditation body. Many stakeholders believe that having the training accredited by a national regulatory or accreditation body is important, but they also believe that maintaining a minimum global standard for every FELTP trainee and graduate is critical. 21 Member states recognized these ongoing conversations and agreed there is a need for each training program to be recognized by the host country and for the training programs to be accredited by the host country's statutory regulatory authorities in order to enable faster integration and acceptance by government institutions. Stakeholders also agreed on the need for regional accreditation, especially for frontline and intermediate-level FELTPs, which are not currently accredited by the TEPHINET Global Accrediting Body. Regional accreditation should be handled by WAHO in collaboration with selected stakeholders. In addition to regional accreditation, the African Field Epidemiology Network Star Rating System, a system for rating member programs based on set productivity and quality performance criteria, will ensure conformity to set standards and encourage continuous quality improvement among programs in the network.
RCSDC is expected to develop standard tools and indicators for monitoring the programs and for continuous quality improvement in collaboration with other partners and organizations. The alumni network in the region needs to be strengthened for the strategic roles they are likely to play in the overall training of epidemiologists. The alumni could support mentoring and, in some cases, cross-border collaboration in training, surveillance, and response.
The member states in collaboration with RCSDC need to develop a strategic public workforce development plan for the region, which the member states could adapt to their local needs and context. This plan, especially at the national level, needs to include a database of FELTP alumni and mentors as well as training plans and budget lines to support the mentorship program. The region also needs a log frame matrix for workforce development, a monitoring and evaluation framework, and tools for epidemiology training in the region.
Funding and Sustainability Issues
Identifying an appropriate and sustainable funding mechanism for FELTPs has been a challenge in the ECOWAS region. There has been little commitment to funding support from local stakeholders.22,23 The funding challenge poses a threat to the sustainability of the program in some countries.11,13,16,21 Other countries, however, have made progress in providing funding support for FELTPs. In South Africa, local funding has become the primary source of financial support for the program. 18
Different models for ensuring a sustainable funding sources exist. Having a funding mix led primarily by the government budget has been the preferred model, with private and donor funding playing supportive roles. Host governments are encouraged to take ownership of the program and ensure it is included in the national budget. To ensure sustainability and recognition of the program, governments also need to decide whether it should be an in-service training or preservice training, or a mixture of both. Doing so will facilitate the appropriate placement of graduates in the public health system, ensuring there is a career pathway for each trainee.
Cost standards should be identified by the programs to ensure efficiencies, including an optimum cost for training a resident under certain predefined conditions. This will allow for cost effectiveness and may encourage more focused spending. Universities could be encouraged to absorb some costs associated with the training as their contribution to the partnership. Member states need to develop strategic ways of driving down the unit cost of training, for example, using field-based supervisors and mentors and recruiting trainees with requisite professional experience. There is a critical need to expand funding support for FELTPs, given their enormous contribution to global health security. This option is already being considered by all FELTP stakeholders. 5
Other forms of sustainability also need careful consideration—such as maintaining an adequate combination of training staff, ensuring the training cycle sustains output, securing a pool of subject-matter experts, and maintaining adequate training and administrative skills required to manage the training. Another important consideration in the sustainability discussion is where to host FELTPs. Some countries host FELTPs within their national public health institute, whereas others host the programs in the ministry of health or a university. Other variations also exist. Although consensus on where to host FELTPs seems to be lacking, each model has reported successes, merits, and challenges. While the discussion continues, each member state is encouraged to adopt a model that best meets their needs.
RCSDC and ECOWAS member states need to jointly develop the regional and local sustainability plan. International partners should mainstream FELTP in their programming and develop an exit plan. In the short term, RCSDC together with member states should continue to secure funding for FELTP training and advocate for improved budgetary allocation and disbursement by national governments.
Way Forward
RCSDC, ECOWAS member states, and partners each play a critical role in improving FELTPs, thereby strengthening public health capacity to prevent, detect, and respond to public health threats in West Africa. RCSDC, under the supervision of WAHO, champions the need for improved coordination of FELTPs, standardized curriculum, deployment of graduates in cross-border disease surveillance, information sharing, and outbreak preparedness and response in the region. RCSDC is expected to develop a regional strategic plan for developing a field epidemiology program that includes an advisory committee to maintain broad-based support from stakeholders and partners, establish minimum standards for regional FELTPs, conduct a cost analysis for different training modalities, develop a detailed roadmap for advanced-level FELTPs, develop a framework for financial sustainability plans and advocacy tools, and clearly define the regional and national monitoring and evaluation plan beyond just the number of people trained. The monitoring and evaluation plan is expected to evaluate trainee competencies during and after training, evaluate the impact of the program at country and regional levels, and define capacities and the level of coverage needed at national and regional levels. RCSDC is also expected to:
Support advocacy and establishment of regional funding mechanisms to support the training by advocating at the highest government levels for epidemiology training programs as key components of health security and economic growth. Convene a field or applied epidemiology technical working group and establish goals for program staffing (both technical and administrative), with roles and responsibilities including leadership roles and mentorship of trainees: ○ Discuss adoption and implementation of policies from the international and continental levels (eg, Africa CDC), RCSDC, and ministries of health to promote development of the public health workforce. ○ Develop strategies to enhance job placement, retention, and career development for trained epidemiologists. ○ Design models for career progression among ECOWAS members. ○ Support the development of standards and accreditation processes and mechanisms for training programs. Disseminate field or applied epidemiology training materials, protocols, standard operating procedures, and toolkits. Conduct cost analysis for different training modalities. Promote health research and cross-border collaboration. Develop training and standard operating procedures for mentors and supervisors. Establish accreditation mechanisms for health training institutes.
Member states are strongly encouraged to urgently add FELTP training to their national budgets or increase the budgetary allocation for training, have an appropriate regulatory body recognize FELTP training, develop a strategic plan for public health workforce development, and optimize the retention and equitable distribution of trained epidemiologists in various states. Member states are expected to:
Develop a strategic plan for the development of a field or applied epidemiology program that includes an advisory group and governance structure with stakeholders and allows for the development of goals and objectives for national (or regional) applied epidemiologists.
Prioritize the training of a specific cadre of epidemiologists to meet national priorities and needs.
Support collaboration among various sectors including human health, animal health, environmental sectors, and other relevant sectors, and support engagement to determine readiness for a field or applied epidemiology program and potential career paths for graduates.
Evaluate existing field or applied epidemiology programs in the region and identify a host country where national public health professionals can be sent for training.
Secure an agreement with another country to host participants and establish funding mechanisms to support the training.
Track the training and rostering of field or applied epidemiology participants and graduates in a host country.
Identify a sustainable funding mechanism for field or applied epidemiology training programs; consider beginning with frontline-level training, with a plan for expanding to intermediate and advanced levels, as determined by country needs.
Designate field supervisors and mentors for field or applied epidemiology training and prepare guidelines for mentorship including monitoring of trainee activities, development of projects, and barriers to training.
Establish a partnership with other countries in the region to share epidemiology training program graduates during emergency events.
Partners are expected to coordinate funding support and provide technical support to member states and the region to achieve regional objectives of increasing the number and distribution of highly trained public health workers for better health and security for all.
Conclusion
Competent, well-motivated field epidemiologists are needed for functional and sustainable public health surveillance and response at all levels of the health system. Coordinating and strengthening the FELTP model in the region will contribute to a public health workforce that can effectively prevent, detect, and respond to public health threats. Critical lessons learned in West Africa include the need for strong commitment and ownership among member states, effective collaboration of major stakeholders, and the strategic role of regional health organizations in fostering collaboration and support for FELTPs.
Member states must commit to a sustainable public health workforce development both politically and financially. This includes making budgetary provisions and structural adjustments to train and use the public health workforce. Technical partners including WAHO, ECOWAS/RCSDC, US CDC, the World Bank, African Field Epidemiology Network, WHO, Africa CDC, national public health institutes, and universities need to foster effective collaboration and support member states and the region to achieve this critical mandate. Finally, regional health organizations must actively lead member states to commit more and support them in developing sustainable regional health security.
Footnotes
Acknowledgments
We acknowledge the funding support from the World Bank through the Regional Disease Surveillance Enhancement project and valuable contributions from partners and ECOWAS member states representatives in organizing the regional consultative meeting. We appreciate their roles before and during the meeting.