
Abstract
Mass vaccination is a crucial public health intervention during outbreaks or pandemics for which vaccines are available. The US government has sponsored the development of medical countermeasures, including vaccines, for public health emergencies; however, federally supported programs, including the Public Health and Emergency Preparedness program and Cities Readiness Initiative, have historically emphasized antibiotic pill dispensing over mass vaccination. While mass vaccination and pill dispensing programs share similarities, they also have fundamental differences that require dedicated preparedness efforts to address. To date, only a limited number of public assessments of local mass vaccination operational capabilities have been conducted. To fill this gap, we interviewed 37 public health and preparedness officials representing 33 jurisdictions across the United States. We aimed to characterize their existing mass vaccination operational capacities and identify challenges and lessons learned in order to support the efforts of other jurisdictions to improve mass vaccination preparedness. We found that most jurisdictions were not capable of or had not planned for rapidly vaccinating their populations within a short period of time (eg, 1 to 2 weeks). Many also noted that their focus on pill dispensing was driven largely by federal funding requirements and that preparedness efforts for mass vaccination were often self-motivated. Barriers to implementing rapid mass vaccination operations included insufficient personnel qualified to administer vaccinations, increased patient load compared to pill-dispensing modalities, logistical challenges to maintaining cold chain, and operational challenges addressing high-risk populations, including children, pregnant women, and non-English-speaking populations. Considering the expected availability of a severe acute respiratory syndrome coronavirus 2 vaccine for distribution and dispensing to the public, our findings highlight critical considerations for planning possible future mass vaccination events, including during the novel coronavirus disease 2019 pandemic.
Introduction
During a pandemic, rapid distribution and dispensing of medical countermeasures (MCMs) is a vital aspect of response efforts, and mass vaccination is particularly crucial during pandemics for which vaccines are available. In fact, the US Pandemic Influenza Preparedness Plan identifies vaccination as “the most effective medical intervention for mitigating the potentially devastating impact of an evolving pandemic.” 1 The US government maintains stockpiles (eg, Strategic National Stockpile, National Pre-Pandemic Influenza Vaccine Stockpile) of a variety of MCMs for use during a public health emergency—including vaccines for smallpox, anthrax, and H5N1 avian influenza—with the expectation that rapid, large-scale mass vaccination could be necessary in response to such events.2,3
After the 2001 anthrax attacks, the United States established federally funded programs to support distributing and dispensing MCMs provided to state and local jurisdictions during emergencies. The Public Health Emergency Preparedness (PHEP) program and Cities Readiness Initiative (CRI), administered by the US Centers for Disease Control and Prevention (CDC), provide funding and guidance to states and several major cities to develop response plans and conduct exercises for MCM dispensing. 4 Created in response to the deliberate release of anthrax, 5 PHEP and CRI have largely focused on enabling jurisdictions to rapidly dispense oral antibiotics rather than mass vaccination operations, although mass vaccination is also a component of response to an anthrax attack. More recently, however, there has been increased attention on improving the mass vaccination component of MCM dispensing for pandemic influenza (Figure 1). For the 2019-2024 PHEP performance period, the CDC provided planning guidance and exercise requirements for PHEP recipients and CRI jurisdictions (Table 1) for both an intentional release of a Category A agent (eg, anthrax) and an emerging infectious disease (eg, pandemic influenza). A select set of high-risk CRI jurisdictions still must focus on an intentional release of anthrax as their primary planning scenario. 5
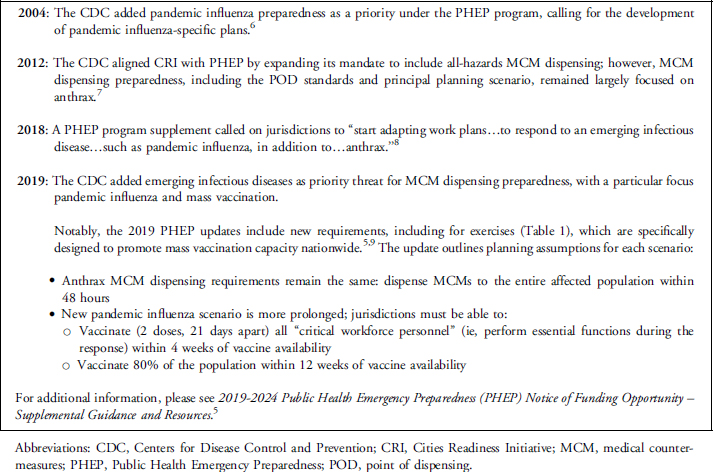
Context and background information about key aspects of PHEP and CRI guidance since 2004.
Updated PHEP and CRI exercise requirements 5
Abbreviations: CRI, Cities Readiness Initiative; MCM, medical countermeasures; N/A, not applicable; PHEP, Public Health Emergency Preparedness.
The response to the 2009 H1N1 influenza pandemic is the one of the most recent and relevant examples of large-scale mass vaccination in the United States.10,11 During this response, delays in vaccine availability reduced the number of vaccines administered and lengthened the timeframe for vaccination campaigns. Despite the role these factors played in limiting the scale of rapid mass vaccination, state and local jurisdictions experienced substantial challenges in vaccinating their populations, illustrating the need to improve mass vaccination preparedness. 12 The interviews for this study were conducted prior to the emergence of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) in December 2019, but the ongoing coronavirus disease 2019 (COVID-19) pandemic appears likely to require a global mass vaccination effort if and when a vaccine becomes available. While a fully tested and approved vaccine will likely not be available for months or longer, planning must begin now to ensure that local operational capacity is in place to enable successful implementation of mass vaccination programs on short timelines across the country and around the world.
There has been insufficient evaluation of the operational capacity to conduct large-scale, rapid mass vaccination nationally since the 2009 H1N1 pandemic. Multiple efforts—including the Trust for America's Health Ready or Not report, 13 the National Health Security Preparedness Index, 14 and 2 peer-reviewed studies15,16—have examined at an aggregate level state and local health departments' abilities to dispense MCMs; however, they have not specifically examined the capacities to conduct mass vaccination operations during public health emergencies, including pandemics. Additionally, studies that address MCM dispensing often lack a clear distinction between the operational needs of mass vaccination versus pill dispensing,17-19 report on experiences of a single population or jurisdiction,20-23 and/or discuss mass vaccination during smaller-scale outbreaks or in nonemergency settings.24,25
Considering the dearth of assessments of mass vaccination operations or US readiness to conduct mass vaccination, and the long-standing focus on anthrax and pill-based MCM dispensing modalities, we interviewed jurisdictional representatives to understand their experiences preparing for or conducting mass vaccination. We aimed to determine the current state of mass vaccination preparedness in the United States, identify outstanding challenges and barriers to establishing this capacity at the local level, and share lessons from those with operational experience in order to support mass vaccination efforts in other jurisdictions.
Methods
This study consisted of semistructured key informant interviews with a total of 37 individuals from 33 jurisdictions from December 2018 through March 2019 (Figure 2; Supplemental Table 1 www.liebertpub.com/doi/suppl/10.1089/hs.2019.0146). We identified prospective interviewees through a review of peer-reviewed literature, existing professional relationships, and collaboration with the National Association of County and City Health Officials (NACCHO). NACCHO announced our research project via its member email listserv, and we emailed additional information to those who expressed interest in participating, including that interviews would be conducted on a not-for-attribution basis. Additionally, we obtained verbal consent to record interview audio for internal note-taking purposes and reiterated that no statement would be attributed to them or their organization without their explicit consent. We used a purposeful sampling methodology to include jurisdictions with diversity in geographic location and mass vaccination experience. 26 The CDC published updated PHEP guidance and requirements during the interview period, which included changes to MCM planning and exercise requirements. All but 5 interviews were conducted prior to the publication of updated PHEP guidance in March 2019, so the interviews largely focused on preparations and planning conducted under the previous version of PHEP guidance.

Map of states represented by at least 1 interviewee. Created with mapchart.net.
Interviewees included local and state health officials involved in preparedness and vaccination activities, including health department epidemiologists, public health nurses, and emergency preparedness coordinators. We developed an interview framework based on themes identified through a review of relevant peer-reviewed literature and our professional experiences and expertise. The framework included general questions about the interviewees' experiences conducting mass vaccination, the circumstances of mass vaccination operations, and relevant challenges and lessons learned. Although we used the framework in each interview, the interviewees largely dictated the interview topics based on their own experiences and priorities. We recorded interview audio to supplement our interview notes during the analysis, however, all interviews were conducted on a not-for-attribution basis to promote transparency.
We performed thematic coding on interview notes using NVivo 12 for Windows (QSR International, Melbourne, Australia) qualitative data analysis software to identify recurring themes, challenges, and lessons learned. Interview notes were divided among 3 researchers, who coded on 6 principal themes: operational and planning guidance, impetus for mass vaccination planning, current and previous mass vaccination experience, mass vaccination staffing, vulnerable populations, and mass vaccination operations and logistics. These researchers then further analyzed the content within these themes to identify the primary findings.
This research was determined to not qualify as human subjects research by the Johns Hopkins Bloomberg School of Public Health Institutional Review Board.
Results
Mass Vaccination Has Unique Operational Needs
Interviewees stressed that certain operational requirements for mass vaccination—such as personnel qualifications, point of dispensing (POD) throughput and volume, documentation, and cold chain requirements—differ substantially from pill dispensing. Interviewees consistently noted that the need for and limited availability of trained vaccinators could substantially limit POD throughput. Unlike pill dispensing, vaccinators are required to have specific training and licensing, which can limit the number of individuals available to administer vaccinations, and vaccination PODs also face increased patient volume compared to pill dispensing. Pill-dispensing PODs can use a head-of-household model (ie, individuals can receive MCMs for multiple other people) to reduce the total POD patient volume, but this is not an option for vaccination. Each individual must be present to receive a vaccine, which increases the patient load on PODs and poses challenges for providing security for POD operations. Additionally, several interviewees anticipated that novel vaccines or formulations during a pandemic, including those in clinical trials, could necessitate lengthy education, consent, and documentation processes that would further slow POD throughput, particularly for populations such as children and pregnant women. While a small minority of interviewees cited cumbersome paperwork and screening/triage processes for anthrax antibiotics as a major operational limitation, most interviewees agreed that mass vaccination posed greater challenges. Unlike most pills, vaccines typically require a cold chain to remain effective. Several local jurisdictions reported possessing limited cold chain capacity to support community-wide mass vaccination. Interviewees specifically cited identifying sufficient freezer space for vaccine storage and maintaining the cold chain during vaccine distribution as key logistical challenges, and several discussed purchase and maintenance costs for vaccine freezers as being financially prohibitive. One participant noted that community partners can offer some temporary vaccine freezer capacity, but it is often limited and fixed in location and, thus, not available for vaccine distribution. While many aspects of mass vaccination operations overlap with pill dispensing, dedicated mass vaccination plans are needed to address unique differences.
The additional logistical and operational constraints associated with mass vaccination necessitate consistent and dedicated preparedness efforts to ensure operational capacity, but there was substantial variation among jurisdictions with respect to mass vaccination planning. Some jurisdictions did report focusing their MCM dispensing planning efforts on mass vaccination, as opposed to pill dispensing, citing their belief that vaccination was a more likely scenario for their jurisdictions than an anthrax release. Others noted that they primarily focused on anthrax pill dispensing, generally as a result of federal funding requirements; however, this could be affected by whether the interviewee represented a CRI jurisdiction. Several interviewees noted that expanding their current MCM plans to include pandemic influenza vaccination would constitute a major shift in priorities due to the additional requirements of administering vaccines, but a few jurisdictions viewed these as relatively minor issues that could be readily integrated into existing MCM dispensing plans. In fact, some interviewees commented that an anthrax scenario presented greater challenges than pandemic influenza due to the need for multiple rounds of POD operations—3-day and full courses of antibiotics, plus vaccination—and the complexity of screening for 2 or more kinds of antibiotics. A small number of interviewees indicated that they had operational plans to conduct community-wide vaccination but planning in many jurisdictions was at a higher level and with less specificity than for pill dispensing. Regardless of the variation in interviewees' planning efforts, dedicated and continued mass vaccination planning efforts are required to ensure pandemic preparedness.
While many jurisdictions discussed ongoing or recent vaccination efforts, including outbreak responses, seasonal influenza vaccination clinics, or school-based clinics for routine childhood immunizations, mass vaccination planning scenarios often reflected jurisdictions' experiences during the 2009 H1N1 influenza pandemic. The exact planning assumptions varied by jurisdiction, but many assumed that initial vaccine availability would be limited and distributed gradually, such that priority groups would be vaccinated first, followed later by the general public as vaccine production increased. This would result in smaller initial patient load and would spread the patient volume across a longer timeframe, giving them additional time to plan and coordinate with community partners such as pharmacies. Based on these assumptions, many interviewees believed that the need to vaccinate their entire jurisdiction in a highly constrained timeframe was not realistic.
Additional Planning Needed for Vulnerable Populations
Accessing vulnerable and high-risk populations remains a challenge for mass vaccination planning and operations, and jurisdictions' planning efforts to meet the needs of these populations vary substantially. Interviewees most commonly cited children and pregnant women as priority populations, as they are often at high risk for severe disease and complications. Additionally, potential vaccinators may require specialized training, experience, and licensure to vaccinate, which further limits the pool of available vaccinators. Licensing concerns also hindered some plans to use pharmacists to increase vaccinator availability, because their limited vaccine administration authority does not typically include populations like young children. Some interviewees noted that immigrant and non-English-speaking populations also required additional resources for effective engagement, including translation services for public communication and education campaigns as well as direct patient interaction (eg, POD screening), which require additional funding and planning for POD operations.
The extent to which jurisdictions have considered the needs of vulnerable populations and incorporated them into existing response plans varies widely. Some interviewees noted that their jurisdictions acknowledged the challenges posed by certain vulnerable populations but had not yet developed plans to address them. Others targeted specific populations during exercises and mass vaccination events, such as seasonal influenza vaccination clinics, and several had already included some vulnerable populations, predominantly children, in their mass vaccination plans. Several interviewees noted that vaccinating certain vulnerable populations, including the elderly and children, was more feasible and convenient through drive-through POD models; however, others noted that this modality posed additional challenges, particularly for children in car seats. Despite these efforts, every interviewee acknowledged that gaps remain with respect to incorporating vulnerable populations into mass vaccination preparedness.
Rapid Scale-Up Is Not Feasible for Many Jurisdictions
To gauge the upper limit of existing mass vaccination capacity, we asked interviewees if their jurisdiction could vaccinate the vast majority of their population within a short period of time (eg, approximately 1 to 2 weeks). We determined that this was a worst-case situation in terms of mass vaccination operations and served as an analogue to existing anthrax planning guidance on providing antibiotics to everyone within 48 hours. While a few interviewees expressed some confidence in their ability to mount this kind of response, nearly all indicated that mass vaccination on this scale and timeline would be highly challenging and likely not feasible. Some interviewees felt that accomplishing mass vaccination at this scale would be marginally easier for influenza than other pathogens, largely due to the public's and responders' familiarity with the disease and vaccine, but still not likely.
A commonly cited reason for this lack of confidence was limited experience undertaking or preparing for such a situation, as no jurisdictions expressed having experience implementing vaccination operations on this scale. While the 2009 H1N1 influenza pandemic was the most relevant example of widespread mass vaccination, many interviewees reported that their response was very resource intensive despite targeting smaller priority populations over a more prolonged timeline. Interviewees estimated that the total number of vaccinations administered in their jurisdiction during the 2009 H1N1 response ranged from fewer than 10,000 to nearly 50,000, which generally translated to a small fraction of each jurisdiction's total population. Additionally, many interviewees noted that they began working at their health department after the 2009 H1N1 pandemic, and while jurisdictions may have documented lessons from that response in after-action reports, staff turnover could mean that valuable firsthand knowledge from those operations has been lost.
Jurisdiction vaccination planning experience typically stemmed from smaller events such as tabletop and functional exercises, seasonal influenza or school-based vaccination clinics, and outbreak responses. Numerous interviewees discussed annual seasonal influenza vaccination clinics as a primary way that their jurisdiction implemented mass vaccination; however, clinic sizes were far smaller than what would be necessary for a major outbreak or pandemic, ranging from fewer than 200 to slightly more than 2,000 recipients. Some interviewees noted that the increasing number of distributed, private-sector influenza vaccine providers in their communities, including pharmacies and supermarkets, has shifted patient load away from seasonal vaccination clinics. Multiple interviewees discussed school-based vaccination—for influenza and other diseases—as useful opportunities to practice vaccination, albeit on smaller scales. Several interviewees also discussed how local outbreaks can provide opportunities to exercise community-based vaccination operations. Recent outbreaks—for example, of measles, mumps, and hepatitis A—in some jurisdictions required mass vaccination, including opening PODs in some cases, but these responses involved limited affected populations and did not sufficiently test the capacity necessary for a community-wide outbreak or pandemic. Tabletop and functional exercises offer opportunities to test certain mass vaccination plans and capabilities, but the limited scale and duration of these exercises and associated simulations (eg, vaccine administration) are not necessarily sufficient to fully test operational capacity.
Mass Vaccination Staffing Remains a Major Gap
Staffing PODs with credentialed vaccinators was the most prevalent challenge to conducting large-scale mass vaccination operations cited by interviewees. As noted previously, specialized training and licensing is required to administer vaccinations, so lay volunteers cannot perform this function like they can for pill dispensing. Interviewees indicated that health departments do not have enough trained vaccinators to implement mass vaccination operations, and capable vaccinators can be in relatively short supply in a given community.
Interviewees discussed the value of community partnerships for identifying available vaccinators during emergencies and explicitly noted the importance of establishing these relationships in advance of an outbreak or epidemic. Interviewees identified law enforcement, schools, community groups, and the private sector health system, including medical/nursing schools, pharmacies, and assisted living facilities, as excellent sources to supplement internal vaccinator capacity. Interviewees also discussed the Medical Reserve Corps as a potential source of vaccinators; however, few expressed confidence in their ability to rely on the Medical Reserve Corps to provide vaccinators during a pandemic, out of concerns that many of these skilled volunteers will also be in demand by local healthcare facilities. Several interviewees expressed increased confidence in implementing mass vaccination if they could draw personnel from nearby jurisdictions—or state or federal partners—or if they had advance warning to aid in planning, including coordinating with community partners. These personnel, however, may not necessarily be available during a widespread pandemic. The combination of a limited vaccinator pool and increased POD volume, due to the need to be physically present to be vaccinated, poses severe limitations on jurisdictions' capacity to conduct vaccination on a large scale. Most interviewees acknowledged that there will likely be a deficit of vaccinators for large-scale responses, even if all available personnel are utilized.
Enhanced Federal Guidance and Support Are Needed
The historical focus on pill dispensing in past MCM planning guidance has contributed to reduced emphasis on specific planning for mass vaccination, and uncertainty regarding what activities satisfy funding requirements, including how preparedness funds could be spent, potentially hindered mass vaccination preparedness. Many interviewees noted that local jurisdictions' preparedness and planning priorities are largely driven by PHEP funding requirements, which focused predominantly on pill dispensing for many years. Some interviewees discussed how the focus on anthrax and pill dispensing limited the attention they could give to mass vaccination preparedness, and many jurisdictions that undertook mass vaccination planning indicated that their efforts were largely self-motivated. Several interviewees commented that their jurisdictions would prefer to focus on mass vaccination, as pandemic influenza is a more likely threat than anthrax, but past federal funding requirements drove their MCM efforts toward pill dispensing.
Interviewees also described differences in the planning and exercise efforts they found to be sufficient in meeting PHEP funding requirements and expressed confusion regarding how federal preparedness funds could be spent. Some jurisdictions discussed using their vaccination efforts, such as for pandemic influenza, to satisfy the requirements of federal grants, while others indicated they were required to focus on pill dispensing to receive funds. Some of this variation, however, could be impacted by whether the interviewee represented a CRI jurisdiction. Several interviewees discussed using federal funds to purchase vaccines for use in mass vaccination events and exercises, but others stated that they were not permitted to do so. Additionally, some jurisdictions used federal funding to purchase vaccines for uninsured individuals, first responders, and outbreak responses as well, but this was not consistent across all participating jurisdictions. Several interviewees commented that sustained and increased communication from federal and state partners was needed to understand past guidance, and some also noted that states' interpretations of federal grant requirements were a major factor in the practical application of federal funding. These uncertainties and communication challenges likely contributed to the disparities in mass vaccination capacity discussed previously, and continued guidance and support from the federal level is needed to promote continued progress on mass vaccination.
Discussion
The ability to rapidly vaccinate an affected population can be vital for response efforts during severe pandemics, and existing federal plans to utilize stockpiled vaccine rely on this capability. National efforts to develop MCM-dispensing capabilities, however, have largely focused on pill dispensing in the past. There have been limited recent national assessments of state and local health departments' mass vaccination capabilities, but experiences during the 2009 H1N1 pandemic suggest that enhanced planning is needed.
The longstanding focus on anthrax and associated pill-based MCM dispensing models has hindered some jurisdictions' efforts to develop dedicated mass vaccination plans due, in part, to the importance of satisfying specific federal grant and assessment requirements. Jurisdictions that have developed mass vaccination plans were largely self-motivated, without the benefit of specific federal guidance on associated planning scenarios and assumptions. In March 2019, the CDC issued an update to the PHEP program, which includes a focus on pandemic influenza and provides planning guidance and exercise requirements for mass vaccination (Table 1). 5
The inclusion of specific guidance for pandemic influenza and mass vaccination could help the PHEP program better address some of the gaps observed in this study, but it may not be a perfect solution. For example, the emphasis on pandemic influenza varies by the type of jurisdiction, which could contribute to disparities in mass vaccination capabilities. Regardless, interviewees indicated that the increased attention on vaccination in federal funding programs is an important, positive development. Our analysis, however, was largely conducted prior to this point, so it was not possible to evaluate the impact these changes will have on mass vaccination capabilities. It will take time to assess the effect of the updated PHEP program on mass vaccination operational capacity.
The PHEP update includes a pandemic influenza planning scenario, which mirrors assumptions that we heard from interviewees. Much like the 2009 H1N1 pandemic, the PHEP planning scenario assumes limited initial vaccine availability, which necessitates vaccinating limited priority populations before expanding to the general public over several months. 5 These assumptions may be appropriate for certain events, but they do not cover the breadth of scenarios that could require mass vaccination. A smallpox attack or avian influenza epidemic, for example, could require rapid jurisdiction-wide vaccination, and vaccine stockpiles exist for these diseases and could be deployed for immediate use. Additionally, meeting even the prolonged timeline in the PHEP pandemic influenza guidance would require substantial planning and resources at the local level, as many jurisdictions have limited experience with large-scale mass vaccination during an emergency. One key area that may be beneficial to local health officials is the allocation of initial limited supply to priority populations. Existing documents, published by the CDC for pandemic influenza, provide support for identifying and engaging priority populations. 27 While this guidance was explicitly developed for pandemic influenza, it can inform other emergencies as well; for example, it is a model for SARS-CoV-2 vaccination planning, as referenced in Operation Warp Speed informational documents. 28
The availability of skilled vaccinators will likely pose the biggest challenge to mass vaccination operations for many jurisdictions. Community partnerships can support personnel, communication, and critical infrastructure for mass vaccination, but these partnerships require proactive and sustained efforts to develop and maintain. Jurisdictions could potentially draw personnel from neighboring regions for smaller outbreaks, but a large-scale pandemic or acute-onset outbreak may not provide this flexibility. Furthermore, legislation or executive orders expanding eligibility to administer vaccinations during an emergency, such as to dentists and emergency medical technicians, could further mitigate personnel limitations, particularly if this eligibility includes children. 29 Establishing these authorities in advance of an emergency can increase personnel availability and reduce operational delays, but executive orders, particularly those issued under emergency authority, can provide temporary authority in the absence of appropriate legislation. Finally, while establishing emergency surge capacity is important, incorporating vaccination training into onboarding and routine training for public health personnel, including nurses and immunization staff, can also help mitigate staffing shortages, particularly in situations with high staff turnover.
Accessing and vaccinating vulnerable populations will also likely pose significant challenges for many jurisdictions. Mass vaccination preparedness efforts should proactively identify relevant barriers to engaging these populations—including young children, pregnant women, immigrant or non-English-speaking populations, and those hardest to reach—and develop mechanisms to mitigate these barriers. Important considerations include specific skills and experience needed to vaccinate vulnerable populations and communication strategies to publicize locations of PODs and educate the public about vaccination operations and vaccine risks. Partnering with local community and volunteer organizations can be critical to establishing trusted relationships with vulnerable communities and responding to their unique needs. Additionally, certain mass vaccinating strategies, such as drive-through clinics, may be useful for particular populations, but they may also present additional challenges.
Funding constraints remain a major challenge for most jurisdictions and could be exacerbated during an emergency. Funding support is needed to purchase and maintain equipment and supply inventories, hire additional personnel, and conduct training, exercises, and community outreach. PHEP funds have historically been linked to anthrax preparedness, which has, to some degree, deemphasized mass vaccination at the local level. The 2019 PHEP update provides guidance regarding how federal preparedness funds can be used, including for purchasing vaccines, but the exclusion of certain activities from eligible vaccine purchases could potentially impact mass vaccination preparedness. PHEP funding can be used to purchase vaccines for certain populations, including for stockpiles for public health responders and their families and for critical workforce groups in exercises. Vaccines purchased with PHEP funds cannot, however, be used for the general public, including at seasonal influenza vaccination clinics or for anyone who qualifies for subsidized vaccines under another program (eg, Medicare/Medicaid, Vaccines for Children). 5 While Section 317 can provide vaccines for mass vaccination exercises and campaigns, it only funds vaccines for uninsured individuals, thereby limiting its use for such activities. 30 Most local operational vaccination experience is limited to seasonal influenza vaccination clinics and outbreak responses, so these circumstances could be a barrier to providing valuable mass vaccination experience at the local level. As with its overall impact, time is needed to evaluate how the updated PHEP guidance will be implemented and how state and local jurisdictions will use the associated funding.
As the United States and other countries look ahead to the availability of a SARS-CoV-2 vaccine, planning and preparations need to begin now, even if it may be months or longer before it is available. While a number of jurisdictions focused on more limited vaccination scenarios in their planning efforts, under the assumption that they were unlikely to need to rapidly vaccinate their entire population on a short timeline (eg, for a pandemic), the COVID-19 pandemic illustrates the importance of including larger events in vaccination plans. The vaccination capacity needed for COVID-19 will likely exceed the resources available at local and state health departments, so health officials should begin coordinating with other sources of vaccinators, including local health practitioners and systems, pharmacists, and medical schools. Additionally, COVID-19 is exhibiting a disproportionate impact on certain vulnerable populations, including older individuals and racial and ethnic minorities, so mass vaccination plans must ensure equitable allocation and access to the vaccine. A future SARS-CoV-2 vaccine will likely become available relatively slowly, over time, which aligns with both the assumptions outlined under the updated PHEP scenarios and those discussed by numerous interviewees. Jurisdictions will likely need to administer vaccinations to priority (eg, healthcare workers) and certain high-risk populations first, until sufficient vaccine can be made available to cover the entire population.
This study experienced several limitations. The updated PHEP funding requirements were published after most of the interviews were conducted, so it was not possible to assess the impact of these guidelines in addressing gaps identified in this study or the interviewees' perceptions of the finalized guidance. Many interviewees knew the guidance was forthcoming but expressed uncertainty and a lack of detailed familiarity regarding its content. We do highlight certain relevant changes to the PHEP program and note where they could have potential impact on these issues; however, a broad scope of logistical, administrative, and operational challenges described by the interviewees remain. Furthermore, while this study represented a range of experiences, most participating jurisdictions already identified mass vaccination as a priority, which could bias the results toward the experiences of more prepared jurisdictions. To mitigate these effects, we conducted a second round of recruitment explicitly designed to encourage participation from jurisdictions with less experience. Nevertheless, the study sample contains a higher proportion of jurisdictions with relatively stronger mass vaccination programs. Despite these limitations, we obtained diverse perspectives—representing a broad scope of capacities, geographic location, and jurisdiction size—and discussed a range of experiences, strengths, and constraints with respect to mass vaccination operations.
Conclusion
During a severe pandemic, timely mass vaccination could be necessary, but the rapid scale-up of mass vaccination operations remains challenging for many jurisdictions. Strong partnerships among government agencies, healthcare systems, and community organizations are critical to addressing these challenges. Increased attention toward mass vaccination at the federal level could help strengthen local preparedness efforts, but gaps remain in operationalizing mass vaccination at the local level. The explicit inclusion of mass vaccination planning assumptions and exercise requirements in the PHEP update is beneficial for addressing some of the existing operational barriers; however, the included pandemic influenza scenario may not fully address the capacity needed for other severe events requiring mass vaccination. The PHEP program update is a positive step forward, but additional time is required to evaluate the full effect of these changes.
Footnotes
Acknowledgments
We would like to acknowledge the funder for this study, the Open Philanthropy Project, and the jurisdictions that volunteered their time to provide insight and share their experiences. The authors declare no conflicts of interest.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.